Introduction
Facial pain (prosopalgia, orofacial pain) is a conventional collective clinical term that unites all pain syndromes localized in the facial area.
According to the International Classification of Diseases, 10th revision (ICD-10), facial pain is divided into those associated with pathology of the anatomical structures of the head and neck, cranial neuralgia and central pain; facial pain is coded G 50.1 - atypical facial pain [1]. According to the terminology of the International Association for the Study of Pain (IASP), orofacial pain is a type of pain that is felt in the face and/or oral cavity [2]. When discussing the problems of facial pain, there is increasing evidence that psychosocial factors have a significant impact not only on treatment outcomes, but also act as prognostic factors for the development of pain syndrome [3]. Many patients with this problem have comorbid conditions, and there are also mental or personality disorders that predispose to chronic pain and thereby affect the outcome of treatment [4]. The results of epidemiological studies indicate that, along with pain syndromes of various localizations, facial pain is one of the causes of disability. It should also be noted that prosopalgia mainly affects women of working age (from 27 to 50 years) [5, 6]. Only 46% of patients with orofacial pain seek medical help, with dentists, neurologists and family doctors prevailing among specialists [5, 7]. In 17% of patients, pain significantly limits their ability to work [8, 9]. Until now, many authors have pointed out the dominant role of trigeminal neuralgia among prosopalgia, while pain in the facial area is represented by a significantly larger number of nosological forms [10]. Thus, in the work of RW Evans (2006) it was shown that in patients with facial pain in 83% of cases there is an overdiagnosis of trigeminal neuralgia, in 100% of cases there is an unsatisfactory diagnosis of idiopathic persistent facial pain as a diagnosis of exclusion [11]. S. Marklund et al. (2010) in a population-based study, using strictly defined pain criteria and examining the neurological status of patients suffering from headaches, showed that trigeminal neuralgia is more common than chronic idiopathic facial pain, but both conditions are rare, and the prevalence of trigeminal neuralgia in lifetime is 0.3% compared to 0.03% for persistent idiopathic facial pain [12].
JS Koopman et al., using research databases of all primary care physicians in the Netherlands, reviewed all cases of trigeminal neuralgia and persistent idiopathic facial pain and found an incidence of 38.7% per 100,000 people [13]. The diagnosis was confirmed by pain diagnostic criteria and found that approximately 48% of patients were misdiagnosed by primary care physicians. Trigeminal neuralgia and cluster headache were the most common types. On the other hand, temporomandibular joint pain (TMJ) and myofascial facial pain syndrome (MFPS) are common in approximately 10–15% of the adult population [14, 15].
According to S. Wirz et al., among patients with chronic facial pain, persistent idiopathic facial pain is represented in 5.8% of cases and is one of the three most common causes of chronic prosopalgia [16]. In the last decade, many authors have reported a wider representation of both MFPS and TMJ dysfunction among patients with facial pain, indicating the dominant role (in 75% of patients) of the muscular-tonic and dysfunctional components in the formation of prosopalgia [6]. There is no doubt that mental health affects pain, with depression and anxiety being particularly significant. It is now known that there are markers of fear and anxiety that increase chronic pain [17, 18].
Patients with borderline personality disorder have been found to have higher levels of pain perception than other patients with the same pain [19].
T. Taiminen et al. reported that of 63 patients with burning mouth syndrome or atypical facial pain, more than 50% had a lifetime history of mental health disorders, including depression. The researchers indicated that these disorders preceded the onset of facial pain. According to the authors, these syndromes may be mediated by dysfunctional dopamine activity in the brain [3]. Recent recommendations for the rehabilitation of patients with temporomandibular disorders also emphasize the need to identify patients with mental health problems (so-called “red/yellow flags”) [20].
Such heterogeneity in the epidemiological features of orofacial pain can be explained by the complexity of the anatomical and functional organization of the face, the difficulty of objectively identifying the causes for most types of facial pain, the absence of a morphological cause of the disease, and concomitant psycho-emotional disorders, such as depression, in the group of patients under consideration.
Trigeminal facial pain: systematics of clinical forms, principles of diagnosis and treatment
Facial pain, which includes pain on the surface of the face and/or in the mouth (orofacial pain), is one of the most common types of pain. Most often, orofacial pain manifests itself as acute dental pain, which usually regresses after dental treatment. However, in a number of cases, facial pain itself (prosopalgia) is noted, manifested by chronic or recurrent pain, often resistant to various methods of conservative treatment. A kind of primacy in severity belongs to trigeminal facial pain, especially trigeminal neuralgia and deafferentation trigeminal neuropathy, during exacerbation of which the severity of pain is many times greater than the intensity of acute toothache familiar to most people.
Taxonomy of trigeminal prosopalgia
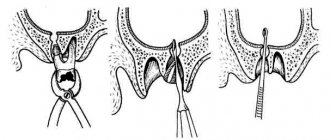
Trigeminal prosopalgia (Greek prosopon (face) + algos (pain)) includes facial pain caused by damage to the trigeminal nerve. From the point of view of topical diagnosis, the development of any form of trigeminal prosopalgia is associated with damage to the peripheral trigeminal neuron - the peripheral trigeminal branches, the sensory trigeminal ganglion (located at the base of the skull), the sensory root of the trigeminal nerve that follows it in the direction of the brain stem, as well as those entering the brain stem sensory trigeminal fibers and sensory nuclei of the trigeminal nerve (
).
Despite the difference in the symptomatology of the clinical forms of trigeminal prosopalgia, the features of facial pain are of primary importance for their differentiation, in some cases manifested by prolonged (constant) pain, and in others in the form of paroxysms of pain. Paroxysmal forms of trigeminal pain are traditionally referred to as neuralgia, and non-paroxysmal forms - trigeminal neuropathy. However, non-paroxysmal postherpetic facial pain is also called neuralgia. These forms of facial pain—neuralgia and trigeminal neuropathy—fundamentally differ in their approaches to treatment.
Paroxysmal trigeminal prosopalgia
Paroxysmal facial pain, lasting from several seconds to several minutes, is manifested by trigeminal neuralgia (typical trigeminal neuralgia), trigeminal neuralgia due to multiple sclerosis, and symptomatic trigeminal neuralgia arising from a tumor lesion of the trigeminal nerve.
Until recently, trigeminal neuralgia, not associated with multiple sclerosis and tumor lesions of the trigeminal nerve, was called idiopathic, i.e. occurring for no apparent reason. However, as it was established as a result of serial neurosurgical interventions, the main etiological factor of typical trigeminal neuralgia is compression of the sensory root of the trigeminal nerve by an atypically located arterial or venous vessel.
Trigeminal neuralgia
Trigeminal neuralgia is the most common form of paroxysmal (paroxysmal) facial pain. It is also considered the most excruciating type of facial pain. It manifests itself as attacks of sharp, high-intensity pain in the area of innervation of the trigeminal nerve. The cessation of an attack of facial pain within a few tens of minutes after taking the anticonvulsant carbamazepine radically distinguishes trigeminal neuralgia from most other types of chronic pain. The symptoms of trigeminal neuralgia undergo significant changes as the pain syndrome increases and regresses, reaching its greatest severity at the height of the exacerbation period.
In secondary (symptomatic) forms of trigeminal neuralgia, which arise from tumor damage to the trigeminal nerve, already at the first stage of the disease symptoms may be observed that differ from the typical clinical picture.
Non-paroxysmal trigeminal prosopalgia
Non-paroxysmal trigeminal prosopalgia, manifested by prolonged facial pain, as well as sensitivity deficit (hypesthesia, anesthesia) in the facial area, includes various clinical forms of trigeminal neuropathy, including postherpetic neuralgia (). Most often, the development of trigeminal neuropathy is associated with obvious etiological factors - trigeminal herpes zoster and traumatic injury to the trigeminal nerve. In some cases, trigeminal neuropathy is one of the early manifestations of systemic diseases, in particular systemic scleroderma, systemic lupus erythematosus, sarcoidosis and Lyme disease.
Traumatic trigeminal neuropathy
It is the main form of trigeminal neuropathy, the clinical signs of which are non-paroxysmal facial pain, sensory impairment (numbness) and, very rarely, motor impairment. As a rule, the acute development of these symptoms has an obvious relationship with local pathological processes and iatrogenic effects in the maxillofacial area.
The first sign of traumatic trigeminal neuropathy is acutely developed sensory insufficiency - from mild hypoesthesia to anesthesia, limited to the innervation zone of the affected sensory branch. Subsequently, paresthesia (a feeling of “pins and needles”) and/or non-paroxysmal pain occurs in the same area of the face. Symptoms of sensory loss that accompany facial pain may persist significantly longer than facial pain. In the affected area, hyperesthesia is often detected, as well as pain on palpation of limited areas of facial skin.
Postherpetic trigeminal neuralgia
Trigeminal postherpetic neuralgia is persistent facial pain and/or burning and itching that persists from the time herpetic lesions develop or occurs several weeks after the lesions resolve (delayed postherpetic neuralgia).
Trigeminal postherpetic neuralgia most often develops in patients over 60 years of age. Its occurrence is usually facilitated by:
- late seeking medical help during the period of acute herpes zoster;
- presence of concomitant pathology;
- complicated resolution of rashes - rashes with a hemorrhagic component and secondary pyoderma;
- pronounced residual sensory deficit (“numbness” of the skin after resolution of the rash).
Deafferentation trigeminal neuropathy (prosopalgia)
Deafferentation facial pain (prosopalgia) is the most severe form of trigeminal lesion, manifested by highly intense facial pain, often resistant to conservative therapy, and severe sensory impairment. Develops as a result of significant damage (destruction) of the peripheral or central structures of the trigeminal system.
The concept of “deafferentation trigeminal prosopalgia”, as a general syndromological definition, was proposed by Yu. V. Grachev and Yu. A. Grigoryan (1995) to designate a special form of facial pain that develops as a result of deafferentation in the sensory system of the trigeminal nerve. The pathophysiological term “deafferentation” (de- + lat. afferentis bringing), literally means the separation of the receptor zones of peripheral nerves from the central sensory structures, due to a violation of the integrity or conductivity of nerve fibers.
Typical peripheral forms of deafferentation trigeminal prosopalgia are postherpetic, tumor and iatrogenically caused facial pain (caused by destruction of the ganglion and trigeminal nerve root), and central are two quite rare forms caused by syringobulbia and medulla oblongata infarction.
Diagnosis of trigeminal prosopalgia
The examination of a patient experiencing facial pain should begin with a systematic medical interview, including clarification of the clinical characteristics of the pain and analysis of anamnestic data (
).
The presence of facial pain requires a detailed study of the function of the cranial nerves, and also makes certain additions to the traditional neurological examination. Objective signs of damage to the nervous system of the face are sensory disturbances in the orofacial region - trigger zones, areas of increased and/or decreased sensitivity (Fig. 2, 3), local autonomic disorders, as well as the presence of local palpation pain.
| Rice. 2. Pattern (model) of sensory disturbances characteristic of exacerbation of paroxysmal trigeminal prosopalgia - neuralgia | Rice. 3. Pattern (model) of sensory disturbances characteristic of exacerbation of non-paroxysmal trigeminal prosopalgia - neuropathy |
When conducting palpation examination of the facial area, it is necessary to distinguish between “neuralgic” and “myofascial trigger” (English trigger).
- Neuralgic trigger points or zones (in patients with trigeminal neuralgia) are hyperexcitable areas of the skin and mucous membrane, with mechanical irritation, including light touch, causing a painful attack. At the same time, strong pressure, usually applied by the patient himself, not only does not cause pain, but in some cases leads to a decrease or disappearance of pain.
- Myofascial trigger points (essentially pain points) are located in the soft tissues of the face in the projection of the masticatory muscles. “Pressing” on them is accompanied by localized or radiating pain.
Establishing a specific form of trigeminal facial pain, which usually requires an interdisciplinary clinical examination, involves excluding a number of forms of orofacial pain not associated with damage to the trigeminal nerve, in particular temporomandibular (arthrogenic and myofascial), symptomatic (ophthalmo-, rhino- and odontogenic) and psychogenic prosopalgia.
Treatment of trigeminal prosopalgia
The complexity of treating patients with trigeminal facial pain is due to the need to determine differentiated treatment approaches due to the ineffectiveness of the use of conventional analgesics for certain forms of trigeminal prosopalgia, the frequent need to change standard treatment regimens and, in some cases, the development of “pharmacoresistant” forms of facial pain that require surgical treatment.
The ineffectiveness of traditional analgesics (for example, NSAIDs) prescribed in connection with the development of trigeminal facial pain is an indication for the use of drugs from other groups, in particular carbamazepine, gabapentin or amitriptyline, which have analgesic activity in a number of forms of prosopalgia (scheme of differentiated therapeutic approaches for paroxysmal and non-paroxysmal trigeminal prosopalgia is presented in
).
Over the past few decades, carbamazepine has remained the most effective and affordable drug in the treatment of patients with trigeminal neuralgia. At the same time, the maximum effectiveness of carbamazepine (as a “monotherapy”) appears in the initial period of the disease. The main indication for the use of carbamazepine is paroxysmal pain, covering the area of innervation of the trigeminal nerve. The daily dose of carbamazepine during an exacerbation of trigeminal neuralgia is usually 600–1200 mg (with a 3–4-time dose of the usual dosage form or 2 times of the retard form), but with uncontrolled use by a doctor it often exceeds 2000 mg/day. As neuralgia regresses, a transition is made to maintenance doses of carbamazepine and its gradual withdrawal when facial pain disappears. If there are contraindications for the prescription of carbamazepine or its forced withdrawal, gabapentin is used as an alternative remedy for the elimination of paroxysmal trigeminal pain.
Gabapentin (Gabagamma) is an anticonvulsant that has an analgesic (GABAergic-like) effect. Obviously, this explains its effectiveness in the treatment of patients with neuropathic pain, including paroxysmal and non-paroxysmal trigeminal prosopalgia. Indications for the use of gabapentin (Gabagamma) are paroxysmal facial pain in trigeminal neuralgia and trigeminal neuralgia caused by multiple sclerosis, as well as subacute and chronic non-paroxysmal pain (including deafferentation) in herpetic and traumatic trigeminal neuropathy. The daily dose of Gabagamma in patients with trigeminal prosopalgia can range from 300 to 1500 mg, with a dosage frequency of at least 3 times a day. Gabagamma is used for a long time and is gradually withdrawn. In general, the use of gabapentin (Gabagamma) is considered safer than carbamazepine and especially amitriptyline.
Amitriptyline is a tricyclic antidepressant that is a norepinephrine and serotonin reuptake inhibitor. This drug is widely used for the treatment of postherpetic neuralgia, especially accompanied by a burning sensation. The analgesic effect of amitriptyline usually develops within 1–2 weeks. To reduce the sedative and anticholinergic effects of amitriptyline, treatment begins with small doses of the drug - 10 mg 2-3 times a day (especially at night), gradually increasing the daily dose (due to evening administration) to 75-100 mg. If amitriptyline is insufficiently effective and facial pain persists, gabapentin (Gabagamma) is indicated.
Treatment of patients with damage to the trigeminal nerve also includes the use of high doses of B vitamins in the form of multicomponent preparations “Milgamma” and “Milgamma compositum”. The composition of the drug "Milgamma" (solution for intramuscular administration) includes 100 mg of thiamine and pyridoxine, 1000 mcg of cyanocobalamin and 20 mg of lidocaine. Milgamma compositum is available in the form of tablets containing 100 mg of benfotiamine and pyridoxine. The effectiveness of Milgamma in the treatment of patients with neuropathic pain is associated with inhibition (probably serotonergic) of nociceptive impulses, as well as acceleration of the regeneration of axons and the myelin sheath of peripheral nerves. The regimen for using Milgamma for trigeminal facial pain includes: prescribing Milgamma in the form of a solution for intramuscular administration - 2 ml daily, for 10 or 15 days, then Milgamma compositum - orally, 1 tablet 3 times a day, for 6 weeks.
Yu. V. Grachev , Doctor of Medical Sciences, V. I. Shmyrev, Doctor of Medical Sciences, Professor, Scientific Research Institute of Advanced Promotion of the Russian Academy of Medical Sciences, State Medical University of the Administration of the President of the Russian Federation, Moscow
Nociceptive pain
The most common causes of nociceptive facial pain are diseases of the teeth and periodontal tissue [5, 21]. Odontogenic pain is one of the most common and painful. It is capable not only of irradiation, but also of repercussion (reflection into other zones). Few dental diseases are chronic, but given their high prevalence, they should be diagnosed in patients with chronic facial pain [22, 23].
Thus, it is known that when a wisdom tooth is damaged or even difficult to erupt, pain can be felt in the ear and the TMJ area. When the molars of the upper jaw are affected, pain may occur, spreading to the temporal region and upper jaw. Damage to the molars of the lower jaw can cause pain reflected in the area of the larynx and crown, the sublingual area. With pathology of the incisors, pain is usually reflected in the area of the nose and chin [24]. Intraoral pain not associated with dental tissues also occurs (in case of damage to the oral mucosa, tongue, or periodontal tissue). Cases of nerve injury due to either dental procedures or trauma have been reported in the literature. Recently, an international group of experts proposed the use of the term “persistent dentoalveolar pain disorder” to classify persistent pain without local disease (other names such as “atypical odontology” or “phantom toothache” are also found) [25]. Terms such as post-traumatic trigeminal neuropathy, peripheral painful traumatic trigeminal neuropathy may be used in cases where there is a clear correlation between the injury and the development of pain [21].
How to get rid of toothache?
In order to relieve sudden toothache, it is recommended:
- refuse to eat too rough food, confectionery, ice-cold, too hot or sour foods, drinks (even up to a visit to the dental clinic);
- brush your teeth thoroughly, making sure that there are no food particles left in the cavities formed;
- rinse your mouth with a soda solution (dissolve 5-7 g of baking soda in a glass of heated water, if desired, you can add 6-7 drops of iodine to the solution);
- Rinse your mouth with freshly prepared sage infusion for 15 minutes (to prepare a rinse, add 150 ml of boiling water to a tablespoon of the herb and leave for at least half an hour);
- take orally a small dose of analgin, ibuprofen or other analgesic drugs;
- Apply a piece of ice or a cold compress to the painful tooth or cheek on the affected side.
Light acupressure can be an effective remedy for pain. In most cases, in order to significantly reduce the pain, it is enough to gently massage the small depression located between the lips and nose, or the V-shaped area formed by the index finger and thumb on the affected side.
Neuropathic pain
Episodic neuropathic pain includes paroxysmal neuralgias, of which the most common is trigeminal neuralgia (TN). The main reason for its development is local demyelination of the trigeminal nerve due to mechanical compression (by a vessel) or an autoimmune process, for example, in multiple sclerosis. In the second case, local demyelination and the formation of ephaptic transmission are morphologically detected; It is known that TN may be the only early sign of multiple sclerosis. An epidemiological feature of TN is that its frequency is higher in women and elderly patients. The clinical picture of TN is characterized by short paroxysms of pain of a burning, shooting, lightning-fast nature (duration - several seconds), usually provoked by irritation of trigger points in the face. However, this is often limited to only the branch of the nerve involved in the pain syndrome. Characterized by a refractory period (from 30 s to 5 min) and antagonistic gestures when the trigger zones are irritated immediately after the end of the previous attack. Features of this pain syndrome are contraction of the muscles of the corresponding half of the face and retraction of the corner of the mouth. These muscle contractions are referred to as tonic and clonic convulsions, which appear as a result of the transmission of excitation from the trigeminal nucleus to the facial nerve [10].
Paratrigeminal Roeder syndrome is distinguished separately
, in which the orbital and maxillary branches of the trigeminal nerve are most often affected in combination with fibers of the anterior sympathetic plexus. One of the most serious causes of this syndrome is a tumor in the immediate vicinity of the Gasserian node. In this case, the nature of the pain differs from classical neuralgia: attacks are very sharp, shooting in the orbital area on the affected side, often begin in the morning and last continuously for several hours, sometimes accompanied by nausea or vomiting and Bernard-Horner syndrome [22].
Tolosa-Hunt syndrome (painful ophthalmoplegia).
The disease was described by FJ Tolosa (1954) and, in more detail, by WE Hunt (1961) [26]. Currently, the cause of this syndrome is considered to be an infectious-allergic lesion of the dura mater in the area of the superior orbital fissure involving the orbital, abducens, trochlear, oculomotor nerves, the wall of the internal carotid artery (periarteritis) and the sympathetic fibers lying on it. The picture of the pain syndrome has a bright vegetative coloring; pain of a constant nature in the forehead, orbit, and retrobulbar space is described as “braining,” “gnawing,” “drilling.” Sensory disorders are often detected, such as symptoms of prolapse - hyposthesia in the area of innervation of the first branch of the trigeminal nerve. Occasionally, when the process spreads to the apex of the orbit, there is a decrease in visual acuity with signs of atrophy in the fundus. The duration of the disease ranges from several days to weeks [26].
SUNCT syndrome
(eng. Short-lasting, Unilateral, Neuralgiform headache with Conjunctival injection and Tearing) - short-term unilateral, neuralgic type headache with redness of the conjunctiva of the eye and lacrimation. This rather rare form of primary headache was first described by the Norwegian researcher O. Sjaastad in 1978 [27]. SUNCT syndrome is characterized by paroxysmal, unilateral pain, localized peri- or retroorbitally, lasting about 60 s, accompanied by local autonomic disorders. It is known that this disease most often occurs with remissions and exacerbations: up to 20 pain attacks are observed per day, most of which occur during wakefulness, although night attacks of pain are also possible (1.2%) [27].
Neuralgia of the tympanic nerve
. Described in 1933 by F. Reichert [28]. It is quite rare. It is considered as a type of neuralgia of the glossopharyngeal nerve, which is due to its anatomy. The etiology and pathogenesis are not reliably known. Localization of pain is the external auditory canal, the TMJ on the affected side and the area adjacent to it, sometimes in the depths of the ear. Painful paroxysms in this pathology occur spontaneously, without provoking factors, and are characterized by the absence of trigger zones; Moreover, after an attack, patients note itching and dull pain in the external auditory canal.
Myogenic pain and myofascial pain syndromes
It is known that myofascial disorders in the facial muscles develop according to the same mechanisms as in skeletal muscles and cause 10–20% of pain syndromes on the face [12]. With long-term fixed local hypertonicity in the masticatory, temporal and pterygoid muscles, secondary local disorders arise, such as vascular, metabolic, inflammatory, and they are regarded as trigger points. The most common etiological factors causing myofascial disorders on the face include malocclusion (Costen syndrome), characterized by pain in the TMJ area and specific sound signals in the inner ear (squelching, squeaking, ringing) that occur when opening the mouth and swallowing, as well as reflected pain from the muscles of the neck and upper shoulder girdle and the well-known psychophysiological phenomenon - bruxism [29].
Psychogenic pain.
Psychogenic pain is a diagnosis of exclusion. Facial psychalgia can occur with a depressive disorder, including “masked” depression. The pathogenesis of this type of pain is not completely clear; there is probably a decrease in the activity of antinociceptive systems of the brain [6].
In the treatment of such patients, cognitive behavioral therapy is used, as well as various relaxation techniques [30].