The proportions of the face largely depend on the condition of the parotid salivary glands, which for various reasons can increase in size, swell and create not only aesthetic problems, but also health problems.
The parotid salivary glands, or rather their unhealthy condition, affect the proportions of the face. this creates aesthetic problems, and can also significantly affect the health of the entire body. The main problem of the parotid glands is the occurrence of a tumor. Outwardly, this is a small swelling, which cannot be immediately noticed, but when palpated, a small formation with clear boundaries appears. As a rule, this type of tumor does not bother the patient in any way, and not everyone notices it right away.
Most of these manifestations do not become a threat to humans, since the tumor is benign. However, there are also situations when the tumor literally becomes larger and larger in a matter of days. in this case, the status of the tumor changes to malignant and requires immediate contact with a specialist for removal of the formation.
Removal of parotid tumor
At the ART Clinic, under the guidance of Professor Nerobeev, operations of the parotid salivary gland are performed. This type of surgical intervention presents certain difficulties that should only be trusted to professionals. The gland contains branches of the facial nerve, which should not be touched under any circumstances. If this happens, then the person who came for help may be left with a distorted face for the rest of his life.
Unfortunately, not all doctors work honestly, and in some cases they ask you to sign a paper that describes the possible consequences in advance. This indicates the unprofessionalism of the surgeon who is not ready to take responsibility.
Treatment of a tumor of the parotid salivary gland at the ART Clinic means reliable staff, high-quality equipment and the best techniques. Before undergoing any surgery, you must schedule an initial consultation for examination. Remember that even if there is no discomfort or pain, a tumor of the parotid gland still requires examination.
Would you like more information about surgery in our clinic? We are ready to answer any questions by phone, as well as in the feedback form. You can find out the cost of the operation on our website or during your first visit.
It is known that congenital changes in the ductal system of the parotid salivary gland can be in the form of a cyst-like lesion of the parotid duct of the “megastenon” type, both outside and inside its parts (ectasia) in combination with individual areas of a sharp decrease in its diameter (stricture) - V.V. . Afanasiev (1993).
Remaining clinically invisible and undetectable for a long time, these changes can ultimately lead to the development of chronic sialodochitis of the parotid gland or the formation of salivary stones.
Exacerbations of chronic parotitis against the background of pronounced congenital changes in the parotid gland occur quite often, are difficult to respond to conservative therapy, and in some cases lead to the development of abscesses and phlegmons of the parotid-masticatory area, requiring repeated emergency surgical intervention in a specialized hospital.
Treatment of such patients should include a complex of special conservative therapy both during the rest period and during the period of exacerbation of the disease [1-4].
Despite the developed methods of conservative treatment, there comes a time when they do not bring adequate clinical results and the question of surgical treatment arises - removal of the salivary gland.
At the same time, many maxillofacial surgeons refuse to remove the parotid salivary gland for chronic sialadenitis due to a well-founded fear of damage to the branches of the facial nerve, which are immured in the inflamed tissue of the gland, and the subsequent onset of paralysis of the facial muscles.
In such cases, doctors limit themselves to palliative measures, dooming patients to an uncomfortable life in the future.
In such cases, some scientists proposed extinguishing the function of the parotid gland by ligating the parotid duct intraorally [5] with possible subsequent alcoholization of the auriculotemporal nerve [6]. The proposed methods, according to clinicians, often gave relapses and were unreliable.
The above prompted us to work on developing a technique for surgical correction of congenital deformities of the parotid ducts.
Material and methods
In total, under our supervision there were 14 patients aged from 24 to 74 years, in whom, on the basis of a comprehensive examination, we diagnosed congenital deformities of the parotid ducts with a pronounced expansion of the extra- and/or intraglandular part of the parotid duct of the “megastenon” type.
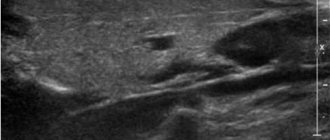
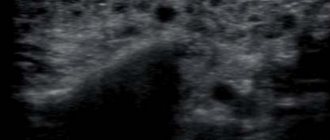
The comprehensive examination included general (complaints, anamnesis, examination, probing of the duct), specific (general radiography, sialography) and special research methods (computer sialotomography, multispiral computed sialotomography with sialography, digital dynamic sialography).
During the examination, attention was paid to the frequency of exacerbations of chronic parotitis, the severity of dilation of the ducts, the localization of ectasia and the presence of strictures.
All our patients were bothered by frequent exacerbations of chronic parotitis, in some cases leading to emergency hospitalization of the patient.
Thus, 4 patients, before contacting us, had undergone operations for phlegmon of the parotid-masticatory area, which arose as a result of repeated exacerbations of mumps. In one patient, such interventions were performed 8 times over 5 years.
In 3 (out of 14) patients, a calculus had previously been removed from the parotid duct using intraoral access, after which strictures of the duct were formed, which led to frequent exacerbations of chronic parotitis.
In 1 patient, a calculus was found in the anterior third of the parotid duct in combination with a pronounced expansion along its entire length and atypical ectasia of the accessory lobe in combination with strictures.
results
We performed reconstructive plastic surgery on the parotid duct in all patients, aimed at extinguishing the secretory function of the parotid salivary gland in order to exclude subsequent exacerbations of the process. This was caused by the presence of several strictures of very small diameter along the course of the duct and the impossibility of restoring its patency.
In all patients, surgery was performed via external access. At the same time, with a cut according to the method of G.P. Kovtunovich managed to limit himself in 9 cases, and in 5 patients, to ensure optimal access, it became necessary to make an additional incision using the A.V. method. Klementova.
Surgical interventions were performed as follows.
Under general anesthesia, a salivary probe was inserted into the parotid duct, if possible. After hydropreparation of the tissues of the parotid-masticatory area with 20 ml of a 0.5% solution of lidocaine hydrochloride and a solution of adrenaline hydrochloride 0.1% - 0.5 ml, an external skin incision was made. After folding the skin-fat flap, the parotid-masticatory fascia and the parenchyma of the gland above the duct were dissected. The parotid duct was isolated to the point of its entry into the peripharyngeal space and the ducts flowing into it. The duct was dissected along its entire length (Figure a, see color insert),
Figure 1. Suturing the dilated parotid duct.
a — the wall of the duct is dissected; b — suturing the duct wall with a duplication; c — the parotid duct is sutured along its entire length. after which the gland ducts were sanitized by washing with antiseptic solutions. In case of pronounced dilatation of the parotid duct, partial excision of its wall was performed. Next, the first order ducts flowing into the main duct were ligated. The parotid duct was ligated by screwing its walls inward in the form of a duplicator to avoid the appearance of a cavity inside it, where saliva secreted by the cells of the duct wall could be secreted (Figure, b, c, see color insert)
.
After this, careful suturing of the parenchyma and parotid-masticatory fascia was performed. The skin flap was placed in place and fixed with a continuous intradermal suture. The wound was drained for 24 hours.
In the postoperative period, a pressure bandage was applied to the parotid area, drug therapy and drugs aimed at reducing the secretory function of the gland were prescribed: 8 drops of atropine sulfate solution 0.1% 3 times a day 30 minutes before meals. The sutures were removed on the 8th day.
In 3 patients in the postoperative period, the occurrence of salivary fistulas along the surgical wound was noted, which were successfully closed conservatively within 2 weeks.
In 1 patient, paresis of the levator angle oris muscle was noted, which was completely relieved 2 weeks after the administration of B vitamins.
Follow-up examinations of patients were carried out up to 3 years. During the postoperative period, 1 patient noted a one-time swelling of the gland during meals, which quickly passed and did not recur. The remaining patients had no complaints, there were no exacerbations of mumps. The postoperative scar was barely noticeable. No saliva was released from the parotid duct.
conclusions
In the presence of pronounced changes in the ducts of the parotid gland such as ectasia or stricture, an alternative treatment method is reconstructive plastic surgery. If it is impossible to perform operations aimed at preserving the function of the parotid gland, surgical interventions aimed at extinguishing its secretory function with excision of the walls of the duct are indicated.
We consider the indication for such interventions to be the presence of severe ectasia and strictures of the parotid duct and a history of frequent exacerbation of chronic parotitis and requiring external incisions due to the development of phlegmon, as well as the patient’s desire to live in comfortable conditions.
Advantages of parotid salivary gland treatment at ART-Clinic
Online consultations for patients from the regions
A team of highly qualified specialists with extensive experience
Modern minimally invasive techniques of operations and reconstructions
Affordable prices, promotions, discounts, installments
Operations for the treatment of the parotid salivary gland at the ART Clinic are performed by a team of highly qualified plastic surgeons, headed by Doctor of Medical Sciences, Professor A.I. Nerobeev, who is one of the most famous maxillofacial surgeons in Russia. He specializes in reconstructive surgery.
At ART-Clinic they perform operations even in very complex cases. Success in this case is determined by both the expert class of surgeons and advanced equipment: during the operation in our clinic, a modern neurodetector is used, which sends weak current pulses and, by the reaction of the facial muscles, allows one to judge where the nerve passes, giving the doctor a hint.
Make an appointment with Professor Nerobeev by phone and 8 800 500 42 32 (calls within Russia are free) or using a special form.
Indications
Indications for removal of the submandibular salivary gland are:
- chronic sialadenitis (inflammation);
- benign or malignant tumors;
- multiple cystosis;
- salivary stone disease;
- severe injury to the gland;
- complete blockage of the salivary ducts with the impossibility of restoring their patency.
Depending on the diagnosis, various tests are prescribed before the operation - ultrasound, computed tomography or magnetic resonance imaging, chest x-ray. In the case of a tumor, a biopsy is also necessary to determine the nature of the formation. Salivary stone disease is examined using contrast sialography.
Causes of parotid gland tumor
The causes of tumor growths of the salivary glands are not fully understood; it is believed that they can be caused by:
- past infections (influenza, scarlet fever, measles and others);
- various chronic diseases, especially diseases of the gastrointestinal tract (the salivary glands are part of a single digestive process);
- eating disorders;
- insufficient oral care;
- genetic factors and unfavorable environmental influences.
Hypertrophy of the masticatory muscles
Along with a tumor of the salivary glands, there is hypertrophy of the masticatory muscles, which also leads to disproportions of facial features, but is sometimes caused by dental and neurological problems. To understand the true causes of the deficiency, it is necessary to conduct a detailed examination and determine whether the glands are directly enlarged or just the muscles.
When it comes to muscle hypertrophy, botulinum toxin injections come to the rescue, blocking excessive muscle activity and over time they decrease in size.
Features of surgery on the parotid salivary gland
“It must be borne in mind that tumors of the salivary glands are often multicentric (that is, there may be several of them, and unevenly located), and if not all are removed at once, relapses are possible. Therefore, parotidectomy (removal) of all or most of the gland is performed, which subsequently does not in any way affect the normal secretion of saliva,” explains A.I. Nerobeev.
During the operation, which lasts about four hours due to its complexity, the doctor makes an incision in front of the ear, isolates the nerve and removes the tumor along its branches along with the gland tissue.
If the tumor occurs in adulthood, a facelift can be performed simultaneously with surgical removal of the parotid gland, especially since the incisions are made in approximately the same places. Such operations are successfully carried out at the ART Clinic. The result of the combined approach is not only the patient’s health, but also his rejuvenated appearance.
After removal of the salivary gland, it is necessary to warn cosmetologists about this, since fillers cannot be injected into the parotid area.
Muscles of the submandibular triangle
Muscles of the submandibular triangle
The submandibular triangle consists of the following muscles:
- digastric;
- stylohyoid;
- maxillohyoid;
- sublingual-lingual.
The digastric and stylohyoid muscles are the boundaries of the triangle, and the mylohyoid and mylohyoid are involved in the formation of its bottom.
The first muscle consists of 2 parts: the anterior and posterior abdomen. The posterior abdomen begins from the temporal bone, or rather from its mastoid notch. The anterior one originates on the body of the lower jaw. They have a common second attachment point - the hyoid bone.
The stylohyoid muscle is located near the posterior abdomen, tightly adjacent to it. Its beginning is located at the styloid process, and its end is also at the hyoid bone.
The mylohyoid muscle is located deeper than the digastric muscle. Its attachment points are the mylohyoid line on the lower jaw and the hyoid bone. The right and left muscles form the suture of the bottom of the lower jaw and participate in the formation of the diaphragm of the mouth.
The mylohyoid muscle seems to continue the mylohyoid muscle. Having the same starting point, it ends on the lateral surface of the tongue.
Important anatomical structures pass through this muscle:
- lingual vein;
- hypoglossal nerve;
- salivary gland duct;
- lingual nerve.