Headaches often occur due to dental errors or chronic dental diseases. A number of factors can cause the problem:
- remnants of roots or fragments in the socket after complex tooth extraction;
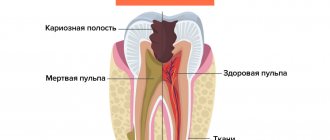
- pulpitis;
- periodontitis;
- galvanism due to fillings and dentures made of different metals;
- poorly installed or too high dentures;
- periodontal diseases;
- osteomyelitis of the jaw bones and other diseases.
More often, headache in pathologies of the dental system is a symptom of odontogenic neuralgia of the trigeminal nerve (more than 60% of cases) or dental plexalgia (diagnosed in 12% of patients), so we will consider these diseases in more detail.
Treatment of odontogenic trigeminal neuralgia
Therapy usually involves a combination of medications and physical therapy. At the first stage, patients are prescribed non-narcotic analgesics. If an inflammatory process is present, then it is recommended to take anti-infective drugs in parallel.
Physiotherapy at this stage may include:
- modulated currents,
- ultrasound,
- Ural Federal District,
- moderate heating.
After the pain subsides, they move on to the second stage of treatment. At this stage, electrophoresis of novocaine or calcium chloride is recommended. If the process is inflammatory, then phonophoresis with hydrocortisone is prescribed. In addition, it is important to begin treatment for the dental disease that caused the problem.
At the last recovery stage, biostimulants, treatment with mud or paraffin, and local use of ozokerite are useful.
Atypical facial pain
Pain that does not fit into the description of neurogenic, autonomic, musculoskeletal prosopalgia is classified as atypical facial pain . As a rule, their atypicality is associated with the simultaneous presence of signs characteristic of several types of pain syndromes, but the psychopathological component usually dominates.
SYMPTOMS AND DIAGNOSIS
One type of atypical facial pain is persistent idiopathic facial pain. The pain can be triggered by surgery on the face, trauma to the face, teeth or gums, but its persistence cannot be explained by any local cause. The pain does not meet the diagnostic criteria for any of the described forms of cranial neuralgia and is not associated with any other pathology. Initially, pain occurs in a limited area on one side of the face, for example, in the nasal fold or one side of the chin. In some cases, patients cannot accurately localize their sensations at all. In the area of pain, no sensitivity disorders or other organic disorders are detected. Additional research methods do not detect any clinically significant pathology. Another form of atypical facial pain is atypical odontalgia. This term is used to refer to prolonged pain in the teeth or bed after tooth extraction in the absence of any objective pathology. This syndrome is close to the so-called “dental plexalgia”. Among the patients, women of menopausal age predominate (9:1). Constant burning pain in the area of the teeth and gums is typical, often with repercussion to the opposite side. There are usually no objective signs of dental or neurological disorders, although in some patients the syndrome develops after dental procedures (simultaneous removal of several teeth or filling material extending beyond the apex of the tooth). In some cases, a decrease in pain during eating is observed and an increase in pain under the influence of emotions, adverse meteorological factors and hypothermia. When the superior dental plexus is damaged, pain can radiate along the second branch of the trigeminal nerve and be accompanied by autonomic symptoms, likely resulting from connections between the plexus and the autonomic ganglia (pterygopalatine ganglion and superior cervical sympathetic ganglion). As a rule, there is no pain at the exit points of the branches of the trigeminal nerve and no pronounced sensory disturbances in the zones of innervation of its II and III branches. Bilateral dental plexalgia develops almost exclusively in women after 40 years of age and has a long course. Burning pain usually appears on one side, but soon appears on the opposite side. Almost all patients develop pain on both sides within 1 year. The simultaneous development of bilateral pain is also possible. As with unilateral dental plexalgia, the upper dental plexus is affected 2 times more often than the lower one.
CAUSES
Possible etiological factors of bilateral dental plexalgia include complex removal of wisdom teeth, premolars and molars, conduction anesthesia, osteomyelitis of the sockets, surgical interventions on the jaws, entry of filling material into the mandibular canal through the root canals of the teeth, removal of a large number of teeth in a short period of time during preparation of the oral cavity for prosthetics, infection, intoxication, mental trauma, etc.
TREATMENT
Treatment should be carried out exclusively by a neurologist. Self-medication is unacceptable.
Signs and features of treatment of dental plexalgia
In this disease, the source of headaches are the structures of the dental plexus. The pain can be localized in the upper and lower jaw. Moreover, 50% of patients report discomfort only in the upper part of the jaw due to the fact that many people lack the lower nerve plexus.
If the upper jaw is affected, the pain can radiate to the palate, cheekbones, eyes, and back of the head. If the lower plexus is affected, pain may be felt in the upper neck, buccal and masticatory areas. In some cases, the pain affects the entire half of the head.
Signs of dental plexalgia:
- excruciating pain that affects the area of 3-7 teeth;
- numbness of the skin of the face or tongue may occur;
- sensations may intensify for several hours and then return to normal intensity;
- the pain becomes stronger when pressing on the area of the dental plexus and decreases while eating.
If you suspect this disease, it is important to consult an experienced doctor, because the problem is often confused with trigeminal neuralgia. Due to an incorrect diagnosis, the patient may be prescribed anticonvulsants or blockades, which are ineffective for this pathology.
Medical Internet conferences
The high prevalence and intensity of dental diseases forces almost every person to seek help from a dentist. Often the treatment is accompanied by the patient’s fear of dental intervention, discomfort and pain, which can provoke the appearance of various general complications during the intervention, as well as exacerbation of the patients’ chronic diseases. That is why studying the etiology, as well as the characteristics of dental pain, is important for the dentist. Pain is an unpleasant sensory and emotional experience associated with tissue damage. Dental pain is caused by dental lesions, divided into lesions of carious and non-carious origin. Carious lesions in the early stages cause short-term pain; as the process progresses, the pain becomes more intense, long-lasting, and continuous. Carious lesions include: caries, pulpitis, periodontitis. The clinical picture of non-carious lesions of teeth is characterized by a combination of pain and parasthesia. Examples of these lesions are odontogenic dental plexalgia, neuritis and alveolar neuropathies. The etiological factor in this case is errors during filling, tooth extraction and anesthesia. A feature of dental pain sensitivity is its reflection. Referred pain is pain in an area of the body that is distant from the actual source of the area. When the upper incisors and canines are affected, the pain is reflected in the frontonasal area, and maximum pain is observed in the area of the superciliary arch. Diseases of the first upper small molars, pain is generalized in the nasolabial area. When the second upper premolars are affected, the pain spreads across the upper jaw. Diseases of the first molars are accompanied by pain and maximum pain in the temporal region. Lesions of the second and third molars of the upper jaw cause pain in the lower jaw, the point of maximum pain is determined in the area of the tragus of the external ear. If the disease affects the incisors, canines and first premolars of the lower jaw, in this case the pain is felt in the chin area, the maximum pain is felt on the edge of the lower jaw. The projection zone for disease of the first and second molars is in the sublingual region, and maximum pain is felt in the corner of the lower jaw. With lesions of the third molars, pain sensitivity spreads mainly in the larynx and parietal region of the head. In conclusion, it should be noted that toothache has a number of specific features, a lot of etiological factors, the elimination of which is the main task of the dentist.
Diagnostic features
Dacryocystitis is easy to diagnose if you monitor the condition of the eye and notice the symptoms of the pathology in time. If you suspect dacryocystitis, you should contact an ophthalmologist who will conduct an examination and, if necessary, prescribe other methods for diagnosing the pathology. You should not draw conclusions on your own - dacryocystitis requires professional help and immediate treatment. Delaying therapy leads to complications.
Diagnosis of the disease includes the following methods:
- Primary examination and diagnosis is the initial stage at which the doctor will identify the symptoms of pathology in the patient, palpate the area, and assess the condition of the lacrimal canal.
- Vesta color test is carried out to assess the patency of the lacrimal canal and involves instilling the eye with a solution of fluorescein or collargol, which have a bright color and will clearly show whether there is a blockage of the canal. With normal patency, the dye will certainly remain on the napkin when the patient is asked to blow his nose after 5–7 minutes. If after 20 minutes the napkin remains clean, this means obstruction of the lacrimal canal and the presence of an inflammatory process (resulting in either blockage with purulent contents, or the disease is accompanied by significant swelling).
- Instillation test is similar to the Vesta color test and is carried out with the same fluorescein solution, after which the patient is examined using a blue lamp. The technique allows you to detect damage to the cornea, since the reagent stains only healthy tissue.
- Probing - determining the patency of the lacrimal canals using a Bowman probe. The procedure is performed under local anesthesia as it is quite painful.
- X-ray – carried out if pathology of the nasal cavities and sinuses is suspected, and with the help of X-ray you can determine the patency of the lacrimal canal and the presence of damage.
- Biomicroscopy of the eye is performed using a special device (slit lamp), which allows you to determine a number of pathologies, including dacryocystitis.
- Passive nasolacrimal test - application of special substances to the cornea, which are quickly washed off with an antiseptic, and then using a slit lamp, the staining of healthy tissues and the presence of unpainted pathologically altered areas are observed (they acquire a specific yellowish tint).
- Culture of discharge from the lacrimal canal to identify pathogenic microflora and prescribe the most effective medications for the treatment of the disease. The bacterial culture is taken in the morning, before hygiene procedures, and the doctor will receive the results of the study in about a week.
When examining the patient, the doctor will conduct a differential diagnosis with other ophthalmological pathologies, primarily with bacterial conjunctivitis, the symptoms of which resemble dacryocystitis, but the causes are different, and therefore the treatment tactics are different.
Types of pathology
Traditionally, the inflammatory disease dacryocystitis is divided according to the type of course into two types: acute form of pathology and chronic. It is noteworthy that the acute form can also have two options for the development of pathology - an abscess or phlegmon.
In most cases, the pathological process begins with a protracted, sluggish inflammation, in which patients experience lacrimation, the mucous membrane of the eye turns red, itching appears, and in the area of the lacrimal sac there is pain when pressed. Externally, there is swelling, and if you press on the corner of the eye, purulent contents are released. If you miss the first symptoms of the disease and do not treat dacryocystitis, then noticeable skin tension in the area of inflammation will soon appear. The area turns red, the skin becomes thin and shiny. If atrophy of the lacrimal sac occurs, ulcers may appear on the cornea.
The acute form of the pathology is more severe, and its course is pronounced. In the area of the lacrimal sac, significant redness of the skin appears, the eye swells, and the palpebral fissure decreases; sometimes there is complete adhesion and the inability to open the eyelid. The inflammation progresses quickly and can spread to the cheek or nasal cavity. As a result of the suppurative process, phlegmon or an abscess appears.
Acute dacryocystitis seriously worsens the patient's condition. Patients complain of severe weakness, fever and headache. Inflammation spreads to the tissues surrounding the lacrimal sac and the maxillary sinuses. Externally, the affected part of the face looks swollen, the cheek and nose are very swollen. When purulent contents accumulate over time, it comes out - the abscess opens with a fistula. If the affected area takes a long time to heal, then the formation of a fistula with an exit outward or inward is possible. From there, tear fluid will be released, and when an outlet is formed, purulent contents will enter the nasal cavity. A significant complication of the pathology is the formation of phlegmon, which affects not only the subcutaneous tissue, but also muscle tissue.
Also, the classification of pathology subdivides the disease not only according to the nature of its course, but also depending on the causes of its occurrence. Dacryocystitis occurs:
- traumatic;
- viral;
- parasitic;
- bacterial;
- mycotic;
- chlamydial;
- allergic.
Doctor's comment
Chebotareva Tatyana Ilyinichna
Chebotareva Tatyana , head. Department of Radiosurgery, Radiation Therapist:
“Trigeminal neuralgia is characterized by very severe pain. These pains are so severe that patients are sometimes not helped by painkillers or even narcotics. And this forces them to look for special treatment methods.
Sometimes the clinical course of trigeminal neuralgia is quite lengthy - patients undergo several stages of treatment over a period of time (therapeutic methods, thermal procedures, surgical treatment). And when no option helps, they are forced to look for some other remedy.
And now the method of radiation therapy, namely radiosurgery, helps reduce and even eliminate pain. Because with radiosurgery we treat the level at which the trigeminal nerve exits the brainstem over a short distance. It all lies in the very small size of the field of influence of ionizing radiation on the area of the trigeminal nerve and in the high dose that we deliver. A small field of influence is determined by a zone located 4 mm from the brain stem and extending up to 6 mm. Such a small zone, which we influence with a large dose of ionizing radiation, leads to a decrease in the sensitive sphere of this nerve.
The trigeminal nerve has mixed functions - both sensory and motor. But with the help of radiosurgery, which in our clinic is carried out using the CyberKnife system, we act specifically on the sensitive area. A single dose ranges from 60 to 80 Gray once. With just one session of exposure to such a high dose, we are able to quickly cope with this disease.”