What can inflammation of the salivary gland ?
Read the answer to this question in this article. The human body is a complex mechanism consisting of a huge number of organs and systems. Several structures are responsible for performing the same function, constantly complementing each other. For example, different organs take part in the digestion process.
In the human body during normal development there are three pairs of salivary glands
The parotid gland is most often affected by various diseases. There are a number of diseases in which the sublingual and submandibular salivary glands become inflamed. If you do not start treatment on time or undergo inappropriate therapy, then serious complications may occur after such diseases, such as encephalitis, orchitis, meningitis, nephritis, neuritis and pancreatitis. However, do not worry, treatment often gives positive results. To avoid inflammation of the salivary glands, you just need to follow a few recommendations.
Treatment of diseases of the salivary glands
Diseases of the salivary glands in humans are quite common. The goal of the work of specialists at the Center for Maxillofacial Surgery and Implantology is to alleviate the patient’s condition and eliminate the causes of inflammation, as well as prevent its development and relapses.
Solid experience in working in situations of varying complexity, including operations on the salivary glands, the possibility of early diagnosis of diseases using high-precision equipment, an individual approach to each patient and the presence of a hospital for rehabilitation after surgical interventions are among the advantages of our center.
Inflammatory diseases of the salivary glands
They come in two types - large and small. The major salivary glands include the parotid, sublingual and submandibular glands. Inflammatory processes in the glands are called sialadenitis. The disease can be bacterial or viral in nature, develop in isolation and spread to adjacent tissues and organs. Typically, inflammation of the salivary glands occurs as complications of another disease, but can also appear independently. Diseases of the salivary glands can also be unilateral or bilateral.
Since the parotid glands are the largest and are more susceptible to the adverse effects of external factors, they are affected more often than others. Inflammation of the parotid salivary glands - mumps, or mumps.
Symptoms of inflammatory disease of the salivary glands:
- Dry mouth, which occurs due to a reduction in the amount of salivary gland secretion.
- A tugging or shooting pain that is felt directly in the area where the salivary gland is affected. The pain may radiate to the neck, ear, or mouth.
- Pain when chewing, swallowing, opening the mouth.
- Redness of the skin in the projection of the gland.
- Unpleasant odor and taste in the mouth.
- Compaction in the affected area.
- A feeling of fullness and pressure in the area where the gland is located.
- Increased body temperature, chills.
- General deterioration of condition.
- A breakthrough of an abscess from the gland into the oral cavity or onto the surface of the skin.
Benign tumors of the salivary glands.
Polymorphic adenoma and adenolymphoma of the salivary gland are neoplasms that occur most often. They can develop at any age and account for 1–2% of all cases of benign neoplasms diagnosed. Usually the disease develops on one side; its symptoms are asymmetry of the face and neck, enlargement of the gland, pain. Bilateral tumors are observed much less frequently.
As a rule, the tumor affects the parotid salivary gland. The neoplasm grows infiltratively, due to which it can affect the facial nerve, causing paralysis or paresis of its branches. Tumors of the glands can spread to the lower jaw, the mastoid process of the temporal bone, into the oral cavity and under the base of the jaw.
Types of benign tumors of the salivary glands
Adenoma usually affects the parotid glands. It grows slowly and has an elastic consistency. The affected gland may not hurt for several weeks or months, so it is not always possible to independently detect a tumor at an early stage. The neoplasm is easily displaced relative to the gland and is separated from normal tissue by a capsule.
Polymorphic adenomas account for more than 60% of cases of all diagnosed glandular tumors. They also grow slowly. In this case, several tumor buds are found in the gland. The capsule separating the healthy gland from the tumor is leaky. Due to this, the neoplasm can be adjacent directly to the parenchyma of the glands.
Polymorphic adenoma in the gland has a complex heterogeneous structure. In 6% of cases it turns into a malignant neoplasm, and then the gland begins to be affected very quickly. To exclude the development of a malignant tumor in the gland, it is necessary to carry out diagnosis as early as possible. Our center uses safe research equipment, so the doctor can accurately identify it and prescribe effective treatment.
Malignant lesion of the salivary gland
If you do not pay attention to treatment for damage to the salivary glands, benign neoplasms can turn into a malignant form. Especially often, inflammation develops inside polymorphic adenoma of the salivary glands.
If you experience discomfort in the salivary gland area or experience other symptoms listed above, you should contact a specialist as soon as possible. Blockage of the salivary canal makes it impossible to separate secretions and affects the condition of both the gland itself and the digestive processes. Speech becomes difficult, aesthetic problems arise, and a general deterioration of the condition is observed.
In most cases, malignant tumors of the glands are treatable, but a lot depends on the time of contacting a specialist and on his professionalism. It is easiest to prevent damage to other glands that play a decisive role in controlling body systems in the early stages. Upon completion of the rehabilitation period, the salivary gland will function normally.
Treatment of damage to the salivary glands
It is easier and more comfortable to treat the disease at an early stage. Innovative diagnostic methods used at the Center for Maxillofacial Surgery make it possible to detect diseases at the initial stages of development and accurately determine their nature. Therapeutic treatment of inflammation of the gland is carried out using modern drugs and physiotherapeutic equipment. Damage to the gland must be dealt with comprehensively and professionally.
In more complex cases, the lesion is eliminated surgically. The specialists of our center have extensive experience and successfully perform operations on the salivary gland. After surgery, you can continue treatment in our hospital. Comfortable rooms and round-the-clock supervision by doctors make it possible to achieve complete elimination of the disease and restore the function of the glands.
The salivary glands can become inflamed not only in adults, but also in children. Our specialists will find an approach to every young patient, and the stay in the children's hospital will be as comfortable as possible for both the baby and his parents.
Three types of inflammation of the salivary gland
Depending on the disease, there are three types of inflammation, namely catarrhal, purulent and gangrenous. First of all, a swelling forms in the area of the salivary gland, which is often accompanied by pain. The inflamed area becomes red, and the skin there is tense and shiny. The exit site of the gland duct has a limited area of edema and inflammation.
In most cases, a specific liquid is released from it, similar to saliva or pus. Body temperature rises sharply to 39 degrees. Opening your mouth becomes more and more difficult and painful. If treatment is not started on time, the disease will develop into a more severe form with serious consequences.
Theory and practical experience in ultrasound diagnosis of salivary gland pathology
Ultrasound scanner HS70
Accurate and confident diagnosis.
Multifunctional ultrasound system for conducting studies with expert diagnostic accuracy.
In domestic and foreign literature there are many works devoted to sialogy (from the Greek Sialon - saliva and logos - study) - the science of diseases and injuries of the salivary glands, methods of their diagnosis and treatment. According to various authors, diseases of the salivary glands account for up to 24% of all dental pathologies. Currently, in clinical practice, the most common are dystrophic, inflammatory diseases of the salivary glands (sialoadenoses, sialadenitis), as well as tumors and congenital malformations of the salivary glands. In addition, pathological changes in the salivary glands often accompany other diseases (diabetes mellitus, bronchiectasis, sarcoidosis, liver cirrhosis, hypertriglyceridemia, lymphogranulomatosis, etc.).
Various instrumental methods are used to diagnose diseases of the salivary glands [1]:
- radiography (if the formation of stones in the ducts of the salivary glands is suspected, but in 20% of the stones of the submandibular salivary glands and 80% of the parotid salivary glands are non-radiographically opaque);
- sialography (examination of the ducts of the salivary glands with a radiopaque substance, is rarely useful in differentiating tumors from inflammatory processes, but it can help differentiate the mass formation of the salivary glands from formations in neighboring tissues. In patients with suspected autoimmune disease of the salivary glands, a characteristic pattern of saccular expansion may be detected ductal system. In case of acute infection of the salivary glands, sialography should not be performed [2]);
- computed tomography together with sialography;
- ultrasound method (is the most accessible, safe and informative in the process of differential diagnosis of the pathological condition of the salivary glands).
Anatomy of the salivary glands [3]
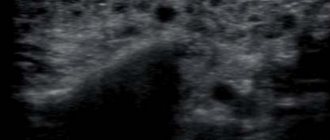
There are three pairs of major salivary glands (SG) and many small ones. The large ones include paired parotid, submandibular and sublingual SGs. The parotid salivary gland (PSG) is located on the outer surface of the branch of the lower jaw at the anterior edge of the sternocleidomastoid muscle, as well as in the retromandibular fossa. Dimensions vary widely: length 48-86 mm, width 42-74 mm, thickness 22-45 mm. The OSJ is covered by the parotid fascia, which is its capsule and is tightly fused with it. Sometimes, at the anterior edge of the parotid duct, there is an additional lobule measuring 10-20 mm, which has its own duct flowing into the parotid. The parotid duct emerges from the gland at the border of its upper and middle thirds, then it passes along the outer surface of the masticatory muscle parallel to the zygomatic arch and turns 90° inward, penetrating the fatty tissue and buccal muscle. The projection of the parotid duct onto the skin of the cheek is determined on the line connecting the tragus of the auricle and the corner of the mouth. The parotid duct opens in the vestibule of the oral cavity at the level of 1-2 large molars. The diameter of the duct is on average 1.5-3.0 mm, its length is 15-40 mm. The thickness of the gland contains the branches of the external carotid artery, the facial nerve and its branches, and the auriculotemporal nerve. There are many lymph nodes around the OUSG and in its parenchyma (Fig. 1), which can serve as a primary or secondary collector for draining lymph from teeth and oral tissues.
Rice. 1.
Lymph nodes in the thickness of the parotid salivary gland.
The submandibular salivary gland (MSG) is located in the submandibular triangle between the body of the mandible and the anterior and posterior bellies of the digastric muscle. The dimensions of the gland are: anteroposterior 20-40 mm, lateral 8-23 mm, superior-inferior 13-37 mm. Posteriorly, the PNJ is separated from the OSJ by a process of the fascia propria of the neck. The medial surface of the gland in the anterior section lies on the mylohyoid muscle. The submandibular duct, bending over the posterior edge of this muscle, is located on the lateral surface of the hyoglossus muscle. Then it goes between the medial surface of the hyoid gland and the genioglossus muscle to the point of its exit in the area of the hyoid papilla. The facial artery and its branches, the lingual artery and the veins of the same name pass through the gland.
The sublingual salivary gland (SSG) is located on the floor of the mouth in the sublingual region parallel to the body of the lower jaw. The dimensions of the gland are: longitudinal 15-30 mm, transverse 4-10 mm and vertical 8-12 mm. The duct of the parathyroid gland passes along its inner surface and opens in the region of the anterior section of the sublingual ridge independently or together with the submandibular duct. Sometimes the PJS duct flows into the middle section of the PJS duct.
The minor salivary glands - labial, buccal, lingual, palatine, incisive - are located in the corresponding areas of the mucous membrane. They can be a source of development of adenocarcinomas of the oral cavity.
Pathology of the salivary glands
SG malformations are rare. The most common are anomalies in the size of the glands (agenesis and aplasia, congenital hyperplasia (Fig. 2) and hypoplasia), their location (heterotopia, accessory glands), and anomalies of the excretory ducts (atresia, stenosis, ectasia, cystic transformation, ductal dystopia).
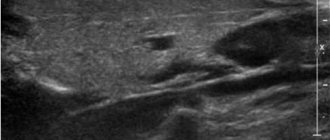
Rice. 2.
Hyperplasia of the left sublingual salivary gland.
Sialadenitis is a large group of polyetiological inflammatory diseases of the gastrointestinal tract (Fig. 3). Primary sialadenitis - sialadenitis considered as an independent disease (for example, mumps). Secondary sialadenitis is sialadenitis that is a complication or manifestation of other diseases (for example, sialadenitis with influenza). The echographic picture for different etiologies is not very specific. Etiology has clinical significance in determining treatment tactics.
Rice. 3.
Sialadenitis of the right submandibular salivary gland.
According to the etiological factor, sialadenitis is classified [4] into:
- sialadenitis developing under the influence of physical factors (traumatic sialadenitis, radiation sialadenitis (Fig. 4) occurs during radiation therapy of malignant tumors of the head and neck);
- sialadenitis developing under the influence of chemical factors (toxic sialadenitis);
- infectious sialadenitis (routes of infection penetration into the fluid: stomatogenic (through ducts), contact, hematogenous and lymphogenous);
- allergic and autoimmune sialadenitis (recurrent allergic, Sjogren's disease and syndrome, etc.);
- myoepithelial sialadenitis caused by a pathological process, previously designated as a benign lymphoepithelial lesion. The term benign lymphoepithelial lesion was first used by JT Godwin in 1952, replacing the concept of Mikulicz disease;
- obstructive sialadenitis, which develops when there is difficulty in the outflow of saliva due to obstruction of the excretory duct with a stone (Fig. 5-7) or thickened secretion, as well as due to cicatricial stenosis of the duct. According to the prevalence of the process, they distinguish between focal, diffuse sialadenitis and sialodochitis - inflammation of the excretory duct. The course of the process can be acute or chronic;
- pneumosialadenitis, which develops when there is air in the gastric tissue in the absence of a bacterial gas-forming infection. Air enters the gland from the oral cavity when the pressure there increases through the duct. Pneumosialadenitis is typical for a number of professions, primarily for glassblowers and musicians playing wind instruments.
Rice. 4.
Post-radiation sialadenitis.
Rice. 5.
Stone of the duct of the submandibular salivary gland.
Rice. 6.
Stone in the parenchyma of the submandibular salivary gland.
Rice. 7.
Stone in the duct of the submandibular salivary gland.
Tumors of the salivary glands
Tumors of the salivary glands are divided into two groups: epithelial and non-epithelial. Epithelial tumors predominate in adults (95%). In children with SG, epithelial and non-epithelial tumors are equally common. In addition to true tumors, processes resembling tumors (tumor-like lesions) develop in the GS.
Among epithelial tumors of the gastrointestinal tract, benign neoplasms are distinguished, as well as malignant ones - carcinomas.
Benign epithelial neoplasms of the stomach include ductal papillomas, adenomas and benign sialoblastoma. SG adenomas are divided into two groups: polymorphic (the most common SG adenoma) and monomorphic (all other) adenomas. Tumors of different structure, origin and prognosis were artificially included in the group of monomorphic adenomas.
Pleomorphic (polymorphic) adenoma (mixed tumor of the gland) is a adenoma of the gland, built from two types of cells: ductal epithelium and myoepithelial cells. Macromorphological picture. The tumor is usually an elastic or firm nodule of lobulated grayish-white tissue, usually partially encapsulated. Typical of a pleomorphic adenoma is the so-called chondroid stroma, resembling hyaline cartilage. Variants of the echographic image of pleomorphic adenomas are presented in Figure 8.
Rice. 8.
Pleomorphic adenoma of the gastrointestinal tract.
Warthin's tumor is an adenolymphoma in which multiple cystic cavities are formed, covered with double-layered epithelium. The papillae protrude into the lumen of the cysts. A pronounced proliferation of lymphoid tissue occurs in the tumor stroma. This tumor almost exclusively develops in the parotid gland.
Other types of benign tumors are less common. These are benign oncocytoma (oxyphilic adenoma), basal cell adenoma, tubular adenoma, benign cystadenoma sialoblastoma.
Among benign primary non-epithelial tumors, the most common are hemangioma, lymphangioma, neurofibroma and lipoma.
Among malignant non-epithelial tumors, malignant lymphomas are more often found (they arise, as a rule, against the background of myoepithelial sialadenitis, Sjögren's disease and syndrome).
Tumor-like lesions of the salivary glands
Rice. 9.
Salivary gland cysts.
- Salivary gland cysts (mucoceles). There are two types of mucocele of the gland: the retention type (retention cyst of the small gland, formed when saliva is retained in the excretory duct) and the type of interstitial secretion, when, when the wall of the duct is injured, saliva enters directly into the fibrous tissue surrounding the gland. Mucoceles in the floor of the mouth are also called ranulae.
- Cysts of the excretory ducts of large SGs are pronounced dilatation of the excretory duct due to retention of secretions in it. Blockage of salivary outflow can be caused by various reasons: tumor, stone, thickened mucus, post-inflammatory stenosis, even cicatricial obliteration of the lumen.
- Sialoadenosis (sialosis) is a non-tumor and non-inflammatory symmetrical increase in SF due to hyperplasia and hypertrophy of secretory cells. The outcome of sialosis is often SG lipomatosis. The process has a chronic relapsing course. Sialosis occurs in a number of diseases and conditions: diabetes mellitus, hypothyroidism, malnutrition, alcoholism, liver cirrhosis, hormonal disorders (hypoestrogenemia), reactions to medications (most often antihypertensive), neurological disorders.
Adenomatoid hyperplasia of small SGs leads to their increase to 0.5-3.0 cm in diameter. The causes of adenomatoid hyperplasia are trauma and prolonged exposure to ionizing radiation.
Oncocytosis is age-related changes in secretory cells and epithelium of the ducts of the gastrointestinal tract. In this case, the SF may slightly increase, but usually their value does not change.
To summarize, I would like to note that ultrasound using Doppler sonography in many of our observations helped to accurately determine the nature of the pathological process in the gastrointestinal tract. However, this diagnostic method does not allow one to unambiguously confirm or refute the malignant nature of the formation of the salivary glands.
Literature
- Benign and malignant tumors of soft tissues and bones of the face. A.G. Shargorodsky, N.F. Rutsky. M.: GOU VUNMTs, 1999.
- Topographic anatomy and operative surgery. I.I. Kagan, S.V. Chemezov. M.: GEOTAR-Media, 2011.
- Salivary glands. Diseases and injuries. V.V. Afanasiev. M.: GEOTAR-Media, 2012.
- Inflammatory diseases of the tissues of the maxillofacial area and neck. A.G. Shargorodsky. M.: GOU VUNMTs, 2001.
Ultrasound scanner HS70
Accurate and confident diagnosis.
Multifunctional ultrasound system for conducting studies with expert diagnostic accuracy.
It is very difficult to diagnose this disease in the early stages.
In most cases, patients notice that something is wrong when the stone prevents the complete drainage of fluid. All this is accompanied by sharp pain, similar to salivary colic. At the site of inflammation, the tissues swell and become swollen. These symptoms are not constant, the pain either increases or disappears. During treatment, the stone is removed; if the situation is too advanced, sometimes the entire gland is removed.
The salivary glands under the tongue extremely rarely. But at the same time, the disease develops at a rapid pace and can have adverse consequences.
In order to maintain your health, first of all, you must adhere to the rules of hygiene and if you experience the slightest discomfort, immediately consult a doctor.
Inflammation of the salivary gland under the tongue
What you can do at home
Treatment of inflammation of the salivary glands at home is acceptable, but only at the very initial stages of the disease or in combination with traditional methods of therapy. To avoid complications, you must consult a doctor .
To speed up recovery, you can drink and rinse your mouth with decoctions based on the following herbs:
chamomile; mint; raspberries; needles; eucalyptus; feverweed; sage; elder.
An excellent folk remedy for reducing pain and inflammation is aromatherapy with essential oils of fir, pine needles, eucalyptus and many other oils.
Pleomorphic adenoma of the minor salivary glands in the palate
Pleomorphic adenoma (PA) is the most common mixed benign tumor of the salivary glands. It is especially common in women in middle age. Approximately 80% of all cases involve the parotid gland, and about 7% involve the minor salivary glands. Histologically, this tumor is represented by both epithelial and mesenchymal elements, and is usually encapsulated in large salivary glands.
Mostly, tumors of the minor salivary glands are malignant (almost 50%). It has been established that the smaller the salivary gland, the greater the likelihood of tumor malignancy. The error of histological diagnosis varies from 1 to 14%. The difficulty of diagnosis lies not only in differentiating a benign neoplasm from a malignant one, but also in further, more detailed classification of the tumor.
The palate is the most common location of the minor salivary glands, followed by the lips and cheeks. PA appears as a painless firm formation and, in most cases, does not cause ulceration of the mucous membrane.
Ultrasound, CT and MRI may be used depending on the location and size of the tumor. The optimal treatment for PA is wide surgical excision of the formation along with the affected edges.
This clinical case examines a pleomorphic adenoma at the junction of the hard and soft palate.
Description of a clinical case
A 43-year-old woman was admitted to the clinic with complaints of a painless mass to the right of the junction of the soft and hard palate (Photo 1).
There was no somatic pathology in the medical history; the patient did not undergo drug treatment. Intraoral examination revealed a firm, approximately 2 x 2 cm, well-circumscribed, oval-shaped swelling to the right of the junction of the soft and hard palate (Figure 1).
Photo 1: Formation on the hard palate.
Also, palpation of the formation identified a tumor of soft consistency with well-defined boundaries.
Photo 2: Orthopantomogram
The orthopantomogram revealed changes in the bone structures and hard palate (Photo 2). MRI showed a well-defined mass on the palate (Figure 3). An incisional biopsy was prescribed. Histological examination revealed a keratinizing structure and myxoid degeneration (Figure 4). The cells were clustered into islands and layers separated from the myxoid matrix (Figure 4). Based on the data obtained, the final diagnosis was made: pleomorphic adenoma of the minor salivary glands of the soft and hard palate. The tumor was completely excised under local anesthesia, and the diagnosis was confirmed by repeat biopsy (Figure 5).
The postoperative period passed without complications and relapse.
Photo 3: MRI. Axial view showing a clearly visible mass.
Photo 4: Histological examination revealing keratinizing structure and myxoid degeneration, x40
Photo 5: Complete tumor removal
Photo 6: 3 weeks after surgery.
Discussion
PA occurs most frequently in the parotid salivary glands (56.7%), followed by the submandibular salivary glands (31.1%), palatine minor salivary glands (8.9%), and buccal minor salivary glands (3.3%).
A large number of tumors of the minor salivary glands are malignant (almost 50%). It has been established that the smaller the salivary gland, the greater the likelihood of malignancy of the tumor. Thus, differential diagnosis is vital.
Among all tumors of the salivary glands, malignant neoplasms such as mucoepidermoid carcinoma, adenoid cystic carcinoma and polymorphic poorly differentiated adenocarcinoma are distinguished. Mucoepidermoid carcinoma is the most common of all malignant tumors of the salivary glands.
The most vulnerable area after the parotid salivary gland is followed by the glands of the hard palate. Typically, such tumors are asymptomatic, grow slowly, have a different consistency, a bluish or red tint, and clinically resemble a mucous cyst. Adenoid cystic carcinoma most often occurs on the palate. It appears as a painful, slowly growing mass that affects surrounding structures and occurs in middle-aged people. Polymorphic poorly differentiated adenocarcinoma is also more often localized on the palate and usually presents as a slowly growing swelling. In the population, this disease predominates in older women.
Ultrasound, MRI and CT are used in diagnosis. In our case, MRI and CT were used. The CT scan was unremarkable, while the MRI revealed a mass on the palate.
Clinically and histopathologically, this formation can be mistaken for malignant; however, PA is a benign tumor that recurs quite rarely. The literature contains data on 2-44% of relapses. Wide surgical excision is the most preferred therapy. The occurrence of relapse may be associated with inadequate surgical treatment and removal of the tumor. In this clinical case, the tumor was completely enucleated.
Conclusion
The purpose of this report was to describe the diagnosis and treatment of a pleomorphic adenoma that was found at the junction of the soft and hard palate in a 43-year-old woman. The tumor was completely excised along with the affected edges. Recovery was uneventful with a short recovery period (Photo 6).
Authors: Firdevs AKPEK, Mustafa TEK, Orcun TOPTAS, Fat ih OZAN