Logic will help you get from point A to point B, imagination will help you get anywhere! Einstein
The most common questions we are asked by orthodontists around the world concern the shape of the arches and the sequence of their replacement.
This article will explain why we believe in Pitts Broad, a relatively new archwire design that provides the most esthetic solution in orthodontics today, and why the Pitts Broad archwire progression sequence is rational, effective, and simple. I have been working on the topic of arch shapes and arch sequences since my residency. During this time I have accumulated a lot of information. When I studied at the University of Washington from 1968 to 1970 under the tutelage of Drs. Richard Riedel and Alton Mohr, I was taught that to achieve stability, the shape and width of the arch should reflect the original shape of the dental arch before treatment. 35 years of collecting and processing information in the Department of Orthodontics at the University of Washington has led me to conclude that long-term stability is very unpredictable.
Picture 1:
The Evolution of Aesthetic Arch Shapes: A Preference for Pitts Broad Arches - Courtesy of Tom Pitts 2013
Figure 2:
Pitts Wide and Utility Arc Comparisons - Courtesy of Tom Pitts 2013
“Orthodontic treatment is inherently unstable and without retention, relapse is inevitable.”
Because of these advances, my clinical experience, and the clinical experience of the thousands of orthodontists I have taught and interacted with throughout my career, I believe in lifelong sleep retention after orthodontic treatment is completed.
Figure 3:
Aesthetic changes associated with changes in archwire shape due to the application of curves to corrective archwires - Courtesy of Tom Pitts 2013
Almost immediately after graduating from university in 1970, I attended the first FACE continuum, where I studied with Dr. Ron Roth. Dr. Roth imagined an arch in the shape of a horse's hoof, very wide at the front. Using this archwire for some time, I realized that treating clinical cases with archwires that are too wide and flat anteriorly and too narrow in the molar area does not create an aesthetically acceptable effect in the final phase of treatment.
Later, a group of innovative orthodontists with whom I collaborated (the A company Innovation Group) developed an arch shape that is sometimes called the Universal or Damon arch shape. This archwire shape has been consistently adopted by many orthodontists around the world and has proven to achieve more esthetic results than previous archwire shapes. I used the Universal and Damon arcs for many years and for me, it was still not enough.
Figure 4:
Aesthetic shapes are obtained by applying curves to the arches and become the basis for the wide Pitz arches (without distalizing the molars) - with permission from Tom Pitts 2013
During the treatment of patients, insufficient width in the posterior region was observed and further treatment with bends on the arches was required. The duration of such treatment from the stage of nickel-titanium arches to the stage of using corrective arches (TMA or stainless steel arches), where further alignment in the posterior area depends on the bends in the arch, takes from eight months to a year. This is effective, but not rational.
Figure 5:
The aesthetic goal is a wider smile, not too wide at the canine area, a delightful smile arc, full enamel alignment when smiling and optimal incisor inclination - courtesy of Duncan Brown
When I participated in the continuum of Dr. Robert Ricketts in 1975, I began to evaluate the treatment results achieved in terms of the aesthetics of the arch shape, offering less width at the canine site and greater width at the molar site. This arch shape resulted in a very aesthetic smile with a decrease in the space of the buccal corridors. I began to inherit this shape with the help of corrective archwires, gradually increasing the width in the molar area to maximize the filling of the buccal corridors with teeth. (Figures 1–3). The result is a reflection of modern concepts of dentistry, when the disposition of 12 teeth during a smile is considered the most aesthetic.
Figure 6:
Width and shape of the arch varies according to aesthetic purposes - courtesy of Duncan Brown 2016
Obviously, some “thinking outside the box” should, in turn, give impetus to the development of an entire system (bracket geometry, archwire shape, archwire sequence) that is rational, effective, easy to use, easy to teach, and allows the orthodontist to consistently achieve exceptionally aesthetic results . Fortunately, OS Orthodontics' corporate culture always strives for significant innovation.
Figure 7:
Aesthetic changes associated with a change in the shape of the dental arch created using a corrective arch – courtesy of Tom Pitts 2013
Arch shape and today's aesthetic and functional expectations:
Today I talk and show photographs of ideal smile aesthetics to potential patients. They readily appreciate the aesthetic value of full lips, wide smiles, a well-defined smile arc, fullness of the maxillary teeth during smiling, and optimal inclination of the incisors for aesthetic reasons. Inevitably they will all say, “I want this.” Anticipated age-related changes in the face during aging should be considered in the treatment plan as an initial goal and not as an additional idea. (Figures 4–9).
Figure 8:
The aesthetically directed arch shape created by applying curves became the basis of the Pitts broad arch – courtesy of Tom Pitts 2013
There is an increasing number of fans of non-excision treatments to satisfy aesthetic needs around the world. Unfortunately, for many, the biomechanics of non-extraction treatment are often associated with the need to control proclination of the upper anterior teeth while addressing crowding. As we mentioned in the previous version of the protocol, control of axial tilt can be achieved using active early protocols by rotating the H4 brackets 180°. For more information regarding active early protocols, see the overview on this topic in this article and also in Section 2 - Protocol.
Figure 9:
Aesthetics achieved with a wide arc according to Pitts Pitts broad creates “Wow!” smiles – courtesy of Nimet Guiga 2016
For many years, at the same time as widening the buccal segments to control anterior axial tilt in non-extraction cases with potential for proclination, I have flipped the upper anterior brackets. Another challenge to expanding premolars and molars with a fixed appliance is that the axial inclination of the buccal segments must be controlled. Even though we use brackets with a torque of -27 degrees on the upper molars and -22 degrees on the lower molars, sometimes during expansion in the posterior region, we add a little torsional moment to the arch.
Figure 10:
A wide smile, remarkable smile curvature and full enamel alignment during smiling become critical in patients with small teeth - Courtesy of Duncan Brown 2016
Our searches confirmed that the final arch width is a function of the arch shape rather than the brackets used during treatment. In response to the need for an improved arch shape that is wide in the molar region (to fill the buccal corridors), narrow in the anterior region (for better incisor expression), and slightly narrower than traditional arch forms in the canine and first premolar region (for better positioning 12 -ty teeth while smiling) I invented the wide arch shape according to Pitts Broad. For most patients, this arch shape creates a 12-tooth smile. I worked with OS engineers to design all the arcs I use, both the Pitts Broad and the universal ones. Beginning treatment with Pitts Broad Thermo-Active Nickel Titanium (TA NiTi) wires can achieve very rapid expansion and are part of an early active protocol.
Figure 11:
The aesthetic goal of optimal incisor angulation - Courtesy of Duncan Brown 2016
In dental aesthetic circles, the aesthetic concepts of the “Golden Proportions” have been very successfully supplanted by the concept of “Virtual Crown Width”. This refers to a description of the visual expression of aesthetically straight teeth and we adhere to this concept. For us, transverse expansion does not depend on the size of the teeth or whether the treatment is extraction, since it is a separate form of the arch, which must meet aesthetic requirements and biological possibilities. We reject the concept that patients with reduced overall tooth size (after extractions or reduced mesiodistal width of anterior teeth) should be treated with narrow arch forms. In my opinion, the shape of the arch is more important for aesthetics than the proportions of the sizes of the anterior teeth among themselves (Figures 10–15).
Figure 12:
Width and shape of the arch varies according to aesthetic purposes - courtesy of Duncan Brown 2016
Caution should be exercised when expanding premolar and molar sites in patients with a thin periodontal biotype. We refer to the concept proposed by Dr. Michael Mejore (Edmonton, Alberta) of continually assessing the patient's biological limitations to achieve the desired tooth movements. In patients with a thin biotype, thin labial/buccal/lingual bone at the level of the root endings, or in patients with bone fenestration already present, I modify the arch shape, do a very slight widening, and palpate the labial and lingual sides at each visit. This is a direct compromise when established biological limitations exceed aesthetic requirements.
Figure 13
As already mentioned, achieving transverse expansion of the area of canines, premolars and molars is very effective on round thermoactive arches. OS provides a full range of arches of different sizes and sections, and already at the initial stage it is possible to achieve the desired shape of the dental arch, which previously could be achieved by applying bends to the corrective arch. OS offers the following archwire shapes (Figure 1): Pitts Broad (which we use most often), Pitts Standard (we use less frequently), and Universal (for patients with biological limitations or for wide lower arches and low values). torque).
Figure 14
The use of beta titanium or stainless steel wires allows subtle adjustments to be made in the final arch shape to suit aesthetic requirements, biological limitations and minor torque corrections. In Active Early treatment, where torsional control and lateral expansion of the archwire is achieved early in treatment, stainless steel archwires will be required less frequently, but are available for those who enjoy using them
Application of a facebow in prosthetic dentistry
Orthopedic dentists use different tools in their daily practice, one of them is the facebow. It is used in combination with an articulator.
Using an arch, the relationship between the upper jaw and the patient's skull is determined and transferred to the articulator. The dentition of the upper jaw is oriented relative to the temporal joint of the lower jaw.
Using these orthopedic devices, the dentist accurately simulates the movements of the lower jaw.
Face bow design
It consists of several elements: a main frame in the shape of the letter U, a bite fork, stops (ear or articular, as well as nasal), a transition device between the frame and the fork, and a plane indicator.
The frame (arch) goes from the temporal joints of the lower jaws to the central upper incisors. The device moves 2–3 cm away from the skin.
of supports - ear and joint. The first come into contact with the skin in the area of the external auditory canals, the second - in the area of the temporal joints of the upper jaw.
The bite fork is attached to the dentition.
Functions of an orthopedic arch
Using the device, orthopedic dentists perform spatial modeling and:
- The occlusal planes are aligned;
- The location of the dentition at rest and in motion is conveyed with high accuracy;
- A perfectly fitted prosthesis is made.
It takes no more than 2 minutes to measure.
Types of face bows
There are two types of instruments: average anatomical and kinematic.
The mid-anatomical or portable arch is a standard device that is attached to the patient’s head using stops (nasal or temporal) at the point of the axis of rotation of the condyles. Next, a bite pad with impression material is attached to the device and placed in the patient’s mouth. The structure is fastened with screws and the device is adjusted to obtain an accurate model.
An arch of this type is used if the patient is missing all his teeth - it is used to make removable dentures.
The kinematic or axial arc is fixed on the chin and forehead. It measures how the jaws and axes relate as they move.
This type of archwire is used in the manufacture of elastic and partial dentures.
How to work with an arc: 3 ways
The device is not an alternative to other prosthetic procedures, such as taking impressions, measuring jaw relationships and measuring centric occlusion. It is used as an additional procedure in the manufacture of a prosthesis. There are 3 ways to use a facebow. Let's look at each of them.
1st method: installation at the point of rotation of the condyle
For a mid-anatomical joint transfer, follow these steps:
- Find the center of rotation of the condyle. Guide yourself along the line that connects the outer corner of the eye and the apex of the tragus of the ear, approximately 1.3 cm anterior to the external auditory canal;
- Place the joint stop at the found point.
This way you will determine the real axis of rotation of the mandibular condyle with an error of 0.2 cm.
Method 2: the easiest installation
This is the simplest method, therefore the most popular. The main feature is that the arch and articulator must have sockets for fixing the arch, both from the external auditory canal and the joint.
It is important that the distance between the nests is strictly 1.3 cm.
The easiest way to install the arch is along the external auditory canal. To do this, fix the bite fork on the dentition of the upper jaw.
The use of an average anatomical arch gives an approximate transfer of the position of the upper jaw and the axis of rotation of the lower jaw.
Using an axial arc will result in more accurate results.
3rd method: using an axial arc
It is necessary to find the central position of the articular head in the joint, which ensures the central relationship of the jaws.
Use axial arc:
- Fix it on the dentition of the lower jaw;
- Ask the patient to move the jaw back and forth and open and close;
- At the same time, notice how the tip of the joint stop moves;
- Determine the axis of rotation of the lower jaw. Record when the stop indicators begin to rotate around their axis when the mouth opens 2.5 mm. This will be the axis of rotation of the lower jaw;
- Mark it on the skin with a dot;
- Transfer the upper jaw model.
The procedure is performed in the same way as we described in method 1.
Advantages of the device
The tool eliminates erroneous orientation when forming the occlusion of the model and prosthesis. This is its main advantage.
The device allows:
- Quickly, simply and accurately identify all the nuances of the jaw relationship;
- To produce high-quality prostheses - accurate and aesthetic;
- To make prostheses taking into account all the anatomical features of the patient.
- If an orthopedic dentist works with a facebow, patients also benefit:
- Save time. There is no need to visit an orthopedist for additional measurements and adjustment of the prosthesis;
- Easy adaptation. A perfectly fitted prosthesis does not take long to get used to. The adaptation period is as comfortable as possible: without pain, discomfort, rubbing, etc.;
- Rapid restoration of chewing functions;
- Durability of dentures. The load on the dentures is distributed evenly, so they will last a very long time.
Thanks to high-quality dentures, the patient’s crowns and “natural” teeth do not wear out longer.
Consequences of not using an arc
If the dentist does not use a facebow, he risks making gross errors in the manufacture of prostheses due to incorrect orientation of the models in the articulator and determination of occlusion.
Here are the most common mistakes dentists make:
- Incorrect spatial location of the upper jaw model in the articulator. The cusps of the upper jaw should correspond to the movements of the lower jaw. This is possible with their tilt angle of 35 degrees, which can be achieved using a face bow. If the device is not used, the angle of inclination will be greater - the bumps may chip.
- Discrepancy between the patient’s real occlusal paths and those on the model. If a facebow is not used, these paths will not correspond to each other, as a result of which the cusps of the lateral molars on the denture may chip.
Thus, in modern prosthetic dentistry, to produce high-quality restorations, it is advisable to use a facebow in combination with an articulator.
Working with arc shape and arc sequence:
In Active Early protocols, the device is activated as early as possible. To do this, brackets are positioned using the Smile Arc Protection (SAP) method to correct the position of the incisors in the vertical plane, brackets are turned over if necessary to activate the torsional moment, a sequence of arches is selected to control axial inclination in the early stages of treatment, arch shapes are used for earlier expansion of the posterior segments, Early Light Short Elastics (ELSE) for force control and appropriate disarticulation to achieve early “desired” tooth movements, as well as extrusion or intrusion.
In contrast to traditional “straight arc thinking,” where forces for torsional correction or lateral expansion are applied for short periods of time late in treatment, the Active Early approach involves using smaller forces for longer periods of time in early stages of treatment.
Figure 15:
Aesthetic goal using Pitz's "Active Early" protocol to control axial tilt early in treatment in a well-cooperative patient - courtesy of Duncan Brown 2014
The Pitts archwire sequence is specifically designed to combine the aesthetically optimized Pitts Broad wires, the reduced buccolingual slot dimensions of the H4 OS brackets, and the early Pitts protocols.
Stage 1 – Arch expansion and torsional moment in uncorrected arches
In the past, the recommended archwire sequence for passive self-ligating brackets involved the use of low forces with long intervals between visits to expand the arch laterally while controlling axial inclination with uncorrected archwires early in treatment. This approach is still relevant in cases of severe crowding, and the H4 brackets, with their shorter depth and more precise groove characteristics, offer more treatment options.
The goal of early active protocols using the Pitts archwire sequence is to move to a .020 x .020" thermally active archwire as quickly as possible to simultaneously achieve transverse extension (with Pitts broad archwires) and control anterior axial tilt (due to torsional moment in the groove).
Dr. Ricketts stated that the square archwire is as gentle and effective in achieving torsional torque as the rectangular archwire. This is confirmed by scientific research. Control of dental arch expansion and anterior axial inclination is maintained in the early stages of treatment through the use of lightweight short elastics, byte turbos and other elements of the Active Early approach from the first visit. We prefer to see patients every 6 weeks for the first three visits, during which time a .020 x .020″ thermally active wire is used.
Figure 16:
Most cases start with a thermoset .014" NiTi or thermoset .018 x .018" UltraSoft NiTi (in cases of minor crowding or rotation). Each of these arcs is present in the Pitz wide form. In cases where treatment begins with a .014 NiTi thermally active wire, patients return 6 weeks after fixation, after which the wire is changed to .018 x .018" Ultra Soft Niti for 6 weeks. The goal is to reach the thermoactive .020 x .020" NiTi arch over a period of 6 to 12 weeks and thus trigger a torsional moment developing inside the groove through the arch simultaneously with the continued expansion of the dentition. Square arches work well in place of rectangular arches. Arch .018 x .018 Ultra Soft NiTi is a new arch that we developed at OS.
Figure 17:
For patients who have difficulty eliminating rotations, we suggest replacing the .020 x .020 thermoactive NiTi archwire with a .018 x .025 thermoactive NiTi archwire. With a .025 archwire in the H4 .026 bracket slot, rotation correction is easily achieved with correct bracket positioning.
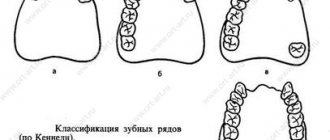
Malocclusion
The position of the dental arches relative to the central occlusion in dental practice is called occlusion. In medical practice, there are two types of occlusions – physiological and abnormal. The first type is characterized by the fact that the upper row of teeth covers the lower one. In the presence of an abnormal bite, the relationship between the upper and lower arches is disrupted. In total, there are 4 malocclusions:
- open;
- cross;
- distal;
- mesial;
- deep bite
Stage 2 – Torsion moment and shape correction in corrective arches
During the treatment phase with corrective arches, there are several alternatives: Without rotation: in cases with slight or minimal rotation, it is usually possible to achieve results with .020 x .020 beta titanium arches. This arch can be easily adjusted to individual aesthetic shape and correction of axial inclination of a single tooth. Clinicians should expect second-order bends, but axial tilt should be achieved (Figures 16–19).
Figure 18:
In the second stage, the clinician should expect to need to apply second order bends to the .020 x .020 archwires - Courtesy of Duncan Brown 2016
With rotations: In cases where rotational control is required, moving to a .025 arc is highly desirable. Since the torsional moment is present in the groove for some time, the axial tilt must be very well controlled for the following reasons:
- We prefer to transition from .020 x .020 thermoactive NiTi wires to .018 x .025 thermoactive NiTi wires in these patients, with corrective beta titanium wires .017 x .025 or .019 x .025 providing a similar finish for the most experienced passive user self-ligating braces.
- With inverted upper anterior brackets (either lateral incisor to lateral incisor or canine to canine), the .017 x .025 beta titanium archwire presents optimal torsional and rotational forces. We found out that arcs larger than these are simply not needed.
- In cases where greater torsional torque correction is needed, thermoactive .021 x .025 NiTi archwires are a good alternative, followed by .019 x .025 or .017 x .025 beta titanium for finishing
Thermoactive arc NiTi Ultra Soft .018 x .018 is a real breakthrough in technology. We begin treatment of many cases with this arch even when we include the second molars in treatment at the first visit. Very often after 6 weeks we change this arc to a thermoactive NiTi .020 x .020. In cases where more rotational control is required, thermoset NiTi .018 x .025 can be used before beta titanium .017 x .025.
Figure 19:
Good torsional moment control is present when flipping upper anterior brackets and canines with a .020 x .020 beta titanium archwire – courtesy of Duncan Brown 2016
Due to the greater compliance of H4 brackets, many clinicians are able to save several months of finishing time compared to previous passive self-ligating brackets by using the archwire sequence described above (Figure 20). We use thermoactive NiTi, not super-elastic NiTi, in all arc sequences.
Figure 20:
Simple Sequence for Changing Archwires Using .022 x .026 H4 Brackets - Courtesy of Tom Peetz
Don't clinicians want more effective, rational and simpler treatment mechanics? As we work with OS, we will always continue to introduce innovations that positively impact orthodontics, mainly from a sustainability perspective. Follow our innovations!
To sum it up:
Our goals in orthodontics are dictated by the aesthetics of “Wow!” and are designed to compensate or counteract the effects of aging. For many orthodontists, such goals provide a new context for their treatment plan and clinical protocols. The boundaries of treatment are constantly expanding. Remaining competitive in an aesthetically oriented professional environment is a real challenge. Pitts Broad, combined with H4 brackets and Active Early protocols, offers new tools to simplify your life while improving patient outcomes.
We invite you to join the Pitts Global Masters continuum beginning March 23, 2022. This continuum is divided into four parts over two years. We are planning even more innovations! It's good that you are with us!
Until next time...
Doctors Tom Pitts and Duncan Brown.
Reasons for changing the arc
Dental defects can be the result of many unfavorable factors. The formation of arches is influenced primarily by heredity. Also, anomalies can result from various formation disorders during embryonic development. Other reasons due to which the upper and lower dentition may be deformed:
- trauma to the maxillofacial area (impact, fall);
- inferiority of the temporomandibular joint;
- presence of bad habits in childhood;
- the presence of some systemic pathologies that affect the condition of the bone tissue in the jaw, etc.
Regardless of what caused the dental anomalies to develop, it is important not to let the disease take its course, but to contact a dental clinic for advice and the development of a treatment plan.