Summary
Breakage of nickel-titanium instruments is a major problem in endodontic treatment. A study examining the failure of nickel-titanium files due to torsional loading found that the majority of such failures occurred at the tip of the tool within the last millimeter and in instruments that had a small taper and/or size. Consequently, the tip of small instruments is at higher risk of breakage due to torsional loading, and to prevent this, the use of torque-reducing motors is necessary to reduce apical pressure and prevent the instrument tip from becoming stuck in the root dentin. In contrast, flexural fracture occurs as a result of repeated subthreshold loading resulting in metal fatigue. Numerous studies examining the causes of overload and breakage of machine-assisted nickel-titanium files have confirmed that by pre-expanding the root canal using hand instruments and creating a glide path before using machine instruments, a significant reduction in the rate of breakage can be achieved. This fact highlights the importance of manually pre-expanding the root canal and creating a “glide path” to reduce the incidence of mechanical instrument failure. To pre-expand the root canal and create a “carpet path,” hand-held steel instruments are most often used. Unfortunately, they have a number of disadvantages due to their relative rigidity and the presence of an aggressive tip, which can lead to the formation of ledges or changes in the course of the root canal in curved and/or calcified canals. For this reason, a new PathFile™ (Dentsply Maillefer) set for glide path creation and root canal pre-expansion was recently introduced, consisting of three machine-made nickel-titanium instruments.
PathFile™ are the first instruments specifically designed and intended for the mechanical creation of carpet and pre-enlargement of the root canal. The combination of a low 2% taper, a square cross-section and 4 cutting edges makes these instruments highly flexible, durable and effective, enabling fast and safe treatment of even severely curved and/or calcified root canals. Preliminary scientific research and clinical trials have confirmed that PathFile™ instruments are highly effective in treating severely curved root canals, allowing the creation of a perfect “glide path” without altering the course of the root canal, even if the working length is incorrectly determined.
Introduction
The use of machine-made nickel-titanium instruments has radically changed the technique of mechanical root canal preparation and the prognosis in difficult clinical situations. Numerous “invitro”1−13 and “invivo”14−17 studies have shown that machine-made nickel-titanium instruments are superior to steel hand files in the quality of root canal formation and the possibility of their use in canals with pronounced curvature, reducing the risk of creating ledges or straightening the canal curvature . Schäfer16 conducted an in vivo study in which 110 root canals were treated with machine nickel-titanium instruments and 84 canals with hand instruments. All canals were processed by 8 experienced doctors. Before the start of treatment and after obturation of the canals, x-rays of each tooth were taken.
Straightening the curvature. Nickel-titanium machine tools.
Work time. Manual steel files.
Rice. 1. Probability of root canal straightening and working time after in vivo root canal debridement using nickel titanium machine tools and hand steel files (adapted from Schäfer et al.16).
Straightening of the root canal curvature was assessed using a computer image analysis program. Root canal preparation using machine-assisted nickel-titanium instruments significantly reduced working time and resulted in less straightening of the canal curvature compared to the use of hand instruments16 (Fig. 1). In another in vivo study, Sonntag et al17 compared the risk of complications in root canal preparation with hand-held steel instruments and machine-operated nickel-titanium instruments. All clinical cases were performed by students. The results demonstrated that even in the absence of sufficient experience on the part of the practitioner, the quality of root canal preparation using nickel-titanium instruments was higher than that using manual steel files, while the number of shoulders was significantly reduced and the integrity of the apical foramen was maintained.17 Unfortunately, the use machine-made nickel-titanium instruments have serious limitations as they are associated with an increased likelihood of file breakage within the canal compared with steel instruments.17,18 Suter et al. When assessing in vivo the possibility of successfully removing a broken instrument from a root canal, success rates are reported to be 87% of cases. Studies of removed instrument fragments confirm that machine-made nickel-titanium instruments break more frequently than hand-operated steel instruments.18 Sonntag et al.16 report that breakage of nickel-titanium instruments is a major problem in endodontic treatment. Studies evaluating the influence of various factors on the breakage of machine endodontic nickel-titanium instruments have demonstrated that file breakage occurs primarily under the influence of torsional load19−25 and instrument fatigue.21,23,26−28 Torsional load depends on the contact area of the instrument with root canal dentin, the taper and diameter of the instrument, the area of the instrument subjected to stress, the strength (cross-sectional shape) of the instrument, the design of the working part, and the torsional load applied to the instrument.27,28 A study on the failure of nickel-titanium files due to torsional load has shown that the majority of such failures occur at the tip of the tool within the last millimeter and for instruments that have a small taper and/or size.24,25,27,28 Consequently, the tip of small-sized instruments is at higher risk of failure due to torsional loading, and to prevent this, the use of torque-reducing motors is necessary to reduce apical pressure and prevent the instrument tip from becoming stuck in the root dentin.27,28 In contrast, flexural fracture occurs as a result of repeated subthreshold loading, resulting in metal fatigue.
The bending load depends on the radius of curvature and size of the root canal, the rotational speed and flexibility of the instrument, the characteristics of the nickel-titanium alloy, the presence of intracanal obstructions, and sudden changes in the course of the root canal (for example, in the case of fusion of canals or the presence of additional canals).27,28 Numerous Studies examining the causes of overloading and failure of machine-assisted nickel-titanium instruments have confirmed that a significant reduction in the incidence of machine instrumentation failure can be achieved by pre-enlarging the root canal using hand files and creating a “glide path” before using machine instruments. In a study of the effect of pre-enlargement of the root canal on the failure rate of 4% taper nickel-titanium machine instruments, Roland et al.29 concluded that “pre-enlargement of the root canal with hand files followed by the use of machine instruments allows the instruments to be used more times before failure than with the isolated use of the crown down technique recommended by the manufacturer.” Peters et al.,30 examining the physical performance of machined nickel-titanium ProTaper instruments in the treatment of curved maxillary molar canals “in vitro”, showed that “even when significant load was applied in some clinical cases, no ProTaper instrument failed in the presence of adequate "carpet path" Blum et al.31, after analyzing the mechanical preparation of extracted teeth using ProTaper machine instruments, determined that “particular attention in a precise root canal protocol should be given to the use of small, flexible hand-held steel files to ensure that each part of the root canal has sufficient space for unobstructed machine access.” tools in the process of further machining...". Berutti et al32 evaluated the effect of manual root canal pre-expansion and torque on failure rates using ProTaper machine instruments. In this study, the authors used 400 plastic training blocks divided into 2 groups. All blocks were processed with ProTaper instruments, but one group had the canal pre-dilated manually using hand instruments to ISO #20 before using machine files. The results of the study showed that after manually pre-expanding the root canal, ProTaper instruments were able to process significantly more plastic blocks before failure occurred32 (Figure 2).
Rice. 2.
Number of plastic training blocks processed to failure by ProTaper S1, without pre-expanding the canal to a #20 ISO file and with pre-expansion. Adapted from Berutti et al.32 No pre-expansion. Pre-extension to ISO file #20.
Finally, Varela et al33 examined the effect of manual canal pre-expansion on the failure rate of three different nickel-titanium machine instruments (ProFile, ProTaper and K3) when used in canals of extracted teeth with curvature greater than 30º. The authors demonstrated a significant reduction in the incidence of file breakage when performing preliminary manual root canal expansion before using machine instruments. In this study, there were no significant differences between the three types of instruments used.33 All of the above studies suggest that the beneficial effect of pre-manual reaming is to reduce the likelihood of the tip of the weakest instruments becoming stuck in the root canal.28−33 In addition, As an explanation for the reduction in machine instrument failure in curved root canals, not only the presence of a smooth “carpet path” to prevent dangerous deformation of the instrument tip must be taken into account, but also the reduction in bending load.28,30,32
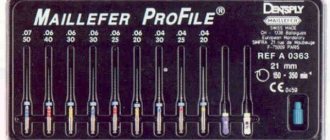
Preliminary enlargement of the root canal and creation of a “carpet path” is most often carried out using manual steel files. Unfortunately, these instruments have a number of disadvantages due to their relative rigidity and the presence of an aggressive tip, which in curved and/or calcified canals can lead to the formation of a shoulder or change in the course of the root canal.34 For this reason, the new PathFile™ set was recently introduced (Dentsply Maillefer) for creating a “carpet path” and preliminary expansion of the root canal, consisting of three machine-made nickel-titanium instruments.
Rice. 3.
PathFile™ No. 1−3 (Dentsply Maillefer). PathFile™ No. 1 (0.13 mm). PathFile™ No. 2 (0.16 mm). PathFile™ No. 3 (0.19 mm).
Endodontic instruments Part 2
Profile Orifice Shapers (profile orifice shaper) - a set of tools made of nickel-titanium alloy with a blunt tip and a taper of 5-8%.
The tool comes in 6 diameters (1-6). The length of the cutting surface is 10 mm. Designed for processing the coronal part of the root canal. The advantage over Gates Gliden, used to widen the mouth of canals, is that, by expanding the coronal part to the first bend, it creates a transition in the form of a cone into deeper parts of the canal. Marked with 3 colored rings on the shank (Fig. 5-8). Profile O is available in 6 sizes 015, 020, 025, 030, 035, 040 with a working length of 21 and 25 mm. The length of the cutting surface is 16 mm, the working part is 21 and 25 mm. Marked with 2 colored rings on the shank.
Profile 04 is available in 9 sizes 015, 020. 025, 030, 035, 040, 045, 060, 090 with working lengths of 21, 25 and 31 mm. Designed for processing the apical part of the canal. Marked with 1 colored ring. In addition, the set includes profiles 08 and 015 for manual work.
Rice. 5-8. Profiles with increasing taper: orifice shaper, profile 06, profile 04, compared to profile 02
Profiles 04 and 06 are designed for handpiece operation at optimal speeds of up to 300 rpm.
Profiles have 4 features that distinguish them from other tools. First, they are made of nickel-titanium alloy, which gives them super-ductility, allowing them to process canals with bends of up to 90° (Fig. 5-9). Secondly, the profiles have a pronounced narrowing towards the top of the tool (Fig. 5-10). This allows you to use the tool more efficiently. A tool with a 2% taper, when penetrating the canal, comes into contact throughout its entire length with the wall (left), and a tool with a 4% or 6% taper, penetrating into the canal, comes into contact in a limited area (right) (Fig. 5-11).
Rice. 5-9. Superplasticity of the profile
Rice. 5-10. The shape of the root canal depending on the taper of the instrument (diagram). Figure 5-11. Borders of contacts between an instrument of increased taper and the walls of the root canal (diagram).
Rice. 5-12. Cross section of the profile. V-shaped side grooves (in the center), unlike other tools. ensures the removal of dentinal filings from the canal.
The third feature of the profiles is the U-shaped cross-section (Fig. 5-12) without pronounced cutting edges, which makes it possible to remove sawdust from the root canal. The fourth feature of the profile is the modified tip (blunt), which allows the tool to penetrate any curved canal.
A new direction in the creation of cutting endodontic instruments is to increase the taper, compared to the original ISO standard, by 2-6 times, i.e. instead of 2% - 4, 6, 8, 10 and 12%.
Greater Taper (GT) Rotary files (Figure 5-13). These new generation nickel-titanium endodontic instruments are perfectly adapted for root canal preparation using the Crown Down technique. Like Profiles, Greater Tapers are designed to operate in a clockwise rotating mode at 150-350 rpm using any suitable machine tip. These instruments are marked with gold-plated shanks.
Rice. 5-13. Greater Taper Set.
The set of rotating GTI files consists of 3 groups of tools.
The first group consists of 4 instruments with a taper of 12, 10, 08 and 06% with the same tip diameter 020 and lengths of 21 and 25 mm. This is the main group of instruments used for preparation using the Crown Down method. When preparing a canal, they first work with a file with a large taper and successively move on to an instrument with the smallest taper (6%).
The second group, also consisting of 4 instruments with a taper of 04%, tip diameters of 020, 025, 030 and 035 and lengths of 21, 25 and 31 mm, is intended for preparing the apical part of the canal. The smooth, flat outer edges of GI rotating U-shaped files prevent self-cutting of the instrument and ensure that the file is centered in the canal.
The third group consists of 3 instruments with a taper of 12%, tip diameters 035, 050 and 070 and lengths of 21 and 25 mm, they are intended for opening the canal orifices.
Using GI rotating files with different tapers, almost all root canals are successfully prepared. The largest size of the instrument tip (020 mm) and the maximum shaft diameter of 1 mm guarantee non-aggressive preparation of the apical part without disturbing the anatomy. As can be seen in the presented diagram (Fig. 5-14), each subsequent tool comes into contact with the channel wall only on a limited part of its length, which eliminates the possibility of jamming and, consequently, tool breakage.
Rice. 5-14. Root canal preparation using instruments with different tapers (diagram).
Tools should be cleaned after each use as cutting performance is reduced when the shank grooves are full. During preparation, abundant irrigation of the root canal is necessary.
PathFile™ Tools Sequence
The sequence of using PathFile™ tools is very simple (Fig. 4):
1 – Primary navigation and examination of the root canal with a K-file No. 10, which should freely enter the canal to the working length. To speed up this stage, if necessary, use endolubricants containing EDTA.
2 – Determination of working length using an electronic apex locator and (or) radiography.
3 – Pass PathFile™ No. 1 (0.13 mm) to working length.
4 – Pass PathFile™ No. 2 (0.16 mm) to working length.
5 – Pass PathFile™ No. 3 (0.19 mm) to working length.
6 – You can then begin using the nickel titanium files using standard techniques (if using the ProTaper system, use file S1).
PathFile™ are used in a gentle reciprocating motion at 300 rpm, motor torque of approximately 5 Ncm until full working length is reached. Significant apical loading on instruments should be avoided. The use of relatively high motor torque is not harmful given the square cross-section of the tool and the results of a study by Berutti et al.38 which demonstrates that the use of high torque allows nickel-titanium machine tools to machine significantly more channels before failure.38 The time required to work with three PathFile™ files per working length does not exceed 3 – 5 seconds for each tool; increasing the working time is useless, but not dangerous, since PathFile™, thanks to their high flexibility, do not change the course of the canal even in the event of errors in determining the working length. Copious irrigation is recommended after each instrument, although PathFile™ coils do not become clogged with dentinal filings and these instruments do not cause filing blockage of the apical foramen.
Rice. 4.
Sequence of using PathFile™ tools. X-ray before treatment (4A). Determination of the working length of the palatal and medial buccal 1 canals (4D). Radiograph showing the master pin in the medial buccal 1 and medial buccal 2 (4E), and in the distal and palatal canals (4F). X-ray immediately after treatment (4G) and 1 year later (4H).
Canal-Leader 2000 from SET
Although we advocate manual work within the dental cavity, progress in the development of new endodontic approaches, both in terms of filling (Thermafil system) and root canal instrumentation, is leading to the emergence of new treatment techniques. Among them, a special place is occupied by the Canal-Leader 2000 endodontic contra-angle handpiece, developed and offered by SET. It is necessary to emphasize that we are talking not only about the tip itself, but about the endodontic treatment system. Micro instruments from SET are mated to the Canal-Leader 2000 handpiece.
These include:
1. Canal expander “K”, for probing narrow root canals.
2. Universal canal expander for probing and treatment of root canals.
3. Channel expander “H” (Hedstrom), for processing channels and removing old material.
4. Gutta-percha sealant.
5. Channel fillers.
Recommended tool rotation speeds (in rpm):
· for channel expander “K” – 2000 – 4000,
· for universal channel expander and channel expander “H” (Hedstrom) - 4000-6500,
· for gutta-percha sealant and canal filler – 5000 – 6500.
Since the Canal-Leader system is multifunctional, it can be used to carry out all stages of endodontic treatment.
The endodontic handpiece operates at a speed reduction of 4:1. This means that, for example, at a tool rotation speed of 2000, the micromotor rotation speed should be 8000 rpm, i.e. the number of revolutions is multiplied by 4.
The instrument in the endodontic handpiece makes translational and rotational movements. With each rotational movement of 200, a translational movement of 0.4 - 0.8 mm is provided. The tip can operate in various speed modes, which are selected taking into account the anatomical features of the tooth.
Microtools have codes, according to ISO classification, from 08 to 40. They are used in accordance with the requirements adopted for the now classic “Step-Back” technique. The choice and sequence of use of canal expanders is determined by the diameter of the canal. In this case, depending on the patency of the canal, probing and treatment usually begin with a universal canal expander, size 15. This is a modified Handstrom file with a special rounded end. We already emphasized at the beginning of the book that the major changes made to endodontic instruments are primarily related to the tip of the instrument. These changes ensure relative safety of work and eliminate the possibility of formation of ledges and perforations of the walls of the root canals. At the same time, these instruments do not exclude the possibility of expanding the apical constriction and, thus, periodontal injury.
To do this, according to the general requirements of endodontics, the working length of the root canal must be carefully determined. The company does not recommend developing root canal orifices using, for example, a Gates-glidden bur if the retractor entered the canal no less than 3 mm. In this case, probing of the canal is carried out at speeds of 4000 - 6500 per minute, with up and down movements, until the expected (fixed with a rubber clamp) apical constriction, with light vertical pressure.
In narrow canals, probing should be carried out with a canal expander "K" 08 or 10. The number of revolutions should be reduced to 2000 - 4000. The operating time should not exceed 10 seconds, with constant washing of the canal or using a gel to expand the canals. It is necessary to take into account that the mouths of the root canals must also be widened with a Gates-glidden bur.
After probing the root canal, it is continued to be processed in all directions with universal canal expanders. The goals and objectives are identical to manual processing, and, accordingly, the sequence of using tools must be followed according to the schemes proposed in the description of the “Step Back” technique. The final size of the canal expanders in each tooth will vary, their recommended sizes are 25 - 40. If work started with a canal expander 15, then 20, 25, 30, 40 are used sequentially. In some cases, the Crown Dawn technique can be recommended, in which the mouth part is expanded with a larger instrument size (so that it enters the root canal by 3 mm without bending), gradually moving to instruments of smaller diameter so that the apical part is developed with instruments 25 - 40.
The Canal-Leader kit from SET includes a flow-through rinsing system, as well as rinsing tablets. All work must be carried out with constant irrigation. Once the canal is fully dilated, the canal is washed and dried using sterile paper points.
In addition, using the Canal-Leader system, you can condense gutta-percha in the root canal and add filling material as a canal filler.