Inflammation of the facial nerve is an unpleasant ailment that does not go away painlessly. The main complaints of patients are sharp attacks of pain in the face, in the upper and lower jaws.
This inflammation is considered one of the most common among facial pains. Most often, the disease proceeds without a trace, but if treatment is neglected, paralysis may occur.
The disease most often occurs in women over 50 years of age; men are treated with this disease much less frequently. People with a genetic predisposition, such as a narrow bone canal, are also at risk. Due to this anatomical feature, there is an increased risk of pinching due to impaired blood supply and various inflammations.
What is the facial nerve?
The trigeminal nerve, also known as the facial nerve, is the largest of the twelve cranial nerves. It originates in the ear, after which it branches, the first path reaches the frontal part, the second is located at the jaw. The nerve goes around almost the entire surface of the human face; it literally controls it.
Every person has two facial nerves - one on each side of the head. It is in contact with other cranial nerves and has supersensitive fibers.
Doctors divide the disease into two types - primary and secondary. The primary one manifests itself as a complication from a cold, in this case the normal nutrition of the nerve is disrupted. Secondary occurs with severe intoxication against the background of inflammatory or infectious diseases, as well as tumor processes.
Causes of inflammation of the trigeminal nerve on the face
Usually the disease is caused by infection or bacteria. List of reasons why inflammation of the facial nerve may occur:
- Temporomandibular joint injuries
- Tumors (benign and malignant) of the brain and facial area
- Anomalies of skull development
- Skull injuries - birth, fracture, base, damage to the face or jaw
- Polio
- Pulmonary tuberculosis
- Otitis
- Sinusitis
- Chronic caries
- Inflammation after tooth extraction or treatment
- Hypertension
- HIV and AIDS
- Poisoning
- Inflammation of the middle ear
- Severe hypothermia of the head
- Changes in hormonal levels in women
- Gum inflammation
- Ramsay Hunt syndrome
- Stroke
- Bell's palsy
Causes range from minor to life-threatening illnesses. Each of the reasons determines the further treatment of the patient. In some cases, special tests are performed for diagnosis - auditory, lacrimal, infectious, salivary or gustatory. In this way, the functioning of the receptors and sensory organs is checked.
Causes
The organs of the skull are interconnected by a network of blood and lymphatic vessels and cranial nerves. These are the channels through which the infection is transmitted from the ears to the eyes, passes to the throat and back. The symptoms are complex. It is difficult to determine the source of inflammation. But there are several main causes of pain in the ears and eyes.
Neuralgia
With inflammation of the trigeminal nerve, pain spreads to the forehead, temple on one side of the face, and ear. The eye muscle on the affected side, the brow ridge, hurts.
The temperature remains normal. The pain comes in attacks, especially severe at night. The site of inflammation is sensitive to touch.
Causes of neuralgia:
- pathologies of the development of skull bones;
- compression due to tumor;
- traumatic brain injury.
The disease is difficult to diagnose. Treatment consists of pain relief. The sensitivity of the trigeminal nerve increases with the changing seasons. Psychosomatic neuralgia manifests itself as an exacerbation of pain during stress.
Otitis
Inflammation of the middle ear occurs due to the spread of coccus bacteria, which causes a runny nose. Otitis externa and otitis media are distinguished. The auricle becomes covered with boils due to the spread of infection from the ear canal.
A fungal infection also spreads in the middle ear. The fungus appears due to the accumulation of moisture.
The eye is affected by the affected ear. The infection occurs when one bottle of drops is used simultaneously to treat the eyes and ears. The result is lacrimation and redness of the conjunctiva.
Labyrinthitis
The inner ear consists of a plexus of passages and resembles a labyrinth. Labyrinthitis is inflammation in the inner part of the hearing aid.
Causes of the disease:
- spread of infection from the middle ear;
- tuberculosis;
- fungus;
- mechanical damage.
Symptoms of labyrinthitis appear 2 weeks after recovery from a respiratory infection. The disease causes dizziness and nystagmus - involuntary movement and tremors of the eyeballs.
Migraine
Hemicrania occurs on one side of the head. Throbbing pain is accompanied by photosensitivity. With migraine with aura, the field of vision is lost. Aching ear pain is accompanied by noise and ringing. In severe conditions, a person experiences auditory hallucinations.
Osteochondrosis
Salt deposits in the intervertebral discs of the cervical spine pinch blood vessels. As a result, brain tissue and cranial organs receive little oxygen. There is sand and a burning sensation in the eyes. There is stuffiness and ringing in the ears.
Intracranial pressure
Increased tone of the vessels of the cranium is a consequence of osteochondrosis. Other causes of pressure:
- thrombosis;
- traumatic brain injury;
- tumor;
- hypertension;
- accumulation of cerebrospinal fluid.
A drawing, throbbing pain is concentrated on one side of the head, covering the eye and ear.
Flu
An acute respiratory infection affects the mucous membranes of the nose and throat. Abundant mucous masses accumulate in the nasal sinuses. Rhinitis develops into sinusitis, inflammation of the inner, middle ear. Obstruction of the nasal passages deprives the tissues of oxygen.
The eyes feel dry, small capillaries burst due to coughing attacks. This creates a complex of symptoms characteristic of various colds. Only a doctor can make an accurate diagnosis.
Tumor
New growths in the brain create compression on surrounding structures. Pressing pain appears as the tumor grows penetratingly. Compression of blood vessels and nerves causes visual and hearing impairment. Symptoms are characteristic of various diseases, so oncological pathology is difficult to establish.
Symptoms of inflammation of the trigeminal nerve
Experts include short-term, but acute and intense pain in different parts of the head as the main symptoms of facial neuralgia. Shooting attacks spread over the entire surface of the face - lips, eyes, nose, upper and lower jaw, gums and tongue.
Patients also report the following symptoms:
- Metallic taste in the mouth
- Muscle weakness
- 2-3 days before facial expressions are affected, pain occurs behind the outer ear, spreading to the face, back of the head and eyes
- Facial asymmetry
- Inability to close the eye on the affected side
- Drooping corner of the mouth
- Dry mouth
- Slurred speech
- Cross-eyed strabismus
- Uncontrollable tearing
- Disorders of taste buds
- Increased drooling
- Facial muscle spasms
- Increased or decreased facial sensitivity
- Temperature increase
Due to discomfort and pain, the patient begins to develop a phobia and increased anxiety. He tries to avoid poses and movements that provoke discomfort.
Diagnosis of inflammation of the trigeminal nerve
Depending on the affected area and the set of symptoms, the strategy for diagnosing the disease is determined. To determine the location of nerve damage, the severity and dynamics of recovery, doctors prescribe a hardware diagnostic method, for example, electromyography. MRI and CT scans are used to determine the presence of tumors in the brain.
The patient may also be referred for a general or biochemical blood test, x-ray of the lungs, ultrasound of soft tissues or ophthalmoscopy.
You can be confident in the quality of the procedures performed in the clinic and the high accuracy of the results of MRI, CT and other methods of diagnosing various diseases. Medunion performs magnetic resonance imaging of all types: head, spine, abdominal cavity and joints using modern equipment.
Prevention
How to prevent the occurrence and spread of infection:
- treat colds promptly;
- do not overcool your head;
- Dry your ears thoroughly after bathing;
- take vitamins to strengthen the immune system;
- use separate bottles of universal drops for treating eyes and ears;
- Carefully clean the ears with cosmetic sticks so as not to damage the eardrum.
Compliance with the rules of prevention and immediate treatment prevents complications. Independent choice of drops, antibiotics, irregular use of drugs only until the first improvement introduces the disease into a chronic state.
The consequence will be the transfer of infection to the lining of the brain - meningitis.
Treatment for inflammation of the facial nerve
Drug treatment
Treatment of trigeminal neuritis is complex. The disease is first treated with medication - the patient is prescribed drugs that will alleviate the situation. These include painkillers, decongestants, vasodilators and B vitamins. Most often, the recommended medications are tablets, but you can speed up the recovery process by using ointments and gels. Sometimes doctors prescribe intramuscular injections.
In special cases, the recovery process of the facial nerve may be slowed down. Then the patient is prescribed glucocorticosteroids, which improve the metabolic processes of nervous tissue. Various biostimulants and hyaluronidases also contribute to a speedy recovery.
You cannot prescribe medications for yourself. Be sure to see a neurologist or neuropathologist at the first symptoms to determine the diagnosis and treatment strategy. Recovery medications are recommended to patients on a case-by-case basis, paying attention to the presence of chronic diseases, symptoms, and so on.
Surgery
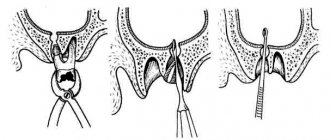
Another way to treat the facial nerve is surgery. However, doctors turn to this option quite rarely - only when the trigeminal nerve is ruptured. Surgery is also required if there is no effect from the conservative method after six months or a year. Surgical intervention is only relevant during the first year of the presence of the disease; later, the muscles on the face irreversibly atrophy.
The surgical process involves suturing the damaged area of the facial nerve to restore its motor function.
Massage
The next treatment method is massage for the treatment of the facial nerve. The purpose of this method is to remove swelling, improve blood circulation, restore sensitivity and conduction of nerve impulses. Massage is contraindicated for tuberculosis, oncology, atherosclerosis and elevated temperature.
Initially, the massage therapist works only with the healthy side of the face, collar area, neck and area above the shoulders. Basically, the master uses rubbing, stroking, kneading and vibration.
For noticeable desired changes, it is necessary to conduct ten to twenty massage sessions from five to fifteen minutes. The duration is determined based on the degree of inflammation of the trigeminal nerve, the goals of therapy and the dynamics of recovery.
Physiotherapy
The next treatment method is physical therapy. It alleviates the severity of symptoms, helps to activate metabolic processes in tissues and restore the functions of the facial nerve.
Doctors prescribe this course of treatment from the first days of the onset of neuritis. The list of physical procedures includes:
- Ultrasound
- Laser irradiation of blood
- Electrophoresis of drugs
- Microwave therapy
- Exposure to ultra-high frequency electricity
- Ozocerite treatment
- Myoelectrostimulation
- Darsonvalization
This complex is indicated for the first week of treatment. Doctors prescribe it together with medication. This tandem helps speed up the process of restoration of the facial nerve. And its most important advantages are the absence of side effects and painlessness.
Alternative Methods
There are also alternative treatment methods. These are procedures aimed at restoring facial muscles and eliminating the symptoms of facial neuritis. Such procedures include:
- Clay or paraffin masks
- Acupuncture
- Reflexology
- Injections to eliminate muscle disorders
- Therapeutic baths
- Taping – stretching the face using adhesive plasters
- Immunosorption – purification of blood from antigens and antibodies
- Biofeedback – facial muscle training
Gymnastics for the face
Also, in conjunction with complex treatment, you can do facial exercises. Before this, you need to consult with a specialist; the doctor will draw up an individual list of exercises based on the severity of the process, location of the lesion and symptoms. Typically, such gymnastics takes about ten minutes a day.
A standard set of exercises includes relaxing and tensing individual facial muscles. For example, to restore articulation, it is recommended to pronounce the sounds “u”, “o”, “and”. Afterwards, you need to bring your lower lip under your upper teeth and reproduce the sounds “v” and “a”.
Gymnastics for inflammation of the trigeminal nerve:
- Close eyes
- Raise your eyebrows
- Frown
- Squint
- Smile with your mouth closed
- Smile with your mouth open
- Puff up your cheeks
- Pull them back
- Whistle
- Widen your nostrils
- Curl your lips
- Raise your upper lip and return to the starting position
- Lower your lower lip and return to the starting position
- Take water into your mouth
- Rinse your mouth
- Close your mouth
- Run the tip of your tongue along your gums
- Move your tongue right and left
What diseases can a headache be a symptom of?
Yulia Vladimirovna Vostretsova, anesthesiologist-reanimatologist, pain treatment specialist at the department for the treatment of patients with chronic pain syndromes at City Clinical Hospital No. 52, tells the story.
Secondary headache is a symptom of an underlying disease. In case of secondary headaches, the main task is to treat the underlying disease, since if it is successful, this also has a positive effect on the symptom of the headache - it either stops completely or at least greatly decreases.
Headache associated with brain tumors
Contrary to popular belief, headache is not a common symptom of a brain tumor. Only 30% of patients with a diagnosed tumor complain of headache at the initial appointment, and in only 1-2% of patients headache is the only symptom of the tumor. This pain is often accompanied by other neurological symptoms, worsens with exercise or changes in body position, and causes night awakenings. However, such symptoms can also occur with primary headaches, such as cluster headaches and migraines, which we discussed in the previous article. Vomiting a week before the onset of a headache may be a sign of a mass formation in the posterior cranial fossa, as well as pain that occurs when coughing, lifting heavy objects, or bending over. The appearance of nipple discharge or amenorrhea in itself should alert the doctor and the patient, and in combination with a headache should suggest diseases such as polycystic ovary syndrome or prolactin-secreting pituitary adenoma. In patients with an already confirmed cancer diagnosis, new headache requires the exclusion of brain metastases or carcinomatous meningitis.
Headache associated with vascular pathology
Subarachnoid hemorrhage is “the worst pain imaginable,” a thunderous headache. Accompanied by stiffness of the neck muscles at normal body temperature. Approximately 25% of all cases of thunderclap headache are associated with subarachnoid hemorrhage. However, in 50% of patients with hemorrhages, the headache may be milder. The main features of headache associated with subarachnoid hemorrhage are localization in the occipital region, piercing nature, extremely rapid increase in pain intensity, as well as meningeal signs. Isolated headache may be a symptom of a ruptured aneurysm, arteriovenous malformation, or intracerebral hemorrhage. Aneurysm of the posterior communicating artery can manifest as double vision, absence or decreased reaction of the icon to light, loss of focus, divergent strabismus, the anterior communicating artery - weakness of both lower extremities, the middle cerebral artery - weakness in the extremities on one side. A sharp increase in intracranial pressure in the posterior fossa can lead to limited mobility of the eyeball, strabismus, double vision, nystagmus, dizziness and loss of balance. If the above symptoms are present and subarachnoid hemorrhage is suspected, CT without contrast and lumbar puncture are performed, and if necessary, MR or CT angiography.
Arterial dissection
Headache occurs in most cases of dissection (dissection) of the carotid artery - it is one-sided and intense, often accompanied by pain in the face and neck on the same side, the occurrence of Horner's syndrome (drooping eyelid, constriction of the pupil, exophthalmos).
Stroke
With ischemic stroke, headache occurs only in 27% of cases. The diagnosis is made on the basis of clinical symptoms, which vary depending on the location of the stroke. It should be kept in mind that migraine with aura increases the risk of stroke.
Venous sinus thrombosis
This is a fairly rare pathology in which headache is present in 90% of cases. Other symptoms include changes in consciousness and papilledema. Risk factors include female gender, pregnancy and the postpartum period, as well as taking estrogen-containing hormonal contraceptives.
Reversible cerebral vasoconstriction syndrome
Characterized by recurrent attacks of headache of very high intensity with a sudden onset and rapid peak (thundering headache). Angiography visualizes vasoconstriction (narrowing) of the cerebral arteries, which resolves over the next 3 months. The cause of this pathology is not fully understood, but it is known that certain substances, such as marijuana, tacrolimus, cyclophosphamide, as well as some drugs from the group of antidepressants, can be triggers. The incidence is also higher in the postpartum period. The headache is usually bilateral with attacks lasting from 1 to 3 hours and recurring over several weeks. Approximately 40% of patients experience nausea, vomiting, and neurological deficits. This condition is transient and requires symptomatic treatment.
Arterial hypertension
It often develops when systolic pressure rises to 180 mm Hg. or diastolic up to 120 mm Hg. This type of headache usually intensifies when the pressure rises and decreases when it decreases. The pain is usually bilateral or diffuse, may be throbbing and worsen with physical activity.
Headache due to heart disease
It is known that myocardial ischemia can also be accompanied by headache. A characteristic feature of such pain is its reduction against the background of resolution of ischemia (with the introduction of nitroglycerin, etc.).
Headache in systemic diseases
Giant cell arteritis
Headache that first appears in a patient after 50 years of age and is accompanied by weakening of the pulsation of the temporal artery should suggest giant cell arteritis. This is a systemic vascular disease with predominant damage to extracranial arteries of medium and large caliber. The disease begins acutely or subacutely with general weakness, low-grade fever, night sweats, insomnia, nausea, loss of appetite, weight loss, muscle and joint pain. Headache is the most characteristic symptom of temporal arteritis. It is localized more often in the temporal region, sometimes in the frontal and parietal regions of the head, less often in the occipital region (in case of involvement of the occipital artery). The spread of the process to the arteries of the face is accompanied by the appearance of acute spontaneous facial pain or a kind of “intermittent claudication” syndrome, that is, pain in the masticatory muscles and tongue when eating and talking. This symptom is pathognomonic for temporal arteritis. Many patients experience visual impairments that can lead to complete blindness. The cause of blindness is either ischemic damage to the optic nerve due to damage to the orbital and postciliary arteries, or blockage of the central retinal artery. Laboratory tests reveal an increase in CRP and ESR. This diagnosis can be accurately confirmed only after a biopsy of the temporal muscle.
Tolosa-Hunt syndrome
The syndrome is characterized by intense unilateral headaches accompanied by impaired movement of the eyeball; attacks occur every few months or even years. People over 40 years of age are most often affected. Pathogenesis is associated with nonspecific inflammation in the cavernous sinus of the superior palpebral fissure or orbital cavity. Impaired or complete absence of movement of the eyeball occurs as a result of granulomatous inflammation of the cranial nerves. The main clinical manifestations are acute unilateral pain in the eye area and the appearance of double vision.
Headache associated with infection
It makes no sense to dwell on this point in detail, since many infectious diseases can be accompanied by a headache. For headaches of very high intensity, accompanied by a stiff neck and other meningeal symptoms, it is important to perform the necessary examinations and begin treatment in a timely manner.
Post-traumatic headache
Headache occurs in 70-90% of cases of head injury. It can be considered post-traumatic if it occurs within 7 days after the injury or 7 days after the restoration of consciousness and the cessation of painkillers. The pain phenotype can be different, often migraine or tension-type headache, and such headache can be accompanied by nausea, dizziness, cognitive impairment, anxiety and insomnia.
Pain after craniotomy
This pain also occurs within 7 days after surgery and usually regresses over the next 3 months. In some cases, the headache may become chronic. Risk factors for chronicity include a patient's history of primary headaches, as well as surgical interventions in the suboccipital area.
Headache associated with diseases of the eyes, nose, ear, sinuses and other craniofacial structures
Acute angle-closure glaucoma
Angle-closure glaucoma is a form of pathology in which fluid accumulates inside the eyes due to lack of access to the drainage system (the iris covers the angle of the anterior chamber). The result is an increase in intraocular pressure, which can lead to an acute painful attack. An attack of angle-closure glaucoma may be similar to a migraine, as it is a unilateral pain in the eye area, accompanied by nausea/vomiting, photophobia, visual disturbances in the form of blurred visual images and iridescent halos around the light spot. When examined during an attack, redness of the conjunctiva and a moderately dilated pupil are noted. Between attacks, the appearance of the eyeball and intraocular pressure are usually normal. Triggers of attacks are often: sudden changes in lighting, prolonged reading, as well as some drugs, such as tricyclic antidepressants, topiramate, acetazolamide, etc. An ophthalmologist will help establish the diagnosis.
Trochleitis
Trochleitis is an inflammation of the oblique muscle of the eye. The pain most often occurs in the inner corner or above the eyeball and can spread to the entire half of the head. The pain intensifies with eye movement, the paraorbital area is painful on palpation. There is usually no lacrimation or discharge from the nose. Some patients may experience diplopia. The cause of trochleitis is often unknown (idiopathic trochleitis), but it most often occurs in patients with rheumatologic diseases such as systemic lupus erythematosus, rheumatoid arthritis, enteropathic arthropathy, and psoriasis.
Rhinosinusitis
The symptoms of rhinosinusitis are familiar to many. Rhinosinusitis can be either an independent cause of headache or an aggravation of the primary headache. The diagnosis is made on the basis of X-ray diagnostics by an ENT doctor. Usually this pain is preceded by an infectious disease with rhinorrhea and nasal congestion.
Headache associated with temporomandibular joint pathology
The causes of joint dysfunction can be trauma, joint asymmetry, disc displacement, joint hypermobility, osteoarthritis. The headache associated with this pathology usually corresponds to the side of the affected joint, but can also be bilateral if muscles are involved in the pathological process. The pain occurs in the projection of the joint and periarticular region and has the character of a pulling, aching, pulsating or acute pain that can radiate to the ear, temporal or parietal region. Pain can occur at rest, but is often provoked by chewing or simply moving the temporomandibular joint.
Seek help from specialists!
Headaches should not be ignored! A pain treatment clinic specialist is called upon to understand the probable causes of its occurrence. After a detailed neurological examination, a further examination may be prescribed to clarify the underlying disease, the symptom of which is pain in the head. Our pain treatment clinic uses many treatment methods - which of them can help a particular patient will be decided by the doctor during a face-to-face consultation.
Disease prevention
Doctors recommend eliminating effects on the body that cause inflammation of the trigeminal nerve. Here are some recommendations to help avoid illness:
- Avoid drafts and hypothermia
- Keep your head warm during the cold season
- Monitor your blood pressure
- Timely treatment of infectious and bacterial diseases
- Have a routine check-up with an oncologist
- Avoid skull and head injuries
You can sign up for an individual consultation, take tests or undergo treatment at the Medunion private clinic. You can easily make an appointment with us by calling 202-95-54 or online, directly on the website, by clicking on the “Online booking” button.
We have been working in Krasnoyarsk since 2006 and provide high-quality medical services to the population. The staff consists of highly qualified doctors of broad and narrow specialization.