Removing a tooth is the last thing a dentist will suggest. Due to a number of subjective and objective reasons, it is impossible to maintain the dentition in ideal condition until old age.
Dental defects are the loss of one or more dental units, leading to a violation of the integrity of the dentition, deviation in the development of physiological occlusion, and an abnormal arrangement of individual teeth.
Reasons contributing to the development of dental defects
Dental defects arise due to:
- untimely treatment of caries;
- inflammatory processes in the oral cavity;
- presence of malocclusion;
- genetic conditioning;
- diseases leading to changes in metabolic processes;
- damage to the jaw apparatus;
- various neoplasms.
Classification of dentition defects
There are several types of classification. Dentists mainly use three of them:
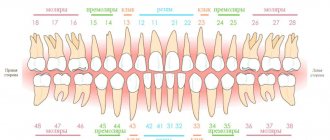
- Kennedy classification:
- Group 1 - bilateral absence of chewing teeth;
- Group 2 - unilateral absence of a molar;
- Group 3 - unilateral absence of lateral teeth with preservation of distal support;
- Group 4 - defect of the anterior jaw.
- Beltman classification:
- Class 1 - the defect includes edentulous chewing teeth.
a) dentition with unilateral terminal defects;
b) dentition with bilateral terminal defects.
- Class 2 - there is one or more included defects (if the terminal units are present, there may be no teeth in other parts of the row).
a) the number of missing units does not exceed three;
b) the number of missing units is three or more.
- Classification according to the Gavrilov system:
- Group 1 - dentition with terminal one- and two-sided defects;
- Group 2 - dentition with anterior and lateral one- and two-sided defects;
- Group 3 - combined defects;
- Group 4 - single preserved dental units.
Direct restoration of the coronal part of the tooth using composite material C-Fill MH
Traditionally, the main requirements set by the patient are to restore the shape of the future restoration and match the color. It is not always possible to carry out such tasks, especially when it comes to restoring the frontal group of teeth. Many patients try to correct the doctor’s actions, saying, “the tooth should look a little longer,” or “Doctor, let’s make this tooth lighter,” while forgetting about the physiological and anatomical possibilities in the oral cavity.
A particularly important point is to discuss all the intricacies of the future restoration immediately before the start of treatment. Using computer modeling, the doctor can show what the tooth will look like after restoration. You can also use wax modeling on models and explain why the tooth will have this particular shape. The patient must understand that restoration of anterior teeth
longer (this was his wish) may not be possible, since these teeth will block
moving the lower jaw forward. This must be demonstrated on diagnostic models made before treatment. After receiving such information, the patient already has an idea of what his teeth will look like at the end of treatment.
Direct restoration of the coronal part of a tooth is a rather complex manipulation. In contrast
from ceramic restorations, which, firstly, take place in several stages, and secondly, imply a large volume of interventions, composite restorations require minimal preparation, which is a very important factor, therefore direct restoration is considered the most popular technique among both dentists and among patients.
The main requirements for performing such work are:
– high professionalism of the doctor;
– the presence of a modern composite material with properties that allow the restoration to maintain color and shine for a long time, as well as sufficient strength and wear resistance.
During diagnostic modeling, the doctor determines the parameters and shapes of the crown part of the tooth. But when restoring a tooth, one of the main tasks is determining the color. If there are shadowless lamps in the office, this is much easier to do.
When choosing a color for the frontal group of teeth, it is important to take into account the thickness of the crown of the tooth, as well as the transparency of the enamel and the degree of destruction. Depending on these factors, the thickness of the material being laid will depend: opaque, dentin, enamel.
Using the example of several clinical cases in which teeth were restored with different
the degree of destruction of the coronal part, we will consider the implementation of restorations using the filling material C-Fill MH (Megadenta Dentalprodukte).
When choosing a material for restoring these teeth, we took into account such physical qualities as high strength, excellent polishability to full shine and a wide range of colors, with which we can achieve an excellent aesthetic effect.
Clinical case No. 1
The patient came to the clinic with complaints about the tooth’s reaction to thermal irritants and the appearance of a cavity.
As a result of the examination, a hard tissue defect of class V according to Black is determined in the cervical area of tooth 22.
All work in the oral cavity is carried out using a rubber dam isolation system. An additional butterfly clasp was installed to retract the gingival margin.
To accurately select the color, the tooth is cleaned with paste and a brush. Minimal invasive treatment is performed.
When using C-Fill MH material, a total etch technique is used.
This is followed by the application of the two-component ethanol-based bonding system C-Prime S Plus.
For better adaptation of the base material, the flowable material C-Fill Flow is used.
The C-Fill MH A3 composite is applied layer by layer.
As a result, after polishing this restoration, we observe an excellent aesthetic effect.
The presence of boundaries between the material and the enamel is almost impossible to determine.
Rice. 1. Cervical caries of 22 teeth, isolation with rubber dam, butterfly clasp installed.
Rice. 2. Formation of a cavity.
Rice. 3. Total etching with C-CID gel.
Rice. 4. Treatment of the cavity with a two-component bonding system C Prime S Plus using a brush.
Rice. 5. Application of liquid material C Fill Flow A3.
Rice. 6. Restoration of the cervical cavity with C-Fill MH material, color A3.
Rice. 7. Polishing with KENDA discs and rubber bands.
Rice. 8. Final view of the restoration.
Clinical case No. 2
Due to multiple defects in the filling material, it was decided to replace the old restoration.
During the treatment, work was carried out in the canal. After removing all necrotic hard tissues, we received a complete absence of the crown part of the tooth. An anchor was installed to support the structure.
The restoration was carried out in several stages.
Initially, a stump of opaque material was formed onto the anchor. Next, we form the main dentin layer.
The final stage is the application of C-Fill MH A2 enamel. The lack of pronounced transparency of the incisal edge on the adjacent teeth excluded the use of transparency.
Rice. 9. Change in color of the restoration of tooth 22.
Rice. 10. Insulation with rubber dam.
Rice. 11. Significant destruction of the crown part of the 22nd tooth.
Rice. 12. Creation of a stump on the anchor.
Rice. 13. Restoration of tooth 22 using C-Fill MH A2 material.
Rice. 14. Defects in filling material on teeth 12, 11, 21.
Rice. 15. Intermediate stage of treatment: prepared cavities.
Rice. 16. Final view of the restoration. The material used is C-Fill MH OA3, A2.
Clinical case No. 3
This clinical case reflects a powerful physical effect on the frontal group of teeth.
As a result of bruxism and the partial absence of chewing teeth, pathological abrasion of the anterior group of teeth appeared, as well as chips in the restoration and enamel.
Restoration was carried out using the technique of layer-by-layer application of C-Fill MH material. When grinding the restoration and introducing it into the bite, changes in the dentition of the lower jaw (teeth are dystopic) and the ratio of antagonists were taken into account.
Final polishing was done using KENDA rubber bands.
Conclusion
The use of modern composite materials and mastery of the latest techniques gives the modern doctor a great advantage - such a dentist can achieve optimal aesthetic results when performing restoration work on the frontal group of teeth, even in the most complex and non-obvious clinical situations.
With direct composite restorations, both small and medium-sized defects in the hard tissues of teeth can be replaced in the most natural way possible – without any compromise in terms of aesthetics and taking into account the wishes of the patients.
Symptoms and consequences of dental defects
Dental defects appear:
- chewing function disorder;
- incorrect bite;
- articulation disorder;
- single displacement of teeth;
- violation of the integrity of the dentition;
- violation of the aesthetics of a smile.
Diagnosis of dental defects
The removal of one or more dental units requires consultation with a dentist and an orthodontist, especially when it comes to the anterior part of the dentition. Untimely correction of the defect does not have the best effect on the condition of adjacent teeth.
As a rule, a visual inspection is sufficient to determine how to correct the defect. In some cases, x-rays may be needed.
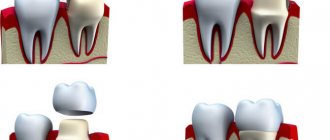
What happens if the crown is not restored in time?
Ignoring crown defects leads to worsening pathological changes, up to complete destruction of the upper part and damage to the root.
The loss of even one crown leads to the following consequences:
- disturbances in the chewing process;
- overload and wear of other sectors of the dentition;
- displacement of neighboring units;
- destabilization of antagonist teeth;
- diction disorders;
- expansion of defects;
- cosmetic defect (especially if the crowns in the smile area are damaged).
Timely restoration of the crown part is much simpler, cheaper and more physiological than replacing your own tooth with an artificial one.
Indications for tooth restoration
For most patients, the procedure is the optimal way to restore a lost tooth fragment. Indications for its implementation are:
- significant destruction of the crown while maintaining the root,
- gaps between teeth,
- cracks and chips on the surface,
- tooth fractures,
- changes in enamel associated with age,
- malocclusion,
- destruction of the crown due to caries,
- wear of enamel,
- darkening of teeth when whitening is not possible.
When choosing a restoration method, the doctor evaluates the degree of damage to the crown, the location of the tooth in the dentition, its shade and shape. The dentist also takes into account the nature of the patient’s bite, bad habits, allergic reactions and possible disorders in the structure of the jaw, joint deviations, psycho-emotional reasons, for example, bruxism.
IROPD - index of destruction of the occlusal surface of the tooth
It represents the ratio of the dimensions of the “cavity-filling” area to the chewing surface of the tooth.
The root cause of damage to the integrity of the tooth remains caries. During the pathological process, the hard tissues of the teeth are damaged, their shape is deformed, leading to disturbances in speech and chewing functions, and the appearance of external defects.
The effectiveness of actions restoring a damaged tooth is determined by a number of factors:
- the degree of damage to the coronal area, which is under the influence of the carious process;
- timely contact with a dentist;
- correct diagnosis, professionalism and experience of specialists, as well as characteristics of the components and technological methods involved. Before recreating the anatomical form and function of dental tissue, individual preparation is required for each individual case.
Determining the degree of destruction of the occlusal surface of the tooth is a determining factor when choosing a treatment method (filling, inlay and artificial crown) in order to prevent further destruction of crowns and tooth extraction. For quite a long time, dentists have been using the method proposed by V.Yu. to determine the area of tooth destruction. Milikevich index of destruction of the occlusal surface of the tooth.
To determine this index, the author used a standard transparent plate with a millimeter grid applied and a plaster model of the jaw. A transparent plate is applied to a plaster diagnostic model of the jaw, to the occlusal surface of the tooth with a defect, and the area of the occlusal surface and the defect is determined. Depending on this ratio, indications for replacing defects in the hard tissues of the tooth crown with various types of orthopedic structures are determined.
IROPS = Cavity/filling area / Masticatory surface area
With IROPI indicators of 0.2 – 0.4
The filling method is used. After endodontic treatment, a temporary filling (bandage) can be placed if it is not possible to place a permanent filling on the first visit or to prevent possible complications. Permanent filling is carried out in one visit.
With IROPV > 0.4
shows the manufacture of inlays from metals, ceramics or composite materials.
With IROPV > 0.6
production of artificial crowns is shown.
With IROPV > 0.8
the use of pin structures with subsequent production of crowns is shown.
Today there is a simpler and accessible way for every doctor to calculate the IRPI. We photograph the tooth from the occlusal surface using any camera (microscope, intraoral camera, camera or smartphone through a mirror) and transfer the image to the computer.
Dental restoration methods
Of the existing methods of dental restoration, there are five most common:
- Filling with photocomposite materials - to harden such fillings, infrared or ultraviolet light is needed. The material is very plastic, therefore it allows you to level out damage up to ⅓ of the tooth crown.
- Dental inlays are ceramic prostheses that help restore the anatomical shape of chewing teeth.
- Veneers are thin porcelain microprostheses that cover the front wall of the tooth, last 10–15 years, and restore the shape and size of only the front surfaces of the teeth.
- Pin - installation is possible only if the root is preserved. When the hard tissues of the tooth are completely destroyed, the doctor inserts a pin, covers it with photopolymer material, and then puts on a crown.
- Crowns are caps that completely imitate the surface of one or more teeth. They are made from different materials. A metal-ceramic crown is based on a metal alloy. The top of the cap is covered with a layer of ceramic. Metal-free dental crowns are a combination of durable ceramics and zirconium dioxide. The method is suitable for destruction of the tooth crown of more than of the surface and loss of at least 40% of dentin.
The position of the tooth plays an important role when choosing a restoration method. For frontally located teeth, photopolymers and veneers are used. Most often, pins or crowns are placed in chewing teeth.
The decision on the method of restoring the crown part of the tooth is made by the dentist after an individual consultation and additional examination.