Who is the study for?
The main indication for ultrasound examination of the salivary glands is the presence of any complaints in the patient. Most often, patients come to the doctor with the following problems:
- sharp pain in the submandibular or parotid area;
- local or general hyperthermia (increased temperature directly in the area of the lesion or in the entire body as a whole);
- increase in the size of the salivary glands;
- dry mouth (xerostomia);
- the presence of compactions (tumors, stones) near the salivary glands.
If the above symptoms are present, as well as after a visual examination, palpation examination and history taking, the doctor, in addition to laboratory tests, refers the patient to an ultrasound scan. The method is used if it is necessary to carry out differential diagnosis for such pathologies as:
- inflammatory diseases of the salivary glands (acute and chronic sialoadenitis, viral and bacterial);
- adenoma;
- salivary stone disease;
- tonsil damage;
- tumor neoplasms (malignant and benign);
- individual anatomical anomalies;
- enlargement of nearby lymph nodes;
- dystrophic lesions of organ tissue.
During the study, specialists can assess the condition of the group of large salivary glands: parotid, sublingual, submandibular.
Sialadenitis - symptoms and treatment
Diagnostic measures for diseases of the salivary glands can be divided into clinical, laboratory and instrumental.
Clinical methods include the collection of complaints, anamnesis (medical history), as well as direct examination of the patient.
During the questioning, the patient’s complaints are clarified, the time of their occurrence, the nature, intensity of pain, the impact of these symptoms on the quality of life, the presence of relapses and remissions, and their duration are specified. Separately, it is worth dwelling on questions about the presence or absence of somatic and infectious diseases - sometimes they can be a cause or an aggravating factor in the course of sialadenitis. It is worth clarifying whether parents and relatives had similar conditions.
During the clinical examination, the doctor pays attention to the presence of swelling and asymmetry of the face, the size, consistency, shape and relief of the affected and healthy salivary gland. These data largely depend on the primary nature of the disease, the presence of relapses and the nature of the treatment performed or its absence. The more relapses there were, the more sclerotic the gland was, which negatively affected its functioning. In the oral cavity, you should pay attention to the mouth of the excretory duct, and also examine the excretory duct itself (if possible) for the presence of salivary gland stones and other pathological changes. It is important to determine whether there is salivation. To do this, massage the gland tissue, after which the amount of saliva, its color and consistency are assessed.
Laboratory methods are required if sialadenitis is suspected. Blood, urine and saliva itself are examined. A general blood test can detect leukocytosis (increased levels of white blood cells) - the primary sign of inflammation. In blood biochemistry, special attention should be paid to blood glucose levels, and in urine - to the amount of salts. In saliva you can find a large number of leukocytes, impurities and pus, possibly the presence of bacteria and sand. Physicochemical parameters of saliva are given special attention [8].
One of the first hardware diagnostic methods for diseases of the salivary glands includes an x-ray of the gland - sialography . It allows you to determine the presence of stones in the thickness and excretory duct of the gland. sialography with contrast appeared , with the help of which it is possible to detect not only stones, but also to identify a narrowing of the lumen of the excretory duct, the presence of cysts and other neoplasms that impede the normal functioning of the gland.
The most modern sialogram method is digital dynamic sialography , through which it is possible to eliminate the overlap of the bone components of the jaws, visualize the soft tissue component of the gland and evaluate the flow of saliva through the duct. Among other things, it significantly reduces the radiation dose to the patient.
Computer and magnetic resonance sialotomography of small foreign bodies (stones) in the excretory duct and the gland itself.
The sialosonography method gives a fairly complete picture of the structure of the gland. With its help, you can easily identify sclerotic changes in tissues, foreign bodies, estimate their number, density, size, and also exclude the presence of neoplasms.
Thermosialography makes it possible to study the dynamics of changes in the temperature of the gland. This allows you to evaluate the effectiveness of the treatment.
Ultrasound-guided salivary gland biopsy is a fairly common diagnostic method. It is especially effective in the presence of cavities (cysts) in the thickness of the glandular tissue [9].
Currently, both throughout the world and in Russia, the most minimally invasive and informative method for diagnosing lesions of the salivary glands is widespread - sialoendoscopy . Modern devices help to visualize not only the excretory and intraglandular ducts, but also the ductal system, up to ducts of 2-3 orders, sometimes it is even possible to examine ducts of 4-5 orders.
The presence of a second working channel in the endoscope body allows not only visualization, but also washing, expansion of the duct, and, if necessary, collection of biopsy material. Using an endoscope, you can evaluate the color of the walls of the excretory duct, their elasticity, and detect the reasons that impede the normal flow of saliva through the ducts - stones, mucus plugs, polyps, neoplasms, areas of narrowing of the lumen of the duct. Also, thanks to endoscopic support during surgery, you can not only get a complete picture of the problem, but also eliminate it with minimal intervention.
How to prepare for the procedure
Ultrasound of the salivary glands is an absolutely safe and painless manipulation, for which the patient does not require special preparation. Patients of almost any age tolerate the procedure well, without showing any anxiety before and during its implementation, and therefore it does not require premedication (pre-administration of sedative medications) even in children.
On the eve of the visit to the specialist (about 3-4 hours in advance), the patient is advised to refrain from eating, and immediately before the examination he needs to thoroughly clean the oral cavity.
Detailed description of the study
Salivary gland cancer is a malignant tumor of the salivary gland formed from epithelial cells. Tumors of the parotid salivary glands (PST) are a rare type of neoplasm. They mainly develop between the ages of 20 and 40. More common in men than in women. Tumors are usually located in the soft tissues of the face and often cause serious cosmetic defects, causing paresis of the facial nerve.
The main risk factors for developing salivary gland cancer are:
- Chronic inflammatory diseases of the oral cavity;
- Hormonal imbalances;
- Genetic disorders;
- Smoking;
- Nutritional factors (low vitamin content, high fat content in food).
Most often the tissues of the parotid salivary gland are affected - 80%, less often the tumor develops in the tissues of the submandibular salivary gland - 15%, sublingual or minor salivary gland.
The following options for the development of pathology are distinguished:
- Primary cancer (from the tissues of the gland itself);
- Secondary cancer (metastasis or germination from neighboring organs).
According to histological parameters, tumors of the salivary glands represent the most heterogeneous group of human neoplasms. More than half of them are benign formations.
Benign neoplasms of the parotid salivary glands are detected in more than 30% of patients who complain, malignant ones - in 65%. Among the morphological types of benign tumors of the parotid salivary gland, the most commonly diagnosed are pleomorphic adenoma (a benign formation that forms in the glandular epithelium), adenolymphoma, lipoma and a very rare adenoid cystic tumor (formed by epithelial cells lining the lumen of the gland).
Malignant tumor formations are most often represented by: mucoepidermoid cancer (formed by cells secreting mucus and epithelium) and adenocarcinoma. Acinic cell carcinoma also occurs, which mainly affects the tissue of the parotid salivary gland.
Usually, during examination of patients, palpation reveals a dense, painless formation in the area of the salivary glands, which, according to patients, grows generally very slowly. In approximately a third of cases, pain may be present.
The “gold standard” for diagnosing tumors of the salivary glands is aspiration puncture of the tumor followed by histological examination of the obtained material, carried out before surgery or intraoperatively. The diagnostic value of this method is up to 90%, because the tissue of the affected area is studied directly under a microscope.
Aspiration puncture (biopsy) is performed using a special needle under ultrasound control. The study allows you to confirm or clarify the diagnosis, track the growth dynamics of the tumor and analyze the changes that occurred during tumor therapy.
During histological examination, three indicators are assessed:
- Tumor size and extent of its spread (T);
- The presence of damage to regional lymph nodes by metastases (N);
- Determination of metastases in other organs and tissues (M).
Based on the degree of malignancy, there are three types of tumors:
- High differentiation, when the cells are similar to glandular epithelial cells, such formations grow slowly and often have a favorable prognosis;
- Low differentiation, when cells are very different from normal, is characterized by rapid growth and early metastases;
- Medium differentiation.
How to do an ultrasound of the salivary gland
The examination can be carried out in 2 ways: from the oral cavity and from the external surface. The procedure does not take much time (it usually takes no more than 20-30 minutes to complete). During an ultrasound scan of the salivary glands, the patient does not feel any pain or other discomfort.
During the examination, the patient takes a supine position, places his head on a specially prepared pillow and tilts it slightly back (or turns it to the left or right, depending on the location of the gland being examined).
If the parotid gland is being examined, the device's sensors are placed on the parotid area. When studying the sublingual and submandibular glands - into the oral cavity (sometimes the extraoral method can be used).
Parotid gland
Parotid gland
(lat.
glandula parotidea
) - paired salivary gland. Along with the submandibular and sublingual glands, the parotid glands belong to the so-called major salivary glands. The parotid glands are the largest of all the salivary glands. The mass of the parotid gland is approximately 20–30 g. The parotid glands are grayish-pink in color and irregular in shape. The parotid glands are located on the lateral surface of the lower jaw and the posterior edge of the masticatory muscle, under the skin, in front and below the auricle. From above, the parotid gland approaches the zygomatic arch, from below - to the angle of the lower jaw, from behind - to the anterior edge of the sternocleidomastoid muscle and the mastoid processes of the temporal bone. Behind the lower jaw, the parotid gland reaches the stylopharyngeal, stylohyoid and styloglossus muscles, starting from the styloid process. Secretes mixed saliva.
The excretory duct of the parotid gland (stenon duct) opens on the side wall of the vestibule of the oral cavity at the level of the second upper molar.
The parotid gland is surrounded by the parotid-masseteric fascia. The density of this fascia is uneven: mostly dense, it has loosened areas covering the upper and medial surfaces of the gland.
Sometimes there is an accessory parotid gland above the Stenon duct, the excretory duct of which merges with the Stenon duct.
On the GastroScan.ru website in the “Literature” section there is a subsection “Oral diseases associated with gastrointestinal diseases”, containing publications for healthcare professionals on this topic.
Parotid gland The Nomenclature of Medical Nomenclature of Medical Services approved by Order of the Ministry of Health of Russia dated October 13, 2022 N 804n provides for the following services:
- Removal of formations of the parotid salivary gland with isolation and preservation of the branches of the facial nerve, service code A16.07.064
- Removal of the salivary gland, service code A16.07.067
- Removal of the parotid salivary gland with isolation and preservation of the branches of the facial nerve, service code A16.07.067.005
- Subtotal resection of the parotid salivary gland, service code A16.07.067.006
- Resection of the parotid salivary gland, service code A16.07.080
- Resection of the parotid salivary gland with a reconstructive plastic component, service code A16.07.080.001
- Resection of the parotid salivary gland with neurolysis of the trunk and/or branches of the facial nerve using microsurgical technology, service code A16.07.080.002
Figure used under CCA3.0 license, taken from “Medical gallery of Blausen Medical 2014”. WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436. Adapted. Back to section
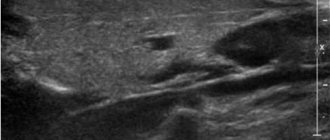
Ultrasound of the submandibular salivary gland
The norm for an ultrasound examination of the salivary submandibular gland corresponds to the following parameters:
- Fine-grained homogeneous structure.
- The edges of the glands are smooth.
- The excretory duct is well visualized, small in size, without signs of blockage.
Determining the normal size of the submandibular glands is not particularly difficult precisely because of its clear contours. During inflammation (sialoadenitis), the organ increases in size and its edges become blurred.
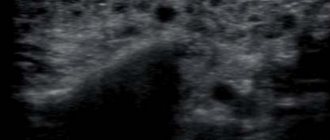
Ultrasound of the sublingual salivary gland
Normally, the sublingual salivary gland has smooth, not very clear contours. They have a homogeneous structure, but echogenicity (the ability to reflect ultrasound) may be slightly increased. In the absence of any diseases, the device will not show the ducts of this organ.
The shape of the sublingual salivary glands displayed on the device screen changes depending on where the sensor is placed. When located in the chin area, the glands have oval contours. If the device is applied parallel to the body of the lower jaw, the glands will be slightly elongated.
Parotid gland
, the largest of all salivary glands, is a complex alveolar gland of the serous type (see diagram on this page and figure in a separate window).
Its mass is ~20 ÷ 30 g
.
It has an irregular shape and is located under the skin anterior and inferior to the auricle, on the lateral surface of the ramus of the mandible and the posterior edge of the masticatory muscle. The fascia of this muscle is fused with the capsule of the parotid salivary gland. At the top, the gland almost reaches the zygomatic arch, at the bottom - to the angle of the lower jaw, and at the back - to the mastoid process of the temporal bone and the anterior edge of the sternocleidomastoid muscle. In the depths of the maxillary fossa, behind the lower jaw, the parotid gland, with its deep part, is adjacent to the styloid process and to the muscles starting from it: stylohyoid, styloglossus, stylopharyngeal. The external carotid artery, mandibular vein, facial and auriculotemporal nerves pass through the gland. Deep parotid lymph nodes are located in the thickness of the gland. The parotid gland has a soft consistency and well-defined lobulation. On the outside it is covered with a connecting capsule. Bundles of capsule fibers pass inside the gland and separate its lobules from each other. At the anterior edge of the gland, the parotid duct emerges from it. It is called the Stensen duct after its discoverer, Niels Stensen, Danish anatomist, naturalist and theologian, 1638-1686. The parotid duct goes forward 1 ÷ 2 cm
below the zygomatic arch along the outer surface of the masticatory muscle, then, going around the anterior edge of this muscle, pierces the buccal muscle and opens in the vestibule of the mouth at the level of the second upper molar. On the surface of the masseter muscle
An accessory parotid gland is often located next to the parotid duct. Arterial blood enters the gland through the branches of the superficial temporal artery. Venous blood flows into the mandibular vein. The lymphatic vessels of the gland drain into the superficial and deep parotid lymph nodes. Afferent innervation of the gland is carried out by fibers of the auriculotemporal nerve. Efferent innervation is provided by parasympathetic and sympathetic fibers. Parasympathetic postganglionic fibers pass as part of the auriculotemporal nerve from the auricular ganglion. Sympathetic fibers pass to the gland from the plexus around the external carotid artery and its branches. Submandibular gland
(see diagram on this page and figure in a separate window) is a complex alveolar-tubular gland that secretes and secretes a mixed secretion.
It is covered with a thin capsule and is located in the submandibular triangle. Outside the gland is adjacent to the superficial plate of the cervical fascia and skin. The medial surface of the gland is adjacent to the hyoglossus and styloglossus muscles. The upper edge of the gland is in contact with the inner surface of the body of the lower jaw, and the lower part comes out from under its lower edge. The anterior part of the gland in the form of a small process lies on the posterior edge of the mylohyoid muscle. Here its submandibular duct emerges from the gland. It is called Wharton's duct after its discoverer, Thomas Wharton, 1614-1673, British anatomist. The duct is directed forward, adjacent on the medial side to the sublingual salivary gland and opens with a small opening on the sublingual papilla, next to the frenulum of the tongue. On the lateral side, the facial artery and vein are adjacent to the gland (before they bend through the lower edge of the lower jaw), as well as the submandibular lymph nodes. The arterial branches of the facial artery approach the submandibular gland, and the venous branches go into the vein of the same name. Lymphatic vessels originate from the adjacent submandibular lymph nodes. Afferent innervation of the gland is carried out by fibers of the lingual nerve (from the mandibular nerve - the third branch of the trigeminal nerve, V pair of cranial nerves). Efferent innervation is provided by parasympathetic and sympathetic fibers. Parasympathetic postganglionic fibers pass as part of the facial nerve (VII pair of cranial nerves) through the chorda tympani and the submandibular ganglion. Sympathetic fibers pass to the gland from the plexus around the external carotid artery. The sublingual gland
(see diagram on this page and figure in a separate window) secretes a mucous-type secretion. It is small in size and located on the upper surface of the mylohyoid muscle, directly under the mucous membrane of the floor of the mouth, which forms the sublingual fold here. The lateral side of the gland is in contact with the inner surface of the lower jaw in the area of the sublingual fossa. The medial side of the gland is adjacent to the geniohyoid, hyoglossus and genioglossus muscles. The large sublingual duct opens together with the excretory duct of the submandibular gland (or independently) on the sublingual papilla. It is called Bartholin's duct after its discoverer, Thomas Bartholin, 1616-1680, Danish naturalist, physiologist and anatomist. In addition, several small sublingual ducts independently flow into the oral cavity. After the name of the discoverer, they are called Rivinus (Bachmann) ducts, August Quirinus Bachmann (Rivinus), 1652-1723, German anatomist and botanist. These ducts are located on the surface of the mucous membrane along the sublingual fold (see figure). The branches of the hypoglossal artery (from the lingual artery) and the mental artery (from the facial artery) approach the gland. Branches of the veins of the same name extend from the gland. Lymphatic vessels depart from the sublingual gland. They begin in the submandibular and mental lymph nodes. Afferent innervation of the gland is carried out by fibers of the lingual nerve. Efferent innervation is provided by parasympathetic and sympathetic fibers. Parasympathetic postganglionic fibers pass as part of the facial nerve (VII pair) through the chorda tympani and the submandibular ganglion. Sympathetic fibers pass to the gland from the plexus around the external carotid artery.
Literature. Illustrations. References. Illustrations
Click here to access the site's library! Click here and receive access to the reference library!
- Garrett JR, Ed. Neural Mechanisms Of Salivary Gland Secretion = Mechanisms of neural regulation of salivary gland secretion. Karger, 1999, 236 p. Tutorial
. Access to this source = Access to the reference. URL: https://www.tryfonov.ru/tryfonov/serv_r.htm#0 quotation
See: Gastroenterology: dictionary, Gastroenterology: Literature. Illustrations,
| LIBRARY = LIBRARY Human Physiology = Human Physiology, Human Anatomy = Human Anatomy, Human Biochemistry = Human Biochemistry, Human Psychology = Human Psychology, Medicine = Medicine, Mathematics = Mathematics, Chemistry = Chemistry, Physics = Physics, General Scientific Literature = General Science Lexis. Click here to access any source in the site's library! Click here and receive access to the any reference of the library! “I AM LEARNED. . . N E D O U C H A ?” T E S T V A S H E G O I N T E L L E C T A Premise : The effectiveness of the development of any branch of knowledge is determined by the degree of compliance with the methodology of knowledge - the knowable entity. |
Error? Click here and fix it! Search on the site E-mail of the author (author)