Acute sialadenitis on ultrasound
Inflammation of the salivary glands is called sialadenitis.
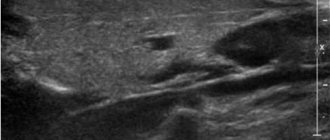
Acute bacterial sialadenitis develops when the infection is introduced hematogenously or through the excretory ducts, as well as from an open injury. Many viruses (for example, mumps virus, influenza, cytomegalovirus) have an affinity for glandular tissue, including the parenchyma of the salivary glands. In acute sialadenitis, a painful swelling appears in the area of the salivary glands, and the amount of saliva secreted decreases. As a rule, during viral infections several salivary glands are affected. In acute sialadenitis, ultrasound shows an increased size of the affected glands; the echogenicity of the parenchyma is reduced, often heterogeneous due to oval hypoechoic areas; the contour of the gland is clear and slightly convex; blood flow is often increased. It is likely to encounter enlarged regional lymph nodes with increased central blood flow. Acute sialadenitis is not characterized by dilated ducts, increased echogenicity of their walls, or hyperechoic inclusions in the parenchyma of the gland.
| Photo. With viral mumps on ultrasound, the parotid gland (A, B) is enlarged, the parenchyma is hypoechoic, heterogeneous due to small anechoic ovals, the color circulation determines dilated vessels; blood flow is noticeably increased (B). Conclusion: Echo signs of acute mumps. | ||
| Photo. A 5-year-old girl with a temperature of 38.6ºC, a wet cough and painful swelling in the parotid region on the right. On ultrasound, the right parotid gland (A, B) is enlarged, the parenchyma is hypoechoic, heterogeneous due to small anechoic ovals, the color circulation determines dilated vessels; blood flow is noticeably increased. The parotid gland on the left (B) is unchanged. In the general blood test, lymphocytosis, the level of IgM antibodies to the mumps virus is increased. Diagnosis: acute mumps. | ||
| Photo. A, B — On ultrasound, the parotid gland is enlarged, the contour is wavy, the parenchyma is hypoechoic, heterogeneous due to small almost anechoic ovals, probably dilated vessels; enlarged lymph nodes are detected. Conclusion: Echo signs of acute mumps, secondary lymphadenitis. B - Echo signs of acute parotitis in the main gland and accessory lobule. | ||
3. Symptoms and diagnosis
Sometimes sialolithiasis is accidentally discovered during dental radiography - either at the asymptomatic stage (when the size of the growing stone is not yet sufficient to cause noticeable discomfort), or in cases of the so-called. “silent” calculus (large enough, but immobile and does not impede the drainage of saliva). However, more often the patient is brought to the doctor by salivary colic - paroxysmal pain associated with eating in the affected area, which can be very intense (there is even a known case of a suicide attempt motivated by unbearable pain). Pain syndrome caused by complete or partial obstruction of the salivary duct, swelling and, in many cases, profuse suppuration due to an acute infectious-inflammatory process, severe limitation of the ability to eat, articulation disorders due to painful movements of the tongue, fever up to 38-39 degrees with a corresponding general malaise - all these symptoms are typical for the clinically pronounced stage of calculous sialadenitis (note that this diagnosis is literally translated as “stone-related inflammation of the salivary gland”).
To establish a diagnosis, in most cases, it is sufficient to have specific complaints, the results of examination and palpation, as well as confirmatory radiography (including contrast sialography). Ultrasound is sometimes used.
About our clinic Chistye Prudy metro station Medintercom page!
Chronic sialadenitis on ultrasound
Congenital disorders of the development of ducts and glandular tissue, salivary gum disease, as well as autoimmune diseases contribute to the development of a chronic inflammatory process in the salivary glands. Regardless of the cause, there are three stages of chronic inflammation: initial, clinically pronounced and late. In each stage there are periods of exacerbation and remission. In chronic sialadenitis on ultrasound, the parenchyma is hypoechoic, heterogeneous due to point and linear hyperechoic inclusions, the contour is uneven. During the period of exacerbation of large iron, its echogenicity is significantly reduced. During the period of remission, the size of the gland decreases and its echogenicity slightly increases. The decrease in the echogenicity of the gland is due to swelling of the parenchyma and hyperplasia of the intraglandular lymphoid tissue. Hyperechoic inclusions appear when parenchyma is replaced by fibrous tissue. Due to severe fibrosis in the later stages, the iron decreases in size.
| Photo. On ultrasound, the parotid gland on the right (A, B) is enlarged, the parenchyma is hypoechoic, heterogeneous due to small anechoic ovals and linear hyperechoic inclusions. The parotid gland on the left is unchanged. Conclusion: Echo signs of chronic mumps. | ||
| Photo. On ultrasound, the parotid gland is enlarged, the parenchyma is hypoechoic, heterogeneous due to small anechoic foci, point and linear hyperechoic inclusions; the vessels are dilated and blood flow is increased. Conclusion: Echo signs of chronic mumps. | ||
Sjögren's syndrome is a chronic autoimmune disease, predominantly affecting women over 40 years of age, in which lymphocytes and plasma cells intensively infiltrate and destroy the salivary and lacrimal glands. The main complaints of Sjögren's syndrome include dry mouth and keratoconjunctivitis, as well as arthritis. The disease often affects all salivary glands. In Sjögren's syndrome, ultrasound shows that the salivary glands are enlarged, the parenchyma is heterogeneous due to diffusely scattered multiple hypo- or anechoic oval foci; blood flow is usually increased. It is believed that hypo- and anechoic foci are lymphocytic infiltrates against a background of unchanged parenchyma. In the presence of lesions larger than 2 cm and rapid growth, a biopsy is recommended.
| Photo. A 50-year-old man complains of dry mouth and keratoconjunctivitis. On ultrasound, all salivary glands are enlarged, the parenchyma is hypoechoic, heterogeneous due to small hypoechoic foci and linear hyperechoic inclusions. Conclusion: Echo signs of chronic sialadenitis. Diagnosis: Sjögren's syndrome. | ||
A special form of chronic sialadenitis is chronic sclerosing sialadenitis or Küttner's tumor, when a persistent painful tumor appears in one of the salivary glands. This disease is rare and most often affects the submandibular gland. Microscopy reveals atrophy of glandular tissue, dense fibrosis, and periductal lymphocytic infiltrates. Sialoliths and mucus plugs are often found in altered ducts. It remains unclear whether they are a cause or a consequence of the inflammatory process. Some authors suggest that thick secretion blocks small ducts, which leads to inflammation, fibrosis, and atrophy of glandular tissue. Other authors point to the autoimmune nature of the pathology. With Küttner's tumor, ultrasound reveals diffuse parenchymal damage in the salivary gland: multiple round hypoechoic foci. Less common is a focal lesion: a hypoechoic heterogeneous focus against the background of unchanged parenchyma, which simulates a malignant process. In all doubtful cases, a biopsy is recommended. Chronic sclerosing sialadenitis is an exclusively benign inflammatory disease. Often the affected gland has to be removed; no additional treatment is required.
How is an ultrasound of the salivary glands done?
Ultrasound of the salivary glands has two methods:
- from the outer surface;
- from the inside of the oral cavity.
The specialist will need about 15-20 minutes to complete the procedure. The patient does not feel any discomfort at this time. The person is in a supine position, and the head is placed on a special pillow and slightly tilted back. Sometimes the doctor asks you to turn your head to the left or to the right. During ultrasound of the parotid region, the transducer is placed near the ear. When examining the sublingual and submandibular glands, the device is installed in the oral cavity. According to the protocol, the doctor examines each salivary gland separately and describes all pathologies, measurements (width, thickness and length) and changes in the norm in detail in the conclusion.
Sialosis (sialoadenosis) of the salivary glands on ultrasound
Sialosis (sialoadenosis) is a non-inflammatory and non-malignant, recurrent, often painless, usually bilateral enlargement of the salivary glands. The causes of sialosis are unclear. Sialosis occurs in patients with endocrine and autoimmune diseases, liver cirrhosis, chronic alcoholism, vitamin deficiencies, etc. With sialosis, ultrasound reveals enlarged hyperechoic salivary glands, but without focal changes and increased blood flow.
| Photo. On ultrasound, the submandibular (A, B) and parotid (C) glands are enlarged, the parenchyma is hyperechoic, poorly transmits ultrasound waves (the posterior contour of the gland is not visible), homogeneous, the blood flow is not changed. Conclusion: Echo signs of sialoadenosis. | ||
Inflammation of the lymph nodes in the salivary glands on ultrasound
The parotid glands contain a large number of lymph nodes that collect lymph from the upper jaw, lips, mouth, cheeks, outer parts of the nose, upper and lower eyelids, temporal and frontal regions, outer ear and tissues of the parotid-masticatory region. Inflammatory disease in these areas causes a reaction in the lymph nodes of the parotid glands. Inflammation of the intraglandular lymph nodes imitates mumps. Misdiagnosis here is unacceptable, since mumps and lymphadenitis have different management tactics and prognosis.
Important!!! With bacterial lymphadenitis, the infection lymphogenously penetrates into the regional lymph nodes through the “entry gate”. Viral infections hematogenously affect the lymph nodes of several anatomical areas.
Ultrasound with acute serous lymphadenitis within the parotid gland reveals an oval-shaped anechoic formation with clear and slightly wavy contours, often with central blood flow - an inflamed lymph node. Inflammatory edema and infiltration of the tissues surrounding the lymph node (periadenitis) lead to the development of lymphogenous sialadenitis (pseudosialoadenitis). A painful, diffuse swelling appears and the amount of saliva decreases. On ultrasound with lymphogenous sialadenitis, the echogenicity of the parenchyma is reduced, an almost anechoic lymph node is determined; the contour of the lymph node is often not clearly visible, which does not always indicate destruction of its capsule. With a positive outcome, the size of the lymph node decreases, its echogenicity increases, and the contour becomes clearer.
| Photo. Ultrasound of the parotid gland: the echogenicity of the parenchyma is not changed, heterogeneous due to oval-shaped hypoechoic foci with a central scar. Conclusion: Echo signs of reactive lymphadenitis. | ||
Purulent lymphadenitis on ultrasound differs little from acute serous lymphadenitis - an oval-shaped anechoic focus, but as the intensity of the reflected signal increases (GAIN regulator) with purulent melting of the lymph node in the peripheral sections (parietal), point inclusions of medium echogenicity appear, while the central sections the lymph node remains without inclusions. The clarity of the contours and the oval shape indicate the preservation of the capsule of the lymph node during its purulent melting - this is a forming abscess in the salivary gland. An anechoic area of uncertain shape with unclear and uneven contours due to purulent melting of the lymph node and its capsule is adenophlegmon of the salivary gland.
| Photo. On ultrasound, both parotid glands are enlarged, hypoechoic, heterogeneous due to hypo- and anechoic foci. Conclusion: Echo signs of multiple microabscesses. | ||
| Photo. A 2-year-old child with swelling in the parotid region on the right. On ultrasound, the right parotid gland is noticeably enlarged, heterogeneous due to many hypo- and anechoic foci with acoustic enhancement behind and increased blood flow along the periphery. Conclusion: Echo signs of a formed abscess in the parotid gland. | ||
Long-term entry of low-virulent flora into the lymph nodes or inadequate treatment of acute serous lymphadenitis can lead to chronicity of the inflammatory process. An enlarged lymph node in chronic lymphadenitis on ultrasound is hypoechoic, oval in shape with clear contours and (necessarily!) inclusions of high echogenicity in the center. It is the presence of echogenic inclusions in the central parts of the lymph node that confirms the existence of a chronic inflammatory process.
1.General information
Sialolithiasis, or calculous sialadenitis, is the formation of calculi (stones) in the salivary gland, which is reflected in the Russian term “salivary stone disease.” This disease was known back in the time of Hippocrates, but to this day many of its aspects remain virtually unstudied.
Thus, thanks to special medical and statistical studies, the true epidemiological picture of sialolithiasis, which 2-3 decades ago was considered a rare pathology and of interest mainly to specialists, began to become clearer. In fact, it turned out that it is sialolithiasis that underlies a significant proportion of clinical syndromes and symptom complexes that sooner or later require the intervention of a maxillofacial surgeon. Frequency estimates in different sources still differ widely (the specific share of sialolithiasis in the total volume of diseases of the salivary glands is today estimated in the range from 30% to 80%), but it is already obvious that the problem is much more pressing than previously seen.
Data have been published showing that salivary stone disease is more common in men. Other authors do not find a reliable statistical dependence on gender, however, in the studied samples of patients, they reveal a three-fold predominance of city dwellers over rural residents. Even greater discord is observed in estimates of age-related incidence trends: data is provided that sialolithiasis is most often found in children of early school age, but the results of other studies refute this, and the age of primary primary diagnosis of salivary stone disease is determined in the range of 30-40 years.
Statistics of predominant localization, on the contrary, are distinguished by uniformity of estimates: in the vast majority of cases (more than 90%), sialolithiasis affects the submandibular gland, much less often detected in the parotid gland, and extremely rarely in all other salivary glands - sublingual or small (palatal, molar, buccal, etc.) .d.).
A must read! Help with treatment and hospitalization!
Salivary stone disease on ultrasound
Salivary stones are most often located in the submandibular gland (60-90% of cases) and can be multiple. The parotid glands are affected in 10-20% of cases. Stones can form due to metabolic disorders. Therefore, it is often possible to trace the hereditary nature of the disease. A rather characteristic combination of salivary stone disease and a chronic inflammatory process in the gland.
Sialilithiasis causes partial or complete mechanical obstruction of the salivary duct, which leads to recurrent swelling of the salivary gland during meals and may be complicated by bacterial infection. Sialoliths in the distal submandibular duct can be palpated at the base of the mouth.
Important!!! In preschool children, the role of a calculus can be played by foreign bodies of the submandibular ducts, which enter the ducts through gaping orifices. Such foreign bodies are often toothbrush lint, wood chips from pencils, seed husks, blades of grass, etc.
Calcified stones in the duct of the salivary gland are visible on ultrasound in the form of hyperechoic point or linear inclusions with a pronounced distal acoustic shadow. The duct proximal to the stone is usually dilated.
Only 20% of sialoliths are radiopaque. Uncalcified stones in the salivary gland duct are visible on ultrasound as inclusions of medium or high echogenicity without a distal acoustic shadow. Air bubbles mixed with saliva can mimic stones. An enlarged intraglandular duct indicates the location of the hyperechoic inclusion within the duct, and not in the parenchyma of the gland.
| Photo. Cross section of the parotid gland: 1 - parotid gland, 2 - excretory duct, 3 - stone with an acoustic shadow behind in the distal part of the excretory duct, 4 - masticatory muscle (m. masseter), 5 - ascending arch of the mandible, 6 - buccal muscle ( m. buccinator). | ||
| Photo. A, B — Stones in the excretory duct of the submandibular gland. B - Small stones in the excretory duct of the parotid gland. | ||
| Photo. The parotid gland is enlarged, echogenicity is reduced, somewhat heterogeneous due to small hypoechoic foci, blood flow is increased; the excretory duct is greatly expanded, in the distal section a hyperechoic inclusion with an acoustic shadow behind is determined. Conclusion: dilation of the excretory duct of the parotid gland, echo signs of a calculus in the distal part, secondary parotitis. | ||
How is sialadenitis treated?
Regardless of the form and type of disease, the patient is given antibacterial therapy. If the course of the disease is mild, then it is enough to undergo a course of physiotherapy and take several injections of antibiotics directly into the inflamed duct of the salivary gland. If acute sialadenitis of the salivary glands is of moderate severity, then painkillers and a course of antibiotics (10-14 days intramuscularly) can be prescribed.
Severe sialadenitis, characterized by the formation of stones in the salivary ducts, requires surgical intervention. For small stones, an ultrasonic crushing procedure is recommended. For larger ones, endoscopic surgery is performed.
Physiotherapy is prescribed:
- therapeutic massage of the salivary gland;
- electrophoresis;
- UHF;
- galvanization.
Most often, the acute form of the disease has a favorable prognosis. With proper treatment, recovery occurs within two weeks. It is important to identify the pathology in time, so the primary diagnosis of sialadenitis in children falls under the responsibility of the parents. If a child begins to complain of pain in the ear, discomfort when swallowing, or an unpleasant taste in the mouth, then you should immediately contact your pediatrician. Even before the appearance of characteristic and pronounced symptoms, swelling of the neck and slight redness of the neck and face are possible - these are also alarming symptoms.
Salivary gland cysts on ultrasound
Simple cysts are uncommon in the salivary glands. They can be congenital or acquired. Some acquired cysts develop due to obstruction of the salivary ducts in the presence of tumor, stones, or inflammation. Clinically they appear as a painless tumor. On ultrasound, simple cysts are defined as avascular anechoic lesions with a clear contour and posterior acoustic enhancement.
Retention cysts of the sublingual glands are located under the tongue on one side of the frenulum of the tongue: sometimes the cyst displaces the frenulum, but never moves to the opposite side. On palpation, a soft, elastic, painless swelling of a round or oval shape with a smooth, slightly wavy surface is determined. Being covered with a thinned mucous membrane, retention cysts have a characteristic cyanotic or bluish tint. On ultrasound, a small retention cyst (up to 2.0 cm in size) is visible as an anechoic formation, on one side of the frenulum and fibrous septum of the tongue; the outer and anterior contour are not clearly defined, since in these places the cysts are adjacent to the lower jaw. Retention cysts grow slowly. Sometimes they penetrate through the mylohyoid muscle into the submandibular region. If the cyst is large, the wall can be damaged when eating solid food (baking bags, crackers, candies, etc.). If the cyst empties completely, it cannot be detected on ultrasound. The cyst begins to grow again as fluid accumulates in it. In long-term large retention cysts there is often a suspension of medium echogenicity.
| Photo. A — Retention cyst of the sublingual gland. B — Ultrasound shows a simple cyst of the parotid gland. B — Ultrasound shows a complex cyst of the parotid gland. Such cysts require additional research. | ||
Classification of sialadenitis, causes and symptoms
Sialadenitis of the parotid gland. These are the largest glands in the human body, located above and below the auricle. Most often, the cause of the pathology is a viral epidemic infection - mumps. It occurs in childhood. Signs of sialadenitis of the parotid salivary gland are quite pronounced - pain behind the ear when swallowing food, constant dry mouth, swelling of the neck and part of the face.
Sialadenitis of the submandibular salivary gland. May be bacterial, viral or fungal. Pathology in these glands is diagnosed much less frequently than in the parotid glands. The symptoms will be identical, but pain will be added when opening the mouth wide and chewing food normally.
Calculous sialadenitis is most often diagnosed at the age of 7-12 years. Inflammation usually develops in the submandibular salivary glands. The causes of calculous sialadenitis lie in the penetration of an infectious agent from other pathological foci into the oral cavity.
Sublingual sialadenitis. Its symptoms are intense and greatly disturb the patient - the sublingual area swells, becomes noticeably red, the patient is forced to constantly keep his mouth slightly open, he has difficulty breathing, and eating solid food becomes impossible.
In medicine, the types of the disease in question are distinguished by the location of the pathological focus. This classification is carried out in relation to the chronic form:
- parenchymal sialadenitis - inflammation occurs only in one part of the salivary gland, namely in the parenchyma;
- interstitial sialadenitis – pathology develops in the connective tissue of the salivary gland;
- sialodochitis - changes under the influence of the inflammatory process occur in the structure of the salivary duct.
In addition, a distinction is made between serous and purulent forms of the disease. And if in the first case the general condition of the patient remains within normal limits, then the symptoms of purulent sialadenitis are high body temperature, acute pain when swallowing even water, severe swelling and dizziness.
Benign tumors of the salivary glands on ultrasound
The most common benign neoplasms of the major salivary glands are polymorphic adenomas and Warthin tumors (adenolymphoma, cystadeniolymphoma). They grow slowly and may be asymptomatic. It is not possible to make a final diagnosis based on ultrasound alone.
Polymorphic adenomas are most common in the parotid gland (60%-90%) in people in the fourth and fifth decades of life, but can occur at any age. Polymorphic adenoma (pleomorphic adenoma, mixed tumor) is a benign tumor with a well-defined fibrous capsule, has slow expansive growth, and is not prone to malignancy, metastasis and relapse. One of the previously existing names for this tumor, fibrochondromyxoepithelioma, indicates that this tumor develops from two germ layers (meso- and ectoderm). Polymorphic adenoma is very diverse and can be represented by both homogeneous dense masses of a grayish color, and mushy masses, areas of mucus with a soft gelatinous consistency, cartilaginous tissues with islands of ossification. Polymorphic adenoma of the salivary glands on ultrasound looks like a round or oval formation of reduced or low echogenicity with a clear, even or coarsely wavy contour. The echogenicity of polymorphic adenoma can be from slightly reduced to low and almost anechoic. The echostructure of the tumor can be homogeneous or contain many pinpoint inclusions of high echogenicity, randomly distributed throughout the tumor, or have large zones with inclusions of medium echogenicity. Blood flow in polymorphic adenoma is often poor or absent, but may be abundant.
| Photo. Polymorphic adenomas of the parotid gland on ultrasound: A - Hypoechoic focus with a wavy contour, almost homogeneous echostructure, blood flow in the center and along the periphery of the focus is increased. B — Hypoechoic focus with a wavy contour, heterogeneous due to hyperechoic foci. B — Hypoechoic focus of lobular structure, heterogeneous due to hyperechoic inclusions. | ||
Important!!! After unsuccessful surgery, polymorphic adenomas can recur multifocally. Untreated pleomorphic adenomas can undergo malignant changes after decades.
Infantile hemangiomas are the most common parotid tumor in infants. Like infantile hemangiomas of other areas, it is benign, appears soon after birth, grows quickly, and spontaneously regresses after 18 months. Surgery is usually not required. On ultrasound, in the projection of the parotid gland, a lobulated hypoechoic formation with a clear contour and extreme vascularization is found.
Warthin's tumor (adenolymphoma, cystadeniolymphoma) accounts for 5-10% of all benign neoplasms of the salivary glands and occurs more often in men in the fifth and sixth decades of life. In 10-60% of cases, Warthin tumors can occur at two or more points, grow and appear at different times. Warthin's tumors are benign; extremely rarely, the epithelial component can undergo malignant transformation. Adenolymphomas consist of a bilayered eosinophilic epithelium and lymphoid stroma. The epithelium forms various glandular and papillary structures: solid, cystic, lobular, papillary. Warthin's tumors on ultrasound are oval, hypoechoic lesions with a clear contour, often containing multiple anechoic areas. Warthin tumors are often hypervascularized but may also contain only short segments of vessels.
| Photo. Warthin tumors on ultrasound. | ||
Cystic lymphangioma occurs from dilated lymphatic vessels when drainage is impaired. Lymphangiomas are not true tumors, but malformations of the lymphatic system. Lymphangioma of the parotid gland is manifested by the presence of an extensive painless formation of soft elastic consistency without clear contours. The color of the skin over the lymphangioma remains normal. Lymphangioma of the parotid gland can extend to adjacent areas (temporal, buccal and submandibular), as well as to the superolateral parts of the neck. Lymphangiomas increase with colds. In this case, the lymphangioma becomes denser and even painful. Inflammation and even suppuration of lymphangioma is often observed, which is accompanied by an increase in volume, thickening, pain that sharply increases with palpation, a change in the color of the skin over the lymphangioma, a local and general increase in temperature. Cystic lymphangioma on ultrasound is visible as an anechoic cavity formation of irregular shape with clear contours, easily changing with pressure. In the lymphangioma cavity, septa are usually visible. The walls of the cysts are relatively thick, up to 1-3 mm, and may contain blood vessels, nerves, and adipose tissue. An inflamed lymphangioma on ultrasound is characterized by greater resistance of the cavity to compression and a convexity of the outer contour, the septa become thicker and more noticeable, and multiple point inclusions appear in the cystic fluid. With hemorrhage, the lymphangioma changes from anechoic to hypoechoic.
| Photo. Cystic lymphangioma. | ||
The parotid gland contains its own veins and transit venous lines - the superficial temporal vein, the mandibular vein, the maxillary vein, therefore, of the hemangiodysplasias in the parotid glands, venous dysplasia or isolated phleboectasis are most common. Venous dysplasia can spread beyond its borders. Large venous nodes located in the subcutaneous tissue and skin create a characteristic clinical picture. Deep venous dysplasia manifests itself as a painless swelling of soft elastic consistency with unclear contours. A characteristic clinical sign of venous dysplasia is an increase in the size of this formation when the child strains or cries, as well as when the head is tilted or in a horizontal position. In a calm state, venous dysplasia on ultrasound is represented by an area of reduced echogenicity of an indeterminate shape with uneven and unclear contours. When performing the Valsalva maneuver, the characteristics of the zone of change change dramatically: its echogenicity decreases, its contours become clearer, and its shape becomes more rounded. This technique allows you to confidently differentiate venous dysplasia from all other diseases of the parotid gland.
Diseases of the salivary glands
Inflammatory diseases of the salivary glands
Nonspecific sialadenitis in children compared to other inflammatory diseases of the maxillofacial area, according to our data, is 14%. Chronic inflammatory diseases of the salivary glands in children are observed in the parotid (88%) and submandibular (3%) salivary glands; in sublinguals - not detected. In the submandibular salivary glands, the chronic inflammatory process occurs as calculous (9%).
Mumps of the newborn Clinical picture: The disease develops acutely in the 1st week of a child’s life. A dense diffuse inflammatory infiltrate of one or two parotid-masticatory areas appears, accompanied by severe general intoxication. After 2-3 days, purulent or purulent-necrotic melting of the gland occurs with the development of phlegmon in the parotid-masticatory area.
Treatment: From the onset of the disease, intensive drug antibacterial, anti-inflammatory and detoxification therapy is carried out with active resuscitation measures. In case of purulent melting of the gland - early surgical opening of the lesion with incisions along the lower edge of the zygomatic arch and in the submandibular region with drainage of the wound and local effects on it.
Mumps (mumps, mumps) is an acute infectious disease caused by a filterable virus that spreads by airborne droplets; the possibility of infection through household items and toys contaminated with the patient’s saliva cannot be ruled out. The mumps virus causes the formation of antibodies in the body in the first 3-8 days of illness. At this time, patients are contagious. The incidence is epidemic. Children aged 3 to 8 years are especially susceptible to the disease.
Treatment is symptomatic: bed rest, diet (non-salivation), hyposensitizing, restorative therapy, ointment dressings of anti-inflammatory absorbable type, physiotherapeutic procedures.
Cytomegaly is a viral disease observed in newborns and infants, weakened, and premature; described in children with congenital malformations of the lip and palate. The causative agent is a virus from the herpes group.
Chronic nonspecific parenchymal sialadenitis in children is the most common among inflammatory diseases of the maxillofacial area in children. There are interstitial, parenchymal sialadenitis and sialodochitis; In children, parenchymal parotitis predominates.
Tumor-like formations from glandular epithelium
Tumor-like formations from the glandular epithelium include cysts and tumors of the salivary glands. Salivary gland cysts are retentional in origin. In terms of frequency, they occupy first place among all tumors and tumor-like formations of the oral cavity in children (71% of tumor-like ones). Most often, retention cysts of the minor salivary glands are observed. Of the large salivary glands, cysts are most common in the sublingual gland.
In young children, a large cyst interferes with sucking and swallowing, and sometimes makes breathing difficult. In older children, speech is impaired. Palpation of the tumor is painless, and a clear ripple is detected.
Cysts of the sublingual salivary gland are most often formed in the posterior part, and cystic dilatation of the submandibular duct is observed mainly in the anterior parts of the sublingual region. This formation only slightly raises the hyoid ridge, without giving the mucous membrane a characteristic bluish tint, as with the cysts discussed earlier. In some cases, during differential diagnosis, to select a rational type of operation, it is necessary to resort to echography and sialography. The cyst is differentiated from cystic or cavernous lymphangioma.
The choice of treatment method depends on the size of the formation and the age of the child. Surgery for cysts of the sublingual salivary gland is performed with removal of the salivary gland in an inpatient setting, regardless of the child’s age.
Tumors of the salivary glands are divided into epithelial, nonepithelial, and unclassified. Tumors of the salivary glands are rare in children, which is the reason for the high frequency of diagnostic errors.
Salivary stone disease of the submandibular salivary glands Salivary stone disease of the submandibular salivary glands is a chronic, long-lasting disease caused by the presence of a stone in the excretory duct of the gland and accompanied by sialadenitis. Salivary stone disease is rare in children.