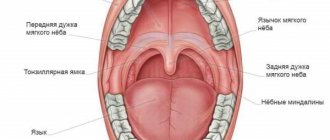
Occlusion form
The shape of the bite can be determined by knowing the size and height of each individual tooth. During the measurement, both jaws should be in a state of complete rest. This is a condition when the lower jaw is as close to the upper jaw as naturally as possible. Only such an arrangement will make it possible to obtain accurate measurement results. A normal distance is considered to be 2-5 mm.
The height of the bite is the localization of parts of the dentition, and its size is the main factor in the normal position of the teeth. Thus, its incorrect height is one of the main signs of disorders in the structure of the jaws.
In addition to special methods, height is determined even by ordinary observation, but correct measurement can only be done by a highly qualified orthodontist with many years of experience.
On the issue of optimal occlusal relationships
Author: Malanyin Igor Valentinovich
Doctor of Medical Sciences,
Professor, Academician of the Russian Academy of Economics,
Honored Worker of Science and Education
Article published: Dental South magazine. Krasnodar, 2007
When preparing for prosthetic or restorative treatment, the main components of the diagnostic process are a detailed medical history and a thorough clinical examination in dentistry. However, treatment planning cannot be carried out only on the basis of intraoral examination data; it is also impossible to accurately determine, mark and count contacts, their ratio and collision moments in the oral cavity. Limited access and visualization in the oral cavity, saliva, and shiny surfaces of abrasion facets and restorative materials make it difficult to accurately mark contacts using articulating paper. The patient's neuromuscular system may habitually direct the mandible away from obstructions, making them more difficult to identify. Additional research methods, such as radiography, diagnostic models in articulators, axiography, functioniography and kinesiography, allow you to obtain the necessary information.
The goals of an occlusion examination are to:
- Determining the initial data, the analysis of which will make it possible to objectively judge the changes that have occurred,
- Identifying any signs of occlusal pathology. Early detection of symptoms can prevent the patient's occlusion from worsening,
- Deciding on the choice between the reorganizing approach of restorative therapy, which involves shifting the maximum intercuspid position to the posterior contact position, and the conformational approach, preserving the intertubercular position.
Occlusion is a biodynamic interaction between the teeth, the neuromuscular system, supporting structures and the TMJ. As in any other physiological system, some degree of adaptability is allowed in this interaction, depending on the magnitude and duration of any changes. Slow changes are likely to cause adaptation, even if they ultimately lead to significant deviation from the ideal norm. The ideal norm is considered to be uniform bilateral contact of the tubercles and grooves throughout the closure of both dentitions (interkuspidation). In the sagittal plane, the apex of the upper canine fits into the space between the lower canine and the adjacent mandibular first premolar. The mesial buccal cusp of the upper first molar fits into the mesial buccal groove of the lower first molar (Fig. 1). An ideal bite is a pattern of occlusion of the anterior teeth.
Rice. 1.
The lower central incisor is in contact with the cutting edge with the mesial and central part of its antagonist, the lower lateral incisor is in contact with the distal part of the upper central incisor and the mesial part of the upper lateral incisor. Accordingly, the lower canine is in contact with the distal part of the upper lateral incisor and the mesial part of the upper canine (Fig. 2).
Rice. 2.
With correct contact of the incisors, the vertical overlap in the sagittal plane (overbite) according to Magox is 3-4 mm (Fig. 3, C). The distance between the central incisors in the horizontal plane (overjet) affects the trajectory of movement in the sagittal and frontal planes during the last 0.5 mm when teeth are closed. The average distance between the cutting edge and the deepest point of the vestibule for the upper central incisors is 20 mm (Fig. 3, A) for the lower incisors - 17.5 mm (Fig. 3, B).
Rice. 3.
Each tooth, except the upper third molars and lower central incisors, has two antagonists, while the tooth of the same name in the opposite jaw is called the main antagonist, and the second is called the adjacent antagonist. The load-bearing cusps of the lateral teeth maintain the height of occlusion; on the upper jaw these are the palatal ones, on the lower jaw they are the buccal ones. They crush food, determine the nature of the movement of the lower jaw within the occlusal field and redistribute chewing forces so that the main chewing load is directed along the axis of the tooth. They are located closer to the center of the chewing surface, in contrast to the protective ones (on the upper jaw - buccal, on the lower jaw - lingual). Protective tubercles perform the function of separating food, create sliding surfaces on their slopes for antagonists during articulation, and protect the tongue and cheeks from getting between the teeth. Closing forces must be shifted to the center of the chewing surface and act along the longitudinal axis of the tooth. The tubercles that fall into the recesses of the chewing surface of the antagonist contact at three points, the tubercles that fall on the edges of the edges contact at two points. The area of all occlusal contacts of the dentition in central occlusion is no more than 4 mm2. The load-bearing palatal cusp of the upper first premolar fits into the distal recess of the lower first premolar. The palatal cusp of the maxillary second premolar also fits into the distal recess of the mandibular second premolar, and a three-point contact is also observed (Fig. 4).
Rice. 4.
The mesial palatal cusp of the upper first molar fits into the central recess of the mandibular first molar, with contact points located on the triangular edge of both lingual cusps and on the distal buccal cusp of the lower molar. The palatal distal cusp of the maxillary first molar contacts the distal marginal edge of the mandibular first molar (Fig. 5).
Rice. 5.
A similar thing happens with the second molar of the upper jaw. The load-bearing cusps of the lower first premolar have a point of contact on the mesial edge of the upper first premolar. The buccal cusps of the upper second premolar contact the distal edge of the upper first premolar and the mesial edge of the upper second premolar. The mesial buccal cusp of the lower first molar has a point of contact at the distal edge of the upper second premolar and the mesial edge of the upper first molar (Fig. 6).
Rice. 6.
The distal buccal cusp fits into the central recess of the upper first molar. In this case, the contact points are located on the triangular edge, on the mesial palatal tubercle and on both buccal tubercles. A similar thing happens with the second molar of the lower jaw. The lateral group of teeth takes on a significant load during closure, with the axes of forces directed along the longitudinal axes of the teeth. The front teeth are not prepared for the forces that arise during closure, so they are protected by the lateral teeth, in turn, the front teeth protect the lateral teeth by directing their tubercles accordingly - during articulation, disocclusion of the lateral teeth occurs as a result of the guiding action of the incisors and canines. This occlusion is called mutually protected. Motsch formulated the basic criteria for correct occlusion: The occlusal surfaces must be formed so that the food is crushed as much as possible under minimal impact of chewing forces. The antagonist teeth must close in such a way that the chewing forces act along their major axis. The closure of teeth or groups of teeth in contact with each other should occur evenly and simultaneously. The supporting tubercles should rest on the grooves or marginal ridges of the antagonist tubercles. When biting with the front teeth, the side teeth should not touch. The lateral teeth should crush food without the participation of the front teeth. All elements involved in occlusion must be functionally interconnected.
Understanding the relationship between form and function highlights the critical importance of attention to occlusion in the complex process of optimizing or maintaining oral health.
The study of functional occlusion both in the oral cavity and on collapsible jaw models in articulators allows us to analyze each clinical situation and make a decision on the most effective restorative treatment, prosthetics or occlusal correction to recreate uniform and simultaneous contact of all teeth and ensure stable occlusion.
Causes and types
Reasons that have a negative impact on the intermaxillary distance:
- greater abrasion of teeth, due to which the strength of hard tooth tissue is lost;
- functional overload of individual teeth, which can be caused by improper bridge prosthetics;
- disorders of the nervous system that are accompanied by grinding of teeth;
- with a fight in the gastrointestinal tract;
- disturbance of phosphorus-potassium metabolic processes.
There are high and low pathological bites. The reason for the overestimation may be an incorrectly made denture, when the implant turns out to be slightly higher than the rest of the teeth.
Low bite, as a rule, is diagnosed when the hard tissues of the tooth are severely abraded, and in rare cases, when the prosthesis is installed incorrectly.
What exactly does physiological rest mean?
Physiological rest - relaxation of the muscles of the upper and lower jaw as much as possible. In a state of anti-gravity reflex, as a rule, the jaws do not touch each other. The jaw is always in this state; contact occurs during conversations and eating. Doctors consider the normal distance between the jaws to be no more than 2-5 mm. Dentists distinguish between two conditions of malocclusion. The main difference is the height:
- Overpriced. The main culprit of this pathology is an unprofessionally made prosthesis. Teeth opposite each other are constantly in contact with each other. During physiological rest, the distance between the jaws deviates from the norm to a lesser extent or is absent altogether. The worst thing in this situation is damage to the joint, which occurs due to long-term injury to the prosthesis and strain on the masticatory muscles.
- Understated. This pathology occurs when the individual tooth surface is highly abraded, or when the prosthesis is not professionally installed. An underbite is considered when, in a state of physiological rest, the distance between the upper and lower jaw is more than three to four mm, while we do not observe any changes in appearance. In this case, the patient experiences angular cheilitis - a disease of the mucous membrane and skin of the corners of the mouth, as a result of increased salivation.
Measurement methods
The anatomical method of determining the height of the bite “by eye”, that is, depending on the physiological structure of the face, is practically not used today in modern medicine.
An anatomical-physiological-specialist places two points. One at the base of the nasal septum, the other in the center of the chin. After this, asking the patient to move his lips, then entering a state of rest, the doctor measures the distance between the points placed earlier. Occlusal ridges are inserted into the patient's oral cavity, which the patient will be asked to bite lightly and the distance between the points will be measured again. The value revealed as a result of these calculations will be the bite height. Any deviation from the norm, to a greater or lesser extent, will indicate an under- or over-occlusion.
As a result of these manipulations, the dentist removes or increases the height of the lower bite ridge until the height of your bite reaches normal.
During the procedure, the dentist pays attention to how your face changes. With skilled work, your facial features should become physiologically more correct.
Planning for prosthetics
There are some differences in the manufacture of dentures for patients with high and low bites. When an overbite is diagnosed, special mouthguards and bite plates are individually made for you, made from impressions of your oral cavity. The time it takes to wear plates and aligners depends on how large the deviation from the norm is in the patient, as well as on the structure and functioning of the patient’s bone and muscle structures. If you have been diagnosed with an underbite, the dentist acts as follows: for 2-3 months, the patient is put on a special non-removable plate, which will help create intermaxillary occlusion - this method is called the Dahl design.
Extending crowns artificially is another method for this pathology. The problem is solved locally, without correcting the remaining teeth. Only a certain element of the dentition is pulled out, causing a deviation from the norm. If these methods are ineffective, then surgical intervention is resorted to.
Whatever problems you experience, the main thing is to contact a specialist in time in order to get the most gentle treatment methods.
Height Determination Methods
The height of occlusion is determined using parameters such as the size and height of each individual tooth. During measurements, both jaws should be in a state of complete rest. This is a condition when the lower jaw is closest to the upper jaw. Only such an arrangement will make it possible to obtain accurate measurement results. A variant of the norm is a distance of 2-5 mm.
Anatomical method
The method is based on determining the normal position of the lower jaw. Experts in this field of dentistry, scientists Gysi and Keller, believe that this method must be guided by certain anatomical features, namely:
- The lips remain mobile and touch each other without tension during measurements.
- The corners of the mouth remain raised, the nasolabial folds remain clearly defined.
Orthodox practitioners believe that this method is not absolutely reliable, and therefore is not widely used in practice.
Hence, the desire of orthodontists to use objective data, which includes anthropometric measurements, is understandable.
Anatomical-functional method
The technique of this method is quite simple. The patient is asked to pronounce phrases containing labial sounds. After this, the patient closes his lips, and the muscles involved in speaking go into a state of relative rest—they should calmly touch each other. Nasolabial folds should have a normal appearance, and wrinkles in the area of the corner of the mouth should not be pronounced. If the position of the face takes the written form, then the patient’s height of relative rest has been established. It is measured with a ruler, and then templates with occlusal ridges are inserted into the patient’s oral cavity. Since the resting height is generally 2-3 mm greater than the height of the central occlusion, the ridges are cut or increased until the height at closure becomes 1-2 mm less than the previously determined resting height. This method is also subjective, but better than the previous one.
Preparation for prosthetics for malocclusion
| Click to sign up for a FREE consultation |
Depending on the type of pathology, a correctional scheme of preparation for future manipulation is determined. In the case of under-occlusion, an acceptable occlusion is first determined. For this purpose, supradental aligners or bite plates are used, that is, the reduced indicator is artificially brought to the normal level. In case of hyperabrasion of the tooth surface, the optimal correction is the installation of a Dahl device. This is a permanent plate made of chrome. It is recommended to wear the design for 3 months. An effective option for bringing the bite height to normal is artificial lengthening of the tooth crowns. In particularly advanced cases, they resort to surgical manipulations - the root of the tooth is exposed, the gum area is given the desired shape and relief.
Material and methods
We determined the CV in an orthopedic dentistry clinic for individuals with intact dentition ( n
=5). 4 methods for determining the CV were used, most often used in clinical practice by orthopedic dentists. One-stage, two-phase impressions were taken from the upper jaw (MF) and mandible using polyvinylsiloxane mass (Zhermack, Elite HD). To cast the models, supergypsum (Elite Rock, Zhermack) was used, which was mixed in a proportion of 100 g per 30 ml of distilled water at a temperature of 18 °C in a vacuum mixer for 30 s.
To determine the CS, a bilateral manipulation was used (P. Dawson, 2006); frontal deprogrammer (V. Lucia, 1964); multisheet template (J. Long, 1970); device for intraoral recording of the Gothic angle (A. Gysi, 1908).
Using each method, 1 operator carried out 10 registrations of the CS of the jaws (200 registrations of the CS in total); the intervals between determinations of the CS were 30 min.
1. The method of bilateral manipulation according to P. Dawson involves relaxation of the masticatory muscles by manual movements of the LF around the hinge axis, as close as possible to the terminal position without occlusal contact of the teeth; the amplitude of the movements performed should not exceed 1-2 mm. After deactivating the muscles and finding the physiological terminal position of the TMJ condyles, a load test was performed to check the correct orientation of the disc-condyle-absence of pain. According to the author of the technique, only in the CS can the TMJ withstand significant loads from the levator muscles without the appearance of signs of discomfort and pain. To register the CS, we used a special hard wax with the addition of aluminum particles (AluWax, Maarc), which was heated and imprints of the palatal cusps of the HF from the canine to the second molar were obtained. After checking the obtained prints on the HF model, the lower part of the plate was heated, then the jaws were installed in the C.S. using bilateral manipulation. After the plate hardened, the resulting impressions were checked on plaster models, and the impressions of the cusps were refined with cement (TempBondNE) in the mouth (Fig. 1).
Rice. 1. Registrar Ts.S. from Aluwax.
2. To determine the CA using the frontal deprogrammer (Fig. 2),
Rice. 2. Registration of C.S. using a frontal deprogrammer. fabricated by the direct method from acrylic plastic (Re-FineBRIGHT), a frontal bite block with a flat surface was produced, allowing the NP to move fully in the transversal plane. The principle of operation of the frontal deprogrammer is to open the lateral group of teeth so that the condyles can take a terminal position in the center of the jaws.
3. Multi-sheet calibrator is one of the most popular devices for determining C.S. The calibrator consists of several layers of flexible plastic; layers are calibrated in thickness (100 µm). The method consists in separating the chewing group of teeth; smooth and flexible plates allow horizontal displacement of the LF as the condyles occupy the terminal position. After finding the center line, the plates are removed one by one until the first contact appears (Fig. 3, 4).
Rice. 4. Registration of Ts.S. using a multisheet template.
Rice. 3. Multisheet template.
4. For intraoral recording of the Gothic angle, a funcciograph (Massad jaw recorder) was used. On plaster models of jaws, individual plates with retention elements were made from photo-curable plastic; a part of the func- ciograph with a pin was attached to the upper plate, and a recording pad was attached to the lower plate (Fig. 5).
Rice. 5. Individual intraoral plates with a funcciograph. Before recording the Gothic angle, individual plates were fitted in the mouth, and the patient was trained in eccentric movements for 10 minutes. Contrast articulation spray was applied to the lower platform; the pin was positioned so that the LF could make eccentric movements without occlusal contacts. The patient consistently performed protrusive, left, and right laterotrusive movements. A plate with a hole corresponding to the recording pin was fixed to the mandibular platform with sticky wax; the hole in the plate coincided with the top of the Gothic corner (Fig. 6, 7).
Rice. 6. Recorded Gothic angle on the bottom plate of the funciograph.
Rice. 7. Registration of Ts.S. using a functionograph. The parts of the funciograph were compared in the mouth; in this case, the position of the pin corresponded to the center of gravity of the jaws. Registration of Ts.S. the listed methods were carried out with polyvinylsiloxane material (OcclufastRock, Zhermack).
To transfer the HF position, a facebow (SAM Axio quick III) was applied to the patient. The models were plastered in an articulator (SAM 2 PX) using articulation plaster (Elite Arti, Zhermack) one at a time; The NP was recast using 40 CS registers for each patient. To obtain an imprint of the 1st contact in the CS, 8 µm articulating foil (Bausch) was used. To analyze contacts in the CS, the photometric method was used (Canon 650D, Canon 60 mm macroISUSMf2.8, Canon macroring MR-14 EX). Occlusal photographs of plaster jaw models were taken at a focusing distance of 0.3 m. The jaw models were fixed and photographed parallel to the horizontal plane. Photography was carried out in manual mode; in this case, the white balance was set automatically: ISO 100, exposure 160, aperture 25, RAW image format. A total of 400 photographs were taken (Fig. 8, 9).
Rice. 9. Photograph of the occlusal surface of the upper jaw with a level.
Rice. 8. Positioning the camera and model when carrying out the photometric method.
To carry out calculations, graphic images were loaded into Adobe Photoshop, and metric data was converted into digital data (pixels). The initial position of the contact and, therefore, the reference point was taken to be the contact obtained during the first plastering of the jaw models into the articulator when determining the CV by each of the methods. The change in the position of the contacts for each variant of registration of the CS was calculated in the mesiodistal (MD) and vestibulo-oral (VO) directions (transversal and distal change in the position of the LF). A grid with a single cell size of 5 pixels, which corresponds to 19 μm, was superimposed on the images (Fig. 10).
Rice. 10. Occlusal contact with digital grid. Cropping was identical for all photographs. The horizon line was taken to be a line drawn through the tops of the hillocks. Axis V.O. the contact deflection was parallel to the horizon line, the MD axis of the contact deflection was at an angle of 90° to the axis BO; it corresponded to a line drawn through the median fissure on the chewing surface of the tooth. Each contact point was divided into a rectangular or square (depending on the shape of the contact) area. Next, we studied the deviation of the sides of this figure along the VO and MD axes from the initial position (Fig. 11, 12).
Rice. 12. Scheme of deviation of contacts from the first definition within the group (the starting point is indicated in black).
Rice. 11. Calculation of occlusal contact deviation in Adobe Photoshop.
Statistical analysis was carried out using the Statistica-10 package. In all statistical analysis procedures, the critical significance level p
was taken equal to 0.05.
The normality of the distribution was checked using the Shapiro-Wilk test, and the hypothesis about the equality of general variances was tested using the Fisher F test. t
were used to test statistical hypotheses . A total of 200 CA registrations were carried out.
Determining the optimal bite height is one of the important and complex problems of dentistry. There are many methods for determining bite height. One of them is anatomical and physiological [1]. This method is easy to use, does not require special devices, but is not accurate enough, since the doctor has to focus on the soft tissues of the face, the patient’s subjective sensations and his ability to voluntarily relax the masticatory muscles.
In order to gain a deeper understanding of the individual anatomy of the patient’s dental system, dentistry uses cephalometric analysis of teleroentgenograms (TRG) of the skull in a lateral projection. This analysis has become widespread among orthodontists, as it allows one to assess the size and position of the jaws relative to each other and the bones of the skull, which is necessary for planning orthodontic treatment. The method is also used by dentists and orthopedists to plan artificial dentition in conditions where there are no sufficient landmarks for this [2, 3].
Cephalometric analysis of TRH is not directly intended and does not provide for the calculation of bite height. However, since many methods of cephalometric analysis to one degree or another contain direct or indirect information about the height of the bite, we believe that such a fundamental possibility exists [4].
The purpose of this study is to develop algorithms for calculating bite height based on the principles of cephalometric analysis developed by different authors.
One of the first researchers to develop his own method of analysis was W. Downs (1948) [5]. The peculiarity of this analysis was that the author positioned it not as a basis for achieving the treatment goal, but as a method for studying and measuring the relationships of the skeletal components of the face, i.e., the upper (MF) and lower jaws (MF) and the dentition, in particular the molars .
S. Steiner (1953) [6] formulated a balanced and comprehensive system for deciphering TRG of the skull in the lateral projection for skeletal, dentofacial and soft tissue formations. The main parameter that C. Steiner pays attention to is the angle ANB. Its value clearly displays the position of the jaw bones relative to each other in the sagittal direction and serves as valuable diagnostic information when planning further treatment.
In 1979, R. Ricketts [7, 8] presented his own method for calculating the TRG of the skull in a lateral projection. His goal was to combine aesthetic and functional parameters and determine the direction of growth of the facial skeleton. Ricketts proposed taking point Xi as the geometric center of the LF branch to estimate the angular values of the height of the lower part of the face and determined the normal value of the bite height (angle ANS-Xi-Pog).
In 1983, orthodontist J. McNamara [9] proposed his own version of cephalometric analysis, which followed from the work of Ricketts and Harvold et al. J. McNamara developed a table in which the effective length of the HF is correlated with the length of the LF and the height of the lower part of the face . Using this table, the doctor can more accurately plan the position of the jaws and teeth during the upcoming treatment.
In 1989, R. Slavicek summarized previously proposed methods of cephalometric analysis and proposed a formula for calculating the height of the lower face, taking into account the phenotypic variability of the patient [10, 11].
In 2010, T. Karine et al. [12] proposed a method for determining the height of the lower part of the face (Seraidarian-Tavano analysis). This cephalometric analysis is based on the assessment of facial angles, the ratio of which determines the height of the bite.
Determination of bite height based on TRG analysis of the skull in the lateral projection according to Downs
W. Downs (1948) was the first author of a cephalometric analysis of the skull in a lateral projection. According to W. Downs, an indicator that indirectly characterizes the height of the bite is the angle between the Frankfurt horizontal (FH) and the mandibular plane (Menton-Gonion), measured at 3 points (Orbitale, Porion and Menton) [13] (Fig. 1). Normally, this angle is 21.9±3.2°.
Rice. 1. Frankfurt horizontal plane FH is drawn between points Po - the upper edge of the bony auditory canal - and Or - the lower edge of the orbit, the mandibular plane (Menton-Gonion) is drawn between points Me - the lowest point of the mental symphysis - and Go - a point on the outer edge of the angle of the MF when it intersects with the bisector of the angle formed by the tangents to the lower edge of the body and the rear edge of the branch.
You cannot directly set the position of the LF by changing the angle of inclination of the mandibular plane and using the point of its intersection with the Frankfurt horizontal line as the axis of rotation. In this case, the head of the LF will significantly lower or rise inside the articular fossa, which is unacceptable from a clinical point of view.
A more correct approach and appropriate control of changes in the angle of inclination of the mandibular plane would be to rotate the MF around the hinge axis.
The average position of the LF hinge axis—point Ax (1, 2)—is determined according to the recommendations of R. Slavicek:
— build the hinge-infraorbital axis, which differs by 6.5° from the FH and passes through the condylar process of the MF;
— on the resulting segment of the intersection of the condyle with the hinge-infraorbital axis, mark point Ax (1, 2) in front of the posterior edge of the condyle contour at a distance of 2/3 of the length of this segment (Fig. 2).
Rice. 2. Determination of the average hinge axis (axis of rotation LF - point Ax (1,2)) according to Slavicek.
Our proposed method for determining the bite height using the TRG of the skull in the lateral projection, taking into account the Downs analysis, was as follows:
— the initial value of the angle of inclination of the NP was measured on a radiograph of the head in a lateral projection between the Or-Po and Me-Go axes;
— draw a line Me'—Go', parallel to Me—Go, through the rotation point of the NP Ax (1, 2) (Fig. 3);
Rice. 3. The line Me'—Go', drawn through the rotation point of the LF Ax (1, 2), is parallel to the line Me—Go.
— calculated the difference between the obtained value of the LF inclination angle and its normal value (
21.9º); the resulting difference can be positive or negative and is expressed in the angular value X (line Me2-Go2);
— then the LF contour was rotated around point Ax (1, 2) clockwise if the angle X is positive and counterclockwise if the angle X is negative; Thus, the angle of inclination of the LF corresponded, according to Downs, to the normal value, and the height of the bite was reduced to the normal value (see Fig. 3).
Determination of bite height based on TRG analysis of the skull in the lateral projection according to Steiner
In 1953, C. Steiner proposed a method for analyzing TRG of the skull in a lateral projection. This method is still one of the most popular all over the world, since the C. Steiner analysis is a balanced and comprehensive system for deciphering TRG of the skull in the lateral projection for skeletal, dentofacial and soft tissue formations, which can be used to predict the growth of the studied areas.
The skeletal component of the analysis allows us to determine the position of the HF and LF, as well as their position in relation to the skull and to each other.
C. Steiner's analysis uses the anterior cranial base or Sella-Nasion axis as the starting line for the skeletal region (Fig. 4). The Sella (S) and Nasion (Na) points are selected in such a way that they are located in the midline structures of the skull and do not depend on the possible rotation of the patient’s head in relation to the cephalostat.
Rice. 4. Na (nasion osseum) - point at the intersection of the median plane with the nasofrontal suture; the most anterior point of the sutura naso-frontalis; S (sella) - sella turcica (the geometric center of the fossa, determined visually); Go (gonion) - a point on the outer edge of the LF angle when it intersects with the bisector of the angle formed by the tangents to the lower edge of the body and the posterior edge of the branch; Gn (Gnathion) is the most anteroinferior point of the mental protuberance.
To measure the LF tilt angle, the angle between the Go-GN and S-N axes is used (see Fig. 4), which was proposed by Wylie and Johnson.
The angle of inclination of the LF, according to C. Steiner, is normally 32±4°.
Our proposed method for determining the height of the bite using the TRG of the skull in the lateral projection, taking into account the analysis according to C. Steiner, is as follows:
— the initial value of the angle of inclination of the LF was measured on a radiograph of the skull in a lateral projection (see Fig. 4);
— draw a line Go'—Gn', parallel to Go—Gn, through the average hinge axis of the NP Ax (1, 2) (Fig. 5);
Rice. 5. The line Go'—Gn', drawn through the averaged hinge spine of the NP Ax (1, 2), is parallel to Go—Gn; rotation of the LF contour around the point Ax (1, 2) until Go'—Gn' and Go2—Gn2 are aligned with each other.
— the difference between the obtained and normal values of the LF inclination angle was calculated, the resulting difference can be positive or negative and is expressed in the angular value X between the Go'-Gn' and Go2-Gn2 axes;
— then the LF contour was rotated around the point Ax (1,2) until the Go'-Gn' and Go2-Gn2 axes aligned with each other; thus, the angle of inclination of the LF was brought to a normal value, and the height of the bite corresponded to the normal value according to Steiner (see Fig. 5).
Determination of bite height based on Ricketts analysis
In 1956, R. Ricketts presented his method of cephalometric analysis, the main goal of which was to combine aesthetic and functional parameters and determine the direction of growth of the facial skeleton. The height of the lower part of the face was determined as the angle formed by the intersection of two axes: ANS—Xi and Xi—Pog (Fig. 6). According to R. Ricketts (1956), normally the angle ANS - Xi - Pog is 45°. Point Xi is determined by the intersection of the diagonals of a rectangle (R1, R2, R3, R4) parallel to the pterygoid vertical [PtV] (perpendicular to FH, passing along the posterior edge of the pterygopalatine fossa) (Fig. 7).
Rice. 6. ANS (Sna - spina nasalis anterior) - apex of the anterior nasal spine; Pg (Pog - pogonion osseum) - the most anterior point of the chin protrusion in the median section when the head is oriented along the Frankfurt horizontal; Xi is the geometric center of the LF branch proposed by Ricketts.
Rice. 7. R1 - point at the intersection of the deepest part of the anterior border of the LF branch and the perpendicular to FH; R2 is the point at the intersection of the middle part of the posterior border of the LF branch and the perpendicular to FH; R3 - point located on the lowest part of the sigmoid notch of the LF branch; R4 is the point at the intersection of the lower boundary of the LF and the perpendicular to FH passing through the point R3.
Our proposed method for determining the bite height using the TRG of the skull in the lateral projection, taking into account the Ricketts analysis, was as follows:
— measured the value of the actual angle ANS—Xi—Pog;
— on the TRG of the skull in the lateral projection, a new angle ANS-Xi-Pog' equal to 45° was laid out;
— then the LF contour was rotated around the Ax point (1, 2) until the Pog point intersected with the Xi-Pog' axis, which brought the bite height to the normal value according to Ricketts (Fig. 8).
Rice. 8. Angle ANS-Xi-Pog' is 45°; rotation of the LF contour around point Ax (1, 2) until point Pog intersects with the Xi-Pog' axis.
Determination of bite height based on McNamara analysis.
The cephalometric analysis of J. McNamara (1984) follows from the work of R. Ricketts and Harvold et al. This analysis includes a series of linear relationships of the HF dentition, maxillary bones, skull base and chin position.
According to McNamara, lower facial height is related to midfacial length. The height of the lower part of the face is measured from the ANS point to the Me point, the midfacial length is measured from the Co point to the A point (Fig. 9).
Rice. 9. ANS (spina nasalis anterior) - apex of the anterior nasal spine; Me (menton) - the lowest point of the mental symphysis; Co (condylion) - a point at the top of the contour of the articular heads; A is the deepest point of the anterior contour of the HF between the ANS and the incisor.
An increase or decrease in the size of the jaws is proportionally reflected in the height of the bite (see table).
The ratio of the length of the upper jaw (Co - A), the length of the lower jaw (Co-Gn) and the height of the lower part of the face (ANS-ME)
Our proposed method for determining the height of the bite using the TRG of the skull in the lateral projection, taking into account the analysis according to J. McNamara, was as follows:
— measured the initial midfacial length;
- using the table, according to the obtained value of the mid-facial length, the corresponding height of the lower part of the face was found;
— to visualize the trajectory of the NP movement, a circle was constructed with a center at point Ax (1, 2) and radius Ax (1, 2) - Me; then on this circle the position of the point Me' was noted, provided that the distance ANS - Me' corresponded to the value of the height of the lower part of the face found from the table;
— then the contour of the lower jaw was shifted around the rotation point of the LF Ax (1, 2) until the point Me intersected with the point Me', which brought the bite height to the normal value according to J. McNamara (Fig. 10).
Rice. 10. Displacement of the LF contour around its rotation point Ax (1, 2).
Determination of bite height based on analysis according to R. Slavicek
R. Slavicek (1989) presented his own method of cephalometric analysis, based on measuring angular values and taking into account the phenotypic variability of the patient.
This technique also uses the Xi point (the geometric center of the LF branch), however, unlike the Ricketts technique, the location of the Xi point is determined somewhat differently:
— first, a perpendicular to the FH plane is constructed through point R3 (the point located in the lowest part of the sigmoid notch of the LF branch);
— at the intersection of this perpendicular with the lower contour of the LF, point R4 is marked;
— then, parallel to the R3-R4 axis, a line is drawn through point R1 (the point of contact with the boundary of the notch on the front branch of the LF);
— a line parallel to the FH plane is drawn through point R1; at its intersection with the posterior border of the LF branch, point R2 is marked;
— then a line is drawn parallel to the R3-R4 axis through point R2;
— through points R3 and R4, lines parallel to the FH plane are constructed.
Lines constructed through points R1, R2, R3, R4 form a rectangle adjacent to the LF branch.
Point Xi is located in the center of the rectangle at the intersection of the diagonals (Fig. 11).
Rice. 11. Point Xi is the intersection point of the diagonals of the rectangle R1R2R3R4.
According to the analysis of TRG according to R. Slavicek, the height of the lower part of the face is determined by
glob formed by the intersection of 2 axes: Xi—ANS and Xi—Pm (Fig. 12).
Rice.
12. ANS (spinanasalis anterior) - apex of the anterior nasal spine; Pm (protuberantiamenti—suprapogonion) is a point on the bend of the anterior contour of the mental symphysis. The norm value is calculated using the formula:
58.0+0.2·(A)—0.2·(B)=Ideal vertical position (IVP),
where A is the angle of the mandibular plane (see Fig. 1), B is the angle of the facial axis (Fig. 13).
Rice. 13. Angle of the facial axis - the angle between the Nasion - Basion plane and the Pterygoid - Gnathion axis; Na (nasion) - the most anterior point of the frontonasal suture in the sagittal plane; Ba (basion) - a point in the middle of the anterior edge of the foramen magnum; Gn (gnathion) - a point located in the middle between the anterior and lower points of the bony part of the chin; PT (pterygoid) is a point at the intersection of the internal border of the round foramen with the posterior wall of the pterygomaxillary fissure.
Our proposed method for determining the height of the bite using the TRG of the skull in the lateral projection, taking into account the analysis according to Slavicek, was as follows:
— measured the values of the angle ANS—Xi—Pm, the angle of the mandibular plane and the angle of the facial axis (Ba—PT—Gn);
- then the ideal height of the lower face (IVP) was calculated using the given formula;
— on the TRG of the skull in the lateral projection, a new angle ANS—Xi—Pm' was plotted, the value of which was obtained from the IVP calculation data;
— then the contour of the LF was shifted around the point of its rotation of the LF Ax (1, 2) until the point Pm intersected with Pm', which brought the bite height to the normal value according to Slavicek (Fig. 14).
Rice. 14. Displacement of the LF contour around its rotation point Ax (1, 2) until the intersection of the point Pm with Pm'.
Analysis of TRG of the head in the lateral projection according to Seraidarian-Tavano
This technique was proposed in 2010 by Karine T. Tavano et al. and was developed on a group of patients with skeletal class I and the presence of all teeth, with the exception of third molars, as well as the absence of a history of orthognathic, surgical, orthodontic, reconstructive operations or restorative procedures on more than two molars in 1 quadrant.
For calculations using this method, the Frankfurt horizontal line, as well as the following points, were used as starting points:
—Na ( nasion osseum
) - point at the intersection of the median plane with the nasofrontal suture;
the most anterior point of the sutura naso-frontalis
;
— ENA ( anterior nasal bone
) - the most anterior point at the bottom of the nasal cavity, in the midsagittal plane;
point ENA is equivalent to point ANS (Sna - spina nasalis anterior
) (see Fig. 6, 8, 9, 10, 13, 14); in the further description we left the mention of ENA, as this is done by the authors Seraidarian-Tavano;
-Me ( menton)
) - the lowest point of the mental symphysis.
Our proposed method for determining the bite height using the TRG of the skull in the lateral projection, taking into account the Seraidarian-Tavano analysis, was as follows:
— the mandibular plane was marked (a straight line drawn through Me and the lowest point on the contour of the mandible in the area of the gonial angle);
— draw a tangent line to the posterior contour of the MF branch in the area of the most distal point of the condylar process of the MF and the ascending part of the gonial angle;
— at the intersection of these lines, a Go point was built;
— noted FH;
— marked the center of the face (point CF) at the intersection of the perpendicular to FH with the distal surface of the contour of the pterygopalatine fissure;
— built the CF-NA and CF-ENA axes;
— measured the angle of the upper third of the face Upper Angle (UA) (between the axes CF-Na and CF-ENA) (Fig. 15);
Rice. 15. Upper Angle (UA) - the angle of the upper third of the face between the CF-Na and CF-ENA axes; ENA (anteriornasalbone) is the most anterior point at the bottom of the nasal cavity, in the midsagittal plane.
— on the mandibular plane, an angle TLA was laid equal to the angle UA, with the apex at point Go and the zero line coinciding with the Me-Go line (Fig. 16);
Rice. 16. Angle TLA is equal to angle UA with its vertex at point Go and the zero line coinciding with the Me-Go line.
— at the intersection of one of the rays of the TLA angle with the CF-ENA axis, the 3rd angle MA is formed;
- according to the authors, normally the CF-ENA and Me-Go axes are parallel, and the angles MA and UA have the same values;
— then, through the rotation point of the jaw Ax (1, 2), lines CF'—ENA' and Me'—Goc' were built, parallel to the axes CF—ENA and Me—Go;
— moved the LF contour relative to the rotation point Ax (1, 2) together with the Me'-Go' line until the CF'-ENA' and Me'-Go' lines coincided, which brought the bite height to the normal value according to Seraidarian —Tavano (Fig. 17).
Rice. 17. Moving the LF contour relative to the rotation point Ax (1, 2) together with the line Me'—Go' until the lines CF'—ENA' and Me'—Go' coincide.
The proposed methods for determining the height of the bite according to TRG data provide the possibility of additional control of the correct determination of the height of the bite during the reconstruction of the dentition. Of interest is the probability of coincidence of the bite height determined by calculation methods of TRG using the methods of different authors - which of the described methods is the most accurate and suitable for use in the clinic or in automatic computer systems for constructing dentition?
We expect to find answers to the questions posed by further studying this topic.