Publication date: June 28, 2022.
Information on this page was updated on October 15, 2021.
Mesial occlusion is recognized by researchers and practicing orthodontists as one of the rarest and most difficult dental pathologies to treat.
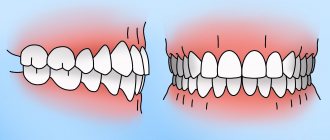
Mesial occlusion or progeny is a type of malocclusion in which the lower jaw protrudes forward relative to the upper jaw. The lower incisors overlap the upper ones or form a reverse sagittal fissure - the space between the front and lower front teeth.
Reverse incisal overlap
Reverse incisal overlap on CBCT image
How to determine mesial bite?
- By the face. Mesial occlusion can be determined by the structure of the face even without looking at the smile. The profile is concave - the middle third of the face falls back slightly, especially relative to the lower third. The chin protrudes forward and looks massive and disproportionate to the face and upper jaw. At the same time, the lower lip looks thicker, and the upper lip sinks. The facial expression seems angry.
- By posture. The temporomandibular joint is directly connected to the spine, so its malposition (as a result of malocclusion) affects the posture and balance of the entire body. Those with complex forms of mesial occlusion are characterized by a slight deviation of the body backwards. If you draw a straight line through the entire body in profile, the head will be tilted slightly back, and the pelvic bones will be pushed forward.
Concave profile with mesial bite
Poor posture with mesial occlusion - By smile and teeth. The clinical situation in which the lower incisors are in front of the upper ones is called reverse incisal overlap. This is the most characteristic intraoral sign of progeny. It is also characterized by: gaps between the teeth, dystopia (improper position) of the teeth, tilting of the lower teeth into the oral cavity.
Forms of prognathic occlusion
There are 4 forms of distal occlusion of the dentition:
- I form – characterized by retrognathia (insufficient development) of the lower jaw, while the upper one is developed normally;
- Form II – macrognathia (excessive enlargement) of the upper jaw bone is observed, as well as the size of the upper crowns being too large. Lower jaw – without deviations;
- III form - 2 anomalies are diagnosed at once - the lower jaw is underdeveloped and the upper jaw is overdeveloped;
- IV form - only the anterior section of the upper dentition protrudes forward.
Types of mesial occlusion
By form:
- Dentoalveolar form. Malocclusion as a result of incorrect position of the teeth.
- Gnathic or skeletal form is an abnormal bite formed by a pathology of jaw development.
A more complex form of malocclusion, sometimes requiring surgical intervention. Often, clinical cases of mesial malocclusion combine both forms - incorrectly positioned teeth and abnormal jaw sizes.
For reasons of occurrence:
- Congenital abnormal jaw sizes: macrognathia of the lower jaw - a large or elongated lower jaw; micrognathia of the upper jaw - underdeveloped, small upper jaw.
- Prognathia of the lower jaw is a forced position when individual teeth interfere with the normal closure of the jaws and jaw growth. This type of bite occurs in children on their baby teeth due to fangs that cling to the lower teeth and prevent the lower jaw from taking a normal position.
- Retrogression of the upper jaw is the posterior position of the upper jaw relative to the proportions of the face. Unlike micrognathia, in this case the jaw is of normal size, but incorrectly positioned.
- Abnormal tooth sizes: macrodentia - large teeth on the lower jaw, microdentia - small teeth on the upper jaw.
Treatment of prognathia in children
Depending on age, treatment of prognathia in children requires different orthodontic appliances. This is explained by the different sizes of bone structures, growth rates, as well as the level of mineralization of the bone tissue of the jaws.
- In children under 5-6 years of age, distal occlusion is treated with custom or standard bite formers and activated vestibular plates. The main therapeutic functions of these devices are stimulation of nasal breathing, active swallowing of food, and regulation of the pressure of the cheek and lip muscles on the teeth. As a result, the child’s jaws develop correctly.
- For children aged 6 to 12 years, functionally stimulating orthodontic equipment is used: Frenkel apparatus, orthodontic crowns with hooks for elastic traction, etc. To stretch and inhibit jaw growth, extraoral compression-distraction devices with cervical or occipital fixation are used.
- In adolescents from 13-14 years of age, it is possible to use various brace systems in combination with extraoral elastic traction. With this combination, there is a simultaneous effect on the dental-alveolar deformations and stimulation of the growth of the lower jaw.
- After 15 years, in especially severe cases, the upper premolars and wisdom teeth (if they exist and have already erupted) are removed, the dentition is straightened and they wait until the age of 23-24 to perform orthognathic surgery.
Request a call back or dial our number!
+7
This phone call does not obligate you to anything. Just give us a chance and we will help you!
Causes of mesial bite
In the early stages of development:
- Heredity - congenital abnormal structure of the skull and facial bones. It is transmitted genetically, sometimes depending on ethnicity. The likelihood of mesial occlusion in the Mongoloid race is higher than in Caucasians.
- Mother's illnesses during pregnancy, unfavorable external environment, lack of nutrients during intrauterine development.
- Incorrect breastfeeding.
- Macroglossia is an increased size of the tongue.
- Childhood diseases (rickets, endocrine gland disorders)
- Bad habits: sucking the upper lip, finger.
- Short frenulum of the tongue.
During the period of milk and permanent teeth:
- Impaired wear of baby teeth, as a result of which the teeth (usually fangs) interfere with the normal closure of the upper and lower jaws. When closing, the lower jaw slips and takes a forced position in front.
- Late eruption or early loss of teeth in the upper jaw.
- Supernumerary teeth on the lower jaw.
- Incorrect body position: lowering the head on the chest during sleep, resting the chin with the hand in a sitting position.
Prognathia: causes of occurrence
Distal bite, as this defect is also called, is most often congenital, hereditary in nature - the risk of developing such an anomaly is higher in people whose parents or grandparents also suffered from bite problems. But there are several other reasons why a child develops prognathia:
- pathologies of intrauterine development of the fetus;
- pathologies of postnatal development;
- improper nasal breathing in childhood;
- incorrect method of artificial feeding, when the baby makes almost no effort to suck milk from the nipple - the lack of load on the masticatory muscles leads to disruption of the development of the bite;
- too early loss of baby teeth, especially canines;
- a complication after rickets - a disease of infants and young children, which leads to impaired bone formation and insufficient mineralization due to vitamin D deficiency.
Consequences of mesial occlusion
First of all, mesial occlusion disrupts external aesthetics. A disproportionate face reveals an incorrect bite even if the person is not smiling. The facial expression seems stern and angry.
Irregular incisal overlap and gaps between the front teeth greatly complicate the chewing process. The front teeth wear against each other, and the entire chewing load is redistributed between several teeth, which decay faster and are more susceptible to caries due to constant work. When teeth are lost as a result of malocclusion, implantation and prosthetics are complicated - there may not be enough space for adequate restoration of teeth.
If the upper incisors, as a result of reverse overlap, reach the mucous membrane of the lower jaw, then a chronic injury occurs at the site of contact. It leads to bacterial growth, periodontitis, recessions and an increased risk of cancer.
Improper dental alignment or jaw structure directly affects the temporomandibular joint. The result of incorrect position of the joint is clicking, pain when opening the mouth or chewing food, headaches, dystrophy and jamming (freezing in one position) of the joint.
Consequences of distal occlusion in adults
Prognathia should be eliminated in childhood, preferably before the age of 14. If this is not done, a person will experience a number of problems in adulthood:
- firstly, a violation of facial aesthetics - abnormal occlusion always affects the appearance, because of this, self-esteem decreases and complexes arise;
- secondly, deterioration in the function of chewing and swallowing - due to poor closure of teeth, a person has to make approximately 30% more chewing movements compared to the norm;
- thirdly, speech disorders - a “lisp” and other speech therapy abnormalities occur.
It should be taken into account that those with a distal bite have a greater risk of developing dental diseases - caries, gingivitis, and enamel erosion. This happens due to the increased load on individual dental crowns and periodontal areas. In addition, there may be problems with the jaw joint - pain when chewing and talking, deterioration in mobility.
Therefore, you cannot ignore the problem; you should contact your dentist in a timely manner. Treatment of distal bite in children and adults is carried out by an orthodontist. You can select such a specialist on our website through a convenient search system.
Diagnostics
To draw up a complete clinical picture and treatment plan, you need high-quality diagnostic data of several types:
- Visual examination of teeth and face by an orthodontist. Usually occurs at the first consultation. The doctor evaluates the position, size and condition of the teeth. If necessary, refers to additional specialists.
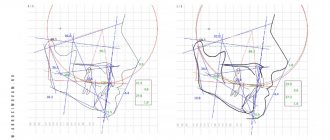
- Assessment of jaw position and size using CBCT. Only a 3D image of the entire skull will give the doctor an accurate idea of how the jaws are positioned relative to each other and the condition of the temporomandibular joint. Based on these data, a plan for moving the teeth is drawn up, and the need for surgical intervention or additional treatment of joint dysfunction is assessed.
- Assessing the position, relationship and closure of teeth using impressions.
- A detailed photo protocol for drawing up a treatment plan and further monitoring the dynamics of treatment.
Treatment
Treatment methods for mesial malocclusion depend on the patient’s age and the shape of the malocclusion (skeletal or alveolar). Earlier treatment is usually faster and more effective because the jaws, teeth and alveolar bone tissue are in the growth phase.
Treatment in milk and mixed dentition
When diagnosing mesial occlusion in a child with primary or mixed dentition, first of all, it is necessary to exclude factors that aggravate the pathology:
- bad habits. Special jaw appliances will help make it easier to wean yourself from a bad habit and adapt to the correct position of the jaws.
- improper swallowing or mouth breathing. To eliminate breathing problems, you will need to consult an ENT doctor.
- forced position of the jaw due to interfering tubercles or cutting edges of individual teeth. In this case, the teeth are ground to a safe extent for normal closure.
If the lower jaw is shifted forward slightly, then massage of the alveolar process (the place where the teeth grow) from the side of the palate in the anterior part of the upper dentition is indicated for correction. The general position of the jaw is corrected with removable devices.
In case of deep incisal overjet, the Brückle apparatus is used in the mixed dentition. It moves the upper teeth forward, and the bite block helps to release the bite on the anterior teeth.
Jaw development can be further hampered by pressure from the lips, tongue, and cheeks on the alveolar bone and teeth. The type 3 Frenkel function regulator normalizes the position and relationship of the teeth, tongue and cheeks.
Bruckle apparatus
Frenkel apparatus type 3
Studies show that it is impossible to restrain the growth of the lower jaw, therefore, in the primary and mixed dentition, orthodontic treatment is focused on stimulating the growth of the upper jaw. To do this, a partial bracket system “4+2” is installed on the permanent incisors and first molars. The action of braces helps to expand and lengthen the upper jaw.
Partial bracket system for mesial occlusion"
Treatment in permanent dentition of dentoalveolar form
In the dentoalveolar form, the mesial bite is formed due to the incorrect position of the teeth. To correct it, it is enough to install a braces system. Treatment is carried out with the mandatory use of intermaxillary traction - elastics, which help to pull the lower dentition back. In case of severe anomaly, the lower eighth teeth (wisdom teeth) are removed, and mini-screws are connected to extend the dentition. Mini-screws or micro-implants are small screws that become absolute support.
Treatment of gnathic permanent dentition
The skeletal form of the bite, that is, fixing the bite at the level of the skull bones, requires additional surgical intervention. An orthognathic surgeon corrects the size and position of the jaws after installing braces and adjusting the position of the teeth. After the operation, the orthodontist details the position of the teeth for a perfect smile.
Distal occlusion (upper macrognathia, prognathia)
Distal bite therapy can be carried out using the following methods and methods:
- orthodontic treatment,
- hardware-surgical,
- surgical,
- prosthetic
- various combined and combined methods.
During treatment, taking into account certain features depending on the clinical form of the anomaly, the age of the patient, the individual characteristics of the structure of the facial skull and the type of its growth, the following tasks must be solved.
- Regulation during jaw growth using a facebow and extraoral traction or a functional apparatus.
- Restriction of growth and shortening of the dentition of the upper jaw due to the distal movement of the upper molars, canines and elimination of protrusion of the anterior teeth
- When treating distal occlusion, it is advisable to transfer form P2 to form II1, which can be achieved by using arches in the traditional sequence, that is, the primary arch, as a rule, is multi-stranded, flexible, allowing the creation of additional bends when teeth are crowded in order to avoid excessive load on them, then a steel one rectangular.
- Distal movement of the upper anterior teeth without or after extraction of individual teeth (most often premolars).
- Stimulation of growth and anterior movement of the lower jaw
- Expansion of the dentition of the upper and/or lower jaw
- Change in interalveolar height and normalization of the Spee curve.
- Normalization of the function of masticatory and facial muscles
- Retention period
It is not always possible to completely correct the anomaly during these manipulations, but a change in position of approximately 45 mm can be achieved. When planning orthodontic treatment of patients with distal occlusion, teleradiological examination data characterizing the type of growth of the maxillofacial complex, the activity of residual growth and their comparison with orthognathic occlusion are very important.
With a distal occlusion, the proportion of the neutral type of growth decreases (from 71% with orthognathic to 50%) in favor of horizontal, namely to 43% versus 15% with orthognathic. This indicates the predominance of development of the facial skeleton in the anteroposterior direction due to intensive growth of the upper jaw, especially in the period of 7-12 years and somewhat less in 12-15 years. That is why the most optimal for modifying jaw growth are the replacement bite and the earliest permanent bite (for 14-15 years, for 12-13).
In patients with a neutral type of growth of the facial skeleton, the main tasks when correcting a distal bite are, first of all, to restrain the growth of the upper jaw and stimulate the growth of the lower jaw. In such patients, mainly removable equipment of functional or combined action should be used.
With the horizontal type, it is necessary, first of all, to restrain the growth of the upper jaw, with simultaneous distal movement of the lateral teeth, using a face bow with a cervical traction. For adult patients, to reduce the upper dentition, treatment is recommended with the removal of the first premolars, followed by distal displacement of the lateral and anterior teeth. This is indicated for prognathia with a reduced or average size of the base of the upper jaw and for prognathia caused by crowding of the upper front teeth, their sharp protrusion, often together with the alveolar process.
In severe forms of distal occlusion with a pronounced horizontal gap, removal of the first premolars is indicated even in a mixed dentition. After this, when treating II1, you can use a flex arch, then a nitinol one, fixing them first on the teeth of the upper jaw. One of the indications for tooth extraction is a reduction in the retromolar space, which enhances the mesial displacement of the lateral teeth and aggravates the close position of the anterior teeth, with insufficient space for the canines of the upper and lower jaw (Zhulev E.N.).
According to WR Proffit (1986), the indication for serial extraction is a discrepancy between the size of the teeth and the dental arch by 10 mm or more, and Ringenberg (1964) believes that the initial value should be smaller, namely 7 mm. According to the point of view of V.P. Norkunaite, with the length of the segment of the dentition “from the distal surfaces of the crowns of the 12th and 22nd teeth to the mesial points of the sixth teeth” equal to 18.5-21.0 mm, and if the sum of the mesiodistal dimensions of the canines and premolars is 22.5-24, 0 mm, then removal of individual permanent teeth is indicated. It should be noted that non-extraction orthodontic treatment is even relatively simpler, since there is no need to move the teeth a significant distance to close the post-extraction gap.
As a last resort, removal of the second molar (sometimes unilateral) is used and distalization of the dentition is performed using a face bow. It is very difficult to move the first molars distally more than 1.5-2.0 mm even after removing the second molars, since distal tooth displacement is much more difficult than mesial displacement. The latter requires more reliable support and stabilization, as E. Engle wrote about. The extraoral thrust should not be low, otherwise extrusion of the molars will occur.
During the period of replacement teeth, when treating distal deep bite, you can use the forgotten but good method of A. Katz, namely, crowns with spikes on the second milk or first permanent molars (the tooth is not prepared) of the lower jaw. When the mandible is advanced forward, the elongated mesial cusps of the artificial crown should fit into the gap between the first and second primary molars of the upper jaw, widened by preparation. In this case, some separation of the bite occurs, which contributes to the dentoalveolar lengthening of the lateral teeth and a decrease in the incisal overlap. Long-term use of such crowns (8-10 months) leads to the formation of an orthognathic bite.
In children with mixed dentition and a clear tendency to develop distal occlusion, McNamara recommends maxillary expansion with overcorrection, usually a rapid maxilla expander. The subsequent use of a retention plate leads to the movement of the lower jaw to a position more convenient for the patient, pushed forward. This eliminates buccal crossbite and, after some time, improves occlusal relationships in the sagittal direction. Somewhat earlier, this phenomenon was explained by H. Taatz and Reichenbach by the fact that the expansion of the upper jaw contributes to the spontaneous displacement of the lower jaw to the anterior position. If such correction does not occur, then RG Alexander recommends the use of a facebow with extraoral traction until the end of the mixed dentition.
In mixed dentition, removable plate devices and a pre-orthodontic trainer are used in the treatment of prognathia.
But in addition to this, when treating anomalies at the dentoalveolar level, especially when combined with a narrowing of the dentition or crowding of teeth, fixed structures can be used. First of all, this is a “2 x 4” device, that is, rings for the first molars and braces for the 4 upper incisors, or utility arches.
Growth can be stimulated using activators, for example Andresen Haüpl or function regulators R.Fränkel. The activator is a removable two-jaw monoblock plastic, functional apparatus, consisting of upper and lower plates connected to each other; a vestibular arch, springs or a screw may be added to them. In addition to the plates adjacent to the inner surface of the alveolar processes, they have a corresponding bed for the oral surfaces of all upper and lower teeth. It is better to fix all types of plates with arrow-shaped clasps and Adams clasps.
The device holds the lower jaw in an extended anterior position (a constructive bite that must be determined by the doctor before treatment), promoting dentoalveolar lengthening in the lateral areas, while the upper anterior teeth are moved posteriorly due to a reciprocal action. On the upper jaw, the plate touches the mesial edges of the surfaces of the teeth, but lags behind the distal ones. On the lower jaw, on the contrary, it fits tightly to the distal edges and lags behind the mesial ones to move the lower jaw.
The clinical laboratory stages of production are as follows.
First clinical impression taking from both jaws; the first laboratory casting of plaster models and making a wax template for the upper jaw with bite ridges to determine the constructive bite, the boundaries of the wax template: in front are the cutting edges of the incisors, behind is a line passing through the middle of the crowns of the last molars, on the side is the chewing surface of the lateral teeth.
The second clinical stage is the determination of a constructive bite: the patient moves the lower jaw forward to a neutral relationship of the first permanent molars (1 class each), and he is asked to close his teeth until they come into contact with the wax. In this case, the separation of the dentition should exceed the “rest height” and it is necessary to monitor the position of the ridge and the coincidence of the midline. If in the position of the constructive bite the neutral closure of the sixth teeth is not achieved and the discrepancy is 45 mm, then this position is fixed. If the sagittal discrepancy exceeds 6 mm, the first activator is first prepared (at 45 mm), and after 6-8 months the second activator is prepared, but with the movement of the lower jaw to the neutral closure of the sixth teeth.
After fixing the constructive bite, plaster models with a wax template are handed over to the dental technician and the doctor gives him instructions:
- make an apparatus with or without a vestibular arch for retrusion of the upper anterior teeth (the shape is being specified),
- install a screw or other additional elements, springs, levers, lingual arches, etc. F.Ya. Khoroshilkina and WR Proffit proposed installing facebow tubes into the activator (bite blocks in the premolar area) in order to be able, along with the functional action of the device, to create additional distal and vertical force using extraoral traction.
Second laboratory stage: the models are plastered in an occluder, the wax template is removed, a plastic base is made, the listed parts or others (as directed by the doctor), the device is polymerized in a special double cuvette or in a regular one, increasing its vertical size
Third clinical stage: fitting the activator in the oral cavity, first to the upper dentition, and then to the lower one; the activator should fit tightly to the teeth, with lips closed; The rules for using and caring for the device are explained to the patient and the next visit is scheduled. During repeated visits, the device is adjusted in the direction of movement of the upper and lower lateral teeth. During the treatment process, the dental bed is polished according to the direction of movement of the teeth, that is, those that need to be moved in the palatal or lingual direction, and vice versa, the plate should fit tightly to those teeth that need to be moved in the vestibular direction. The device can mainly be used while at home or while sleeping. Treatment is especially successful in the early stages of distal and deep bites.
The device helps restore nasal breathing, since the child is forced to breathe more through the nose due to the closure of the oral fissure by the plate. But it is contraindicated if nasal breathing is completely absent. The activator also helps eliminate the habit of sucking fingers, tongue, lips and various objects. The vestibular deviation of the lower teeth can be prevented by the activator hood, which overlaps them by 1/3 of the height of the crowns, so the plastic in it is polished or the hood is completely removed. Similar actions, depending on the progress of treatment, are taken at each visit. You can also stimulate the advancement of the lower jaw using the Balters bionator.
Treatment of distal occlusion (II2) can be carried out in two stages. First, the upper anterior teeth are deviated, eliminating the blocking of the lower jaw, that is, subclass II2 is transferred to II1 using edgewise therapy, rotating the first molar. The latter should be the first step in the treatment of a class II anomaly if there is a tendency for mesial rotation of the molar around the palatal root. If orthodontic treatment II1 is carried out without tooth extraction, then sometimes it is enough to turn the first upper molar with its buccal surface posteriorly, which allows you to create an additional space of 1.5-3.0-4.0 mm and the subclass will move to II1. This can be done with the help of an extraoral yaga, the Gozhgarin palatal clasp, in which the ends of the clasp, curved in two planes, are fixed into the palatal locks on the molars. The device is activated by unbending the loop.
This treatment method can be used when a class II anomaly is combined with an open bite. To illustrate, we give an example from the clinical practice of Dr. P. Ngan et al.: an 8-year-old patient had closure of the molars on both sides according to E. Engle class II, a 5-millimeter sagittal discrepancy in the frontal area, an anterior open bite and lower retrognathia. The main goal of treatment was to delay the anterior growth of the upper jaw, transfer the molar relationship from class II to class I, reduce concomitant skeletal disorders and open bite.
The treatment apparatus consisted of an activator and an extraoral arch attached to it. Because the base plate of the device did not cover the vault of the palate, a connecting arch (diameter 1.2 mm) was used instead, which increased the space for the tongue. For fixation to the extraoral traction activator, a special tube with a diameter of 1.12 mm (0.045 inches) was mounted in the plastic between the upper and lower dentition. The force of extraoral traction was up to 400 grams on each side. Springs for tilting the front teeth were made of elastic steel wire with a diameter of 0.5-0.6 mm, the lower part of which was fixed with horizontal shanks in plastic. The vertical part of the springs had a point contact in the area of the necks of the teeth.
The mandibular part of the apparatus consisted of an incisal platform for advancing the lower jaw. When determining the constructive bite, the lower jaw moved forward until the incisors made direct contact. In patients with hyperactivity of the muscles of the perioral region, to reduce their effect, lip pads in the form of a “tear” according to R. Fränkel were used, which were located in the vestibule of the oral cavity parallel to the alveolar process. The ratio of molars according to class I. was achieved in about a year and at the same time the size of the open bite decreased, which led to an improvement in the lip relationship. The entire treatment lasted about 14 months.
Sometimes symmetrical or unilateral removal of premolars in the upper jaw is performed. At the second stage of treatment, the lower jaw is set in the correct relationship with the upper jaw. To do this, when there is a sharp narrowing of the lower dentition, it is expanded, and then, based on the clinical picture and X-ray data of the temporomandibular joints, sagittal movement of the lower jaw is carried out using plates with an inclined plane. There are a large number of varieties of plates, including those with an inclined plane. Depending on a particular clinical situation, the doctor selects the appropriate design.
A. Katz's bite block is used to treat prognathia in combination with a deep bite. A special feature of its design is an inclined plane and reversible clasps that bend over the cutting edges of the front teeth onto their vestibular surface. The plate does not adhere to the mucous membrane of the anterior part of the palate and the necks of the anterior teeth. When closing with an inclined plane, the lower teeth slide along its surface, trying to return from a forced (constructive) bite to its original position, and the lower jaw moves forward, and the upper teeth tilt towards the palatine side. In the lateral areas, due to the separation of the bite, a vertical restructuring occurs, that is, dentoalveolar elongation.
The fundamental clinical and laboratory stages of making a plate differ little from those described in the manufacture of the activator: obtaining impressions, making a wax composition of the plate with retaining and reversible clasps, determining the constructive bite, polymerization of plastic, fitting and application of the device.
It should be remembered that when treating distal occlusion in patients 15-20 years old, when using bite blocks before stabilization occurs, a double or “wandering” bite may be established, that is, in a position of physiological rest, the lower jaw is fixed in a neutral position, and during function it moves to the former (distal).
The devices proposed by R. Fränkel are called functional regulators, the main parts of which are side shields and pelota, which relieve the dentition from the pressure of the cheeks and lips. As a result, under the influence of the tongue, the growth of the apical base is stimulated in the transversal and sagittal directions. The parts of the apparatus are held together by metal arcs made of elastic wire. This skeletonization made it possible to increase the strength of the regulators, reduce the size of the plastic shields, lighten the apparatus and make it open in the frontal area for better swallowing and speech. Active elements (screws or springs) can be added to the device to accelerate the movement of individual teeth.
R. Fränkel proposed function regulators of three main types: type I (FR I) is used to eliminate protrusion of the anterior teeth and distal occlusion, combined with narrowing of the dentition, fan-shaped arrangement of the upper frontal teeth and with anomalies of 1 class. E. Engla; type II (FR II) for the treatment of distal occlusion of subclass 2 (II2), that is, in combination with deep overlap and retrusion of the upper anterior teeth; type III (FR III) for the treatment of progenia. The principal clinical and laboratory stages of the regulators have been described previously.
The use of this method is effective in early childhood (the period of primary and mixed dentition), that is, when one can count on the growth of the jaw bones and especially the apical base. Treatment with the regulator, especially during the period of its development, is recommended according to the following scheme: for the first two weeks use the device during the day for 1 hour, for the next 2 weeks every day for 2 hours, then during all free time, removing the device only during meals; in 2-3 months around the clock. After correcting the bite with adjusters, retention devices are not required, since already during the active phase of orthodontic treatment, the conditions that contribute to the occurrence of relapse are eliminated.
Sagittal movement of the lower jaw during prognathism should be considered as the last stage of treatment, based on the considerations that the restructuring of muscles, temporomandibular joints, as well as dentoalveolar lengthening in the lateral areas in the vertical direction are not always successful. When treating severe forms of prognathia with deep overlap, the separation between the lateral teeth should be at least 45 mm. With active protraction of the lower jaw, tissue restructuring occurs in the order of activation (stimulation) of functional hypertrophy, mainly of the lateral pterygoid muscle, which is poorly developed during prognathism.
It is necessary to constantly monitor the separation of the bite and, as contact between the lateral teeth is achieved, to re-create the separation of the bite by correcting the inclined plane. It is also necessary to correct the appliance in the area where its base adheres to the palatal surfaces of the anterior teeth. In most cases, a sagittally moved mandible is secured in its new position due to the close contacts of natural teeth or contacts created by dentures.
The use of devices can be combined with active myogymnastics, but they are incompatible with edgewise therapy, although it would be very desirable to correct the dentoalveolar components of the anomaly simultaneously with the correction of jaw growth. This is possible when using non-removable functional devices or when combining braces with a face bow. There is no point in drawing a sharp boundary between the phases of treatment, expecting, for example, leveling of the dentition, because extraoral appliances also contribute to a certain extent to the correction of the dental components of the anomaly.
RG Alexander is a proponent of the use of extraoral traction both for growing jaws (children, adolescents) and for adults. But in the first, with the help of a facial arch, the growth of the upper jaw is suppressed and at the same time its dentition is leveled, the lower jaw is unblocked, providing the opportunity to achieve its genetic potential. In adults, when growth has stopped, the main purpose of extraoral appliances is to hold the upper molars in place, to avoid their displacement forward.
Intermaxillary traction, in the author's opinion, should be used while the dentition of both jaws is aligned and stabilized, rigid end steel archwires are installed (0.17 x 0.25) and torque control is established to prevent incisor tilting. The arches must completely fill the slots of the braces and be in the mouth for at least a month before installing elastic traction according to class II. Having studied the vector of forces in the traditional position of the above-mentioned thrust, that is, from the upper canines to the lower first molars, RG Alexander determined the presence of an undesirable, very significant vertical component of the force. An increase in the horizontal component of the force can be achieved through a different fixation of the traction, namely, from the second lower molar to the spherical hook of the bracket on the upper lateral incisors. This increases the vector of horizontally acting force and reduces the tendency to “open” the bite, for which, by the way, elastics are not used in the “Vari Simplex Discipline” system.
When treating the first subclass (II1) of prognathia, complicated by a deep or open bite, the incorrect position of the teeth and an anomaly in the shape of the dentition are usually eliminated. If it is necessary to expand the lateral areas of the upper dentition, then a rapid palatal expander (rapid maxilla expander) is used in the early stages of treatment, before the installation of fixed appliances. If the teeth have not erupted, then plastic plates with a screw can be used, and only then the lower jaw is moved forward. When treating a distal bite in combination with protrusion of the upper anterior teeth, their close position and narrowing of the dentition or their asymmetry, one should not rush to eliminate the protrusion, since the upper anterior teeth, which have become palatally inclined as a result of treatment, will interfere with the movement of the lower jaw.
According to many clinicians, with early treatment, distal occlusion can be eliminated in approximately 80% of patients with functional devices. The use of edgewise therapy, in particular the direct arch technique, expands the age-related indications for orthodontic correction, but positive dynamics of treatment are observed only at the dentoalveolar level.
In case of distal occlusion (II2), the method of eliminating crowding of teeth must be planned taking into account the structure of the facial skeleton, the age of the patient and the amount of space in the dentition. The correct choice of method allows you to get an optimal result and avoid complications during and after treatment.
Treatment of adult patients is reduced mainly to leveling the position of the teeth and eliminating deep incisal overlap, if any. The process of “detailing” the molars is either prolonged (as a result of the “distalization” of first the second and then the first molars) or is impossible because adults already have erupted second and third molars. In such patients, extraction is more indicated, and a dilemma arises: which tooth should be removed, the first or second premolar? To resolve this issue it is necessary to take into account:
- the magnitude of the space deficit; if, after straightening the teeth, a residual gap of no more than 2.0 mm is predicted, then the first premolar is removed, and if it is more than 2.0 mm, then the second premolar; this choice can be argued by the fact that during the closure of the spaces between the teeth, the tendency for retrusion of the incisors increases, while the removal of the second premolar has a lesser effect on the position of the incisors;
- dental condition, it is preferable to remove the affected teeth (destroyed crown, endodontic treatment, changes in periapical tissues, large filling or severe abrasion);
- after extraction, it is necessary to retract the canines or “first premolar canines”, for which the full arch technique or the segmental arch technique can be used;
- The full-arch technique in its standard implementation is as follows: at the first stage, braces are fixed on all teeth, using for additional support, for example, a Gozhgarin clasp, when indicated in combination with a face bow; the initial arch, as a rule, is nitinol, with simultaneous “distalization” of the canine or first molar using an eight-shaped ligature (within the dentition this can be done using springs, elastic traction, elastomeric power modules); it should, however, be noted that in this case, a protrusive displacement of the incisors occurs, which is very undesirable in adults, since then it is necessary to retract them to eliminate the sagittal discrepancy, therefore it is better to use the segmental arch technique;
- segmental arch technique: braces are fixed only on the teeth of the lateral segment, with additional stabilization of the supporting teeth, as in the previous version; then a steel edge arch with a diameter of 0.40×0.55 mm is passively inserted into the braces; for “distalization” the usual sliding technique; if the canine has an abnormal position initially, then a nitinol arch should first be introduced, fixing it only in braces on the canines and premolars, with simultaneous “distalization” with an 8-shaped ligature; after normalizing the position of the fang, you can move on to a full arch and fixation of braces on the incisors, the leveling of which is carried out according to the traditional method (nitinol arch, steel arches, TMA); This technique allows for canine retraction without side effects on the incisors.
For surgical treatment, write down clear indications:
- justification for the need for such therapy, for example, the magnitude of the sagittal discrepancy of the jaws is 10 mm or more, the angle of the SNSs (SNA) on the teleroentgenogram is greater than normal, which is ~ 82°
- good state of somatic and mental health, the growth of the patient’s facial skeleton must be complete
- pronounced protrusion of the lower incisors (the angle of inclination is less than 70-80°, while the norm is 90-95°); it is well known that the vestibular movement of the lower anterior teeth is very limited and the limit depends on the value of the initial axial angle; the maximum reasonable limit should not be less than 90-95°, therefore, when using equipment for the vestibular movement of the lower front teeth, you need to be very careful; correction of the sagittal position of the lower anterior teeth can be carried out: by changing their vestibular inclination,
- changes in the length of the lower jaw, but this depends on the age and nature of micrognathia, that is, it is of the condylar type (when the articular process, which is the center of longitudinal growth, is affected) or extracondylar,
- changes in the position of the mandibular head, if the anomaly has developed due to distal displacement of the mandible
An approximate set of myogymnastic exercises for the treatment of distal occlusion. Exercises should be selected according to the child’s age and not be too difficult. L.S. Persia recommends first of all determining the level of development of the child and giving the load not to the point of fatigue, but approximately 75% of it. Exercises to correct a specific anomaly should be dosed and performed against the background of general physical exercise, starting 2-3 weeks before orthodontic treatment.
Muscle contractions must be performed with maximum amplitude, their intensity must be within physiological limits, with a gradual increase in speed and duration; between two successive contractions there should be a pause equal to the duration of the contraction itself.
Exercises to normalize breathing function (performed during morning exercises, physical education lessons or while walking); starting position: the state of correct posture: the head and torso are held straight, the shoulders are slightly pulled back and slightly lowered, the chest is turned out, the shoulder blades are adjacent to the back, the stomach is tucked and the knee joints are straightened.
Exercises to normalize lip closure (can be performed during speech development classes). Starting position: sitting in front of a mirror, head held straight, shoulders slightly pulled back and slightly lowered, chest turned out, knee joints bent, legs together, stomach tucked.