Tooth canal treatment: when is it necessary and how is it carried out?
Tooth canal treatment is a procedure that is carried out for certain indications and allows you to stop active inflammation in the internal tissues of the tooth and avoid the removal of a dental unit. Treatment of tooth canals has its own specifics and is complex; only an experienced and competent specialist can carry out the procedure efficiently. In the article we will look in detail at the process of root canal treatment: we will find out under what circumstances the procedure is carried out, how it goes, what methods are used for treating tooth canals.
Development of root canals - the basis for treatment success (part 2)
Rudolf Beer (Dr. Rudolf Beer) professor (Essen, Germany)
The first information about attempts to use machine methods for developing root canals appeared in the literature about a hundred years ago. In this article, the author presents common root canal development techniques: Step-back, Step-down and Double-flare.
Cleaning and Shaping
The title of the section Cleaning and Shaping, of course, looks a little unusual, since the article deals with the basics of root canal design. However, these two terms, which were introduced by endodontic luminary Professor Schilder 30 years ago, eloquently characterize both basic requirements for instrumental treatment of root canals: clean (clean) and shape (give the canal a shape).
Cleaning means the removal of all its contents from the root canal: infected tissues, antigenic material, all organic tissue residues, bacteria and their metabolic products, as well as the elimination of carious tissues and denticles or other hard tissue deposits; material infected with bacteria (contaminated) for filling root canals and other factors contributing to the occurrence of the inflammatory process. The term Cleaning means instrumental processing and mechanical removal of the contents of the root canal, as well as chemical dissolution of tissue residues and their leaching from the root canal.
The concept of Shaping implies giving the root canal a certain (special) shape. According to Schilder, five conditions must be met when carrying out this manipulation (see below). The Shape procedure, or root canal preparation, allows instruments intended for obturation of the root canal (for example, pluggers, spreaders, etc.) to freely penetrate the root canal and develop the force necessary for obturation. Due to this, it becomes possible, for example, to give the required shape to a root filling made of gutta-percha.
High-quality formation of gutta-percha, in turn, ideally ensures filling of the lateral tubules, branches of the root canal and various irregularities, i.e., it allows for three-dimensional filling of the entire root canal system. Shaping, as a mechanical component of root canal treatment, is carried out using the following tools, used according to certain rules:
- Gates-Glidden burs;
- burs designed to work at low rotation speeds;
- ultrasonic and sonic nozzles;
- hand-held endodontic instruments and, increasingly, nickel-titanium instruments with appropriate taper (e.g. Shaping files).
The first step in successful Cleaning and Shaping is to create an access cavity of sufficient size in the coronal area. Then it is important to obtain the necessary shape of the root canal in the apical region and in the middle third (Body Shape), as well as create the necessary taper (Taper) towards the apex of the tooth root.
There are different opinions regarding the need to pass through the apical foramen. Schilder defines this stage of root canal development as Foraminal Patency (passing the apical foramen) and believes that when instrumenting the root canal, it is necessary to pass the root canal slightly beyond the apical foramen using a thin K-file. As mentioned above, according to Schilder, when forming a root canal, five conditions must be met:
- Obtain a conical shape of the root canal that continuously increases from the apex to the coronal part.
- Maintain a very small root canal diameter in the apical direction, with a minimum diameter at the apical foramen.
- Divide the root canal (especially if it is curved) into several planes and prepare in these multiple planes.
- Never change the location of the apical foramen or move it to the side.
- When developing a root canal, try to maintain the smallest possible dimensions of the apical foramen.
It is to comply with the last condition according to Schilder in the apical region that it is enough to develop the canal to sizes 20 or 25, and sometimes 30. At the same time, unless absolutely necessary, the root canal should not be expanded in the area of apical narrowing (constriction). Of great importance for ensuring the success of treatment is the creation of a continuously increasing conical shape of the canal. In this case, it is necessary to begin root canal preparation from the coronal area and sufficiently irrigate the root canal.
In the coronal and middle third of the root canal there is a significant portion of infected and necrotic tissue. The root canal in this area should be treated first and also widened sufficiently. In order to promptly prevent possible blocking of the root canal, it is also necessary to repeatedly perform recapitulation (repeated passage of the canal to check its patency) using a file of the previous size. You can also carry out this manipulation each time using a K- or H-file of size 15.
Step-back technique (“step back”, step-by-step retreat, apical-coronal)
There are two methods for developing root canals: from the apical foramen to the coronal part (apical-coronal) and from the coronal part of the canal to the apical foramen (coronal-apical). When using the apical foramen to coronal root canal technique, the apical part of the root canal is first completely processed, and then the canal is widened and tapered.
When using this technique, an apical stop is created, and the shape of the root canal acquires a slightly increasing taper towards the coronal part. There are two variants of this method: standard technique and Step-back. When performing instrumental treatment of the root canal from crown to apex, all manipulations are carried out in the reverse order: first, the coronal part of the root canal is expanded, and only then its apical part is processed.
When using the Step-back technique, the apical part of the root canal is first treated, and then its coronal part is formed. Immediately after opening the tooth cavity, an x-ray is taken to measure the working length of the root canal. The first file that fits tightly into the canal to its full working length is called the initial apical file (IAF).
Then the root canal should be expanded by four sizes by processing all the walls of the canal with files in a circular manner. At this initial stage of work, you should not jump to a larger instrument size without skipping the previous one, as this may lead to blocking of the root canal. To improve the quality of root canal treatment, it is recommended to carry out frequent recapitulation using a file of the previous size. After treating the root canal with each subsequent size of instrument, it is also necessary to sufficiently treat the canal with an irrigation solution.
The final file that performs instrumentation of the root canal and removes only white dentin chips (i.e., the infected dentin is completely removed) is called the “apical master file” (AMF). Its size corresponds to the main gutta-percha point (master point) used in the future. The coronal part of the root canal is then tapered using the Step-back technique, and the root canal is expanded by four sizes (shaping).
In this case, the working length of K-files following the “apical master file” (AMF) sizes is set to 1 mm shorter for each subsequent size. Thus, the root canal takes on the shape of a cone with an increasing diameter towards the coronal part, as well as a fixed apical stop. Performing recapitulation with an apical master file (AMF) helps verify the patency of the root canal.
Comparative studies were carried out to determine the quality of cleaning and verify that the required shape of the root canal was obtained when using various tools for its processing: K-files, Hedstrom files and unifiles.
At the same time, it was found that even when treating the root canal with only K-files using the Step-back technique, very good apical development of the root canal was achieved without the formation of coves; An almost rounded shape of the root canal in cross section was obtained, and the canal also acquired the shape of a cone with a diameter increasing from the apex to the coronal part and a fixed apical stop. However, when treating curved root canals, in 46% of the studied cases there was a change in the original shape of the root canal after its development.
Treatment of straight root canals is carried out using rotational movements of the instrument in a clockwise direction, i.e. rotation to the right (reaming). But such instrumental processing is still not without risk. During rotational movements, the cutting edges of the instruments penetrate deep into the dentin, and the instrument can jam and get stuck in the canal. Both during the development of the root canal and when removing the instrument from the canal, its breakage may occur.
If the root canal is slightly curved, steps may form, leading to a loss of the working length of the root canal. When using K-files in combination with partial rotational movements, it is possible in 80% of cases to achieve a round cross-section of the root canal at a distance of 1 mm from the apical foramen. As the radius (angle) of curvature of the root canal increased, the probability of obtaining a rounded root canal in cross section decreased accordingly.
When the angle of curvature of the root canal is over 25 degrees. a round cross-sectional shape of the root canal was achieved only in 33% of cases. At the level of the apical third, it is possible to obtain a rounded cross-sectional shape of the root canal only when developing the canal with size 40 files.
Step-down technique (“step forward”, from the crown down, coronal-apical)
When using this method of root canal treatment, the coronal part of the root canal is first expanded and only then its apical part is developed. The technique is based on sequential work with tools from larger to smaller sizes. This method of root canal treatment has the following advantage compared to apical-coronal techniques: widening the root canal in the coronal region makes it possible to insert an irrigation needle to a sufficient depth into the root canal.
Thus, during instrumental processing of the apical part of the root canal, the dissolution of necrotic remains of pulp tissue is facilitated using a sodium hypochlorite solution. At the beginning of root canal treatment, the maximum length of its patency should be determined.
For these purposes, at the very beginning of root canal treatment, a file of size 15 is used, which must be rotated at 45 degrees. insert into the root canal with little force. Using partial rotational movements in combination with reciprocating movements of the file, the root canal is carefully expanded; at this stage of development, there is no fear of blocking the root canal.
The coronal portion of the root canal is then widened using Gates-Glidden burs until the root canal begins to curve. Using a size 1 (#50) Gates-Glidden bur at 500 rpm. the root canal expands to the point of curvature. In this case, the top of the instrument should first be coated with a lubricating gel (endolubricant). The working length of the Gates bur size 2 (#70) is set 1 mm shorter.
Accordingly, the working length of tools of sizes 3, 4 and 5 is set sequentially 1 mm shorter. By repeatedly irrigating the root canal with sodium hypochlorite solution, dentinal filings are washed out of the root canal. After widening the coronal part, a size 15 K-file is inserted into the root canal, with which a radiograph is taken to measure the working length. If the root canal is so narrow that it is not possible to insert a K-file into it to the working length, you should use a Hedström file to ensure patency of the root canal with careful movements.
Treatment of the apical part of the root canal is carried out alternately, first with Hedstrom files (reciprocating and scraping movements in a circular manner along the walls of the canal), and then with K-files (rotational movements) using the balanced-force technique. Thus, the coronal part of the root canal is expanded using a size 20 Hedström file, and finally the canal is processed using a pre-curved K-file size 20 to the full working length.
If the file cannot be inserted into the canal to the working length, then the instrument should not be inserted into the canal through forced rotational movements in the apical direction. In this case, it is necessary to recapitulate with a file of the previous size. By using the correct Patency file technique, blocking of the root canal or the formation of steps is almost eliminated, and the root canal curvature area can be better processed according to its shape.
In order to avoid the formation of a funnel-shaped expansion in the apical region, the instruments should first be curved in accordance with the curvature of the root canal. Preliminary bending should be carried out in the apical part of the instrument. Bending the instrument closer to the coronal part leads to an undesirable change in the shape of the root canal. Once the initial apical file (IAF) size is established, the root canal is enlarged four sizes to the size of the apical master file (in this case, size 35).
When using this technique, there is no penetration of bacteria from the infected coronal part of the root canal into the uninfected apical parts of the root canal, since infected tissue is removed from the coronal and middle parts of the root canal at the first stage of its treatment. Due to this, the incidence of pain after endodontic treatment is significantly lower than with the Step-back technique.
In addition, after treating the coronal part of the root canal with Gates burs, it becomes easier to focus on tactile sensations when working with endodontic instruments in the apical sections of the root canal. The irrigation needle can now penetrate deep into the root canal, and irrigation allows for better development of the root canal using hand instruments. It should also be noted that after preliminary expansion of the coronal part of the root canal, the likelihood of changing its shape when determining the working length decreases.
Double-flare technique (double expansion, double cone)
After opening the tooth cavity and extirpating the remaining pulp, a radiograph is first taken to measure the working length of the root canal. The Double-flare technique consists of three stages. First, the coronal part of the root canal is processed using the Step-down (reverse flaring) technique, then the apical part of the root canal is developed, and finally, a conical expansion of the root canal is carried out along the entire working length using the Step-back (flaring) technique.
The root canal orifice is an anatomically defined narrowing (coronal constriction). Timely elimination and expansion of this narrowing facilitates further stages of root canal treatment.
Such expansion can be carried out using the reverse flaring technique. In this case, manual files for further processing of the root canal in the apical region are used in the reverse order. Once the longest length of root canal patency has been established using a size 15 K-file, a size #45 file is inserted only a few millimeters into the coronal portion of the root canal, then a size 40 file is inserted deeper into the coronal portion of the canal, and using a size # 40 K-file 35, the coronal part of the root canal expands even deeper towards the apex.
After such expansion from the area of the root canal mouth to the middle of the canal length, a size 15 K-file is inserted into it again to the full working length to expand the root canal along its entire length. Then files of sizes 17, 20, 22, 25 and 27 are introduced into the channel. With this processing, two options are possible:
- In addition to files of standard sizes 15, 20 and 25, use files of intermediate sizes from the Golden Medium system (Maillefer).
- Make files of intermediate sizes yourself from standard files by successively shortening the tip of the tools by a millimeter. Since the cross-sectional diameter of a K-file with a 2% taper per millimeter of length increases by 0.02 mm from the tip of the tool to the shank, if the tip of the tool is cut in a certain way, it is possible to obtain a tool of intermediate size. After cutting off the top of the file, a sharp and uneven edge appears, which must be smoothed using a diamond-coated tool, and then the file must be sterilized again in a ball (Glasperlene) sterilizer.
After the final expansion of the apical part of the root canal to size 30, the working length of the file 35 in accordance with the Step-back technique is set to 1 mm shorter. Recapitulation is then carried out using the previous file size to the full working length of the root canal to prevent blockage of the root canal. The working length of a size 40 file is set to 2 mm shorter, a size 45 file is set to 3 mm shorter, and a size 50 file is set to 4 mm shorter. As a result of the use of this processing technique, the apical third of the root canal also acquires a conically widened, or flared, shape (flaring).
In addition to the method described above, expansion of the root canal in the coronal region can also be carried out using Hedstrom files or Gates-Glidden burs. You can also use shaping files from the ProTaper system.
When the root canal is enlarged in the apical region, the root canal should be treated for a sufficient period of time using small instruments. The following feature is characteristic of instruments standardized according to the ISO system. The increase in the cross-sectional diameter of a file of the next size relative to the file of the previous size is significantly higher for small-sized instruments than between large-sized files. For example, the cross-sectional diameter of a tool from size 10 to size 15 (0.15 mm at the tip of the tool) increases by 50%. The increase in tool cross-sectional diameter from size 30 to size 35 is only 16.7%.
In summary, the Double-flare technique can be characterized as follows: expansion of the coronal part of the root canal begins with a large instrument, then smaller instruments penetrate deeper into the root canal, and in the final stage the canal is processed from the apex to the coronal part using a small instrument. As a result, a double expansion of the root canal is obtained: in the apical and in the coronal part (double flaring). This method of root canal treatment is a combination of Step-down and Step-back techniques.
Rice. 5. The mouth of the root canal is first expanded using Gates burs, and then a carpet path is formed to the apical opening. Rice. 6. After determining the working length of the root canal, you can manually or using nickel-titanium files to expand the root canal to working dimensions. Rice. 7. Development of the root canal is controlled using an operating (dental) microscope with 10-20x magnification. Rice. 8. Monitoring the results of treatment using x-rays.
Article provided by the magazine ZWP - ZAHNARZT WIRTSCHAFT PRAXIS (Oemus Media AG, Leipzig, Deutschland, No. 7+8 / 2009, pp. 34-40).
Translation by Inna Bichegkueva.
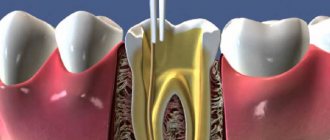
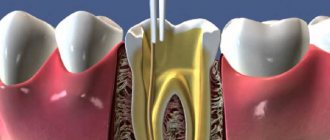
Where is the tooth canal located, how is it structured
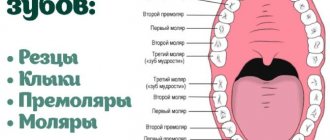
Human teeth have almost the same anatomical structure, including three main parts: crown, neck and root. Inside the tooth there is a pulp chamber, from which canals originate and extend all the way to the root. The pulp chamber contains the pulp or nerve of the tooth, which is a bundle of nerve fibers and blood vessels. Nerve fibers and vessels also pass through the entire internal space of the dental canal. The shape of the tooth canals can be either straight or curved, and their number varies depending on the type of tooth. Thus, the canines and incisors of the upper jaw have one canal, the canines and incisors of the lower jaw have two. There may be two or three canals in molars, and the maximum number of canals is observed in wisdom teeth - from three to five. The exact number of dental canals is determined using radiographic examination.
As mentioned above, the shape of the canals can have bends and turns, which complicates the process of their high-quality cleaning and treatment. Meanwhile, when treating canals, it is important to thoroughly clean their internal space - otherwise it will not be possible to stop the inflammatory process and save the diseased tooth.
Errors and complications associated with creating endodontic access
Insufficient removal of the arch of the dental cavity (Fig. 1).
Rice. 1. Insufficient removal of the arch of the tooth cavity
Causes:
- insufficient knowledge of the topographical features of the tooth cavity;
- non-compliance with the rules for opening the tooth cavity.
Prevention:
- knowledge of the topographical features of the tooth structure;
- following the algorithm for opening the tooth cavity.
Endodontic treatment begins with the complete removal of carious tissue and poor-quality restorations. The opening of the tooth cavity is carried out with a spherical diamond bur. To expand the cavity, it is better to use cylindrical burs or mechanical wellhead files. The most rational approaches to the dental cavity are considered coronal-apical and mesiodistal. They make it possible to minimize the number of errors at the initial stage of processing and not to lose the correct direction of the tool in the channel. To check the free access of the instrument into the canal, the “hanging” instrument rule is used: the instrument must enter in a straight line without bending at the mouth.
Perforation of the bottom or walls of the tooth cavity is one of the most common complications during mechanical treatment of the tooth cavity and root canals.
The problem of tooth perforation appeared with the introduction into practice of drills in 1871 and special instruments for mechanical expansion of root canals (Gates Glidden, Beutelrok, Drill reamer, etc.). Even then, there was an increase in the number of complications. The factors leading to the occurrence of perforations were pointed out by the dentist M. Morgenstern in 1901: if “... careless handling of root drills when using an electric drill, it is easy to drill the root.” Currently, dentists make the same mistakes as they did a hundred years ago.
Perforation of the bottom of the tooth cavity is caused by excessive preparation with a bur during the search for the mouths of the root canals. This happens especially often when re-treating a tooth previously treated with the resorcinol-formalin method, since the search for the mouths of the canals is complicated by the changed color and structure of the dentin of the bottom of the tooth cavity.
The prerequisites for the occurrence of perforations of the bottom and walls of the tooth cavity are:
- displacement of the tooth axis in the lingual or buccal direction;
- reduction in the height of the tooth crown due to significant abrasion of the chewing surface or deposition of a large amount of replacement dentin;
- endodontic treatment of a tooth through an artificial crown.
Clinically, perforations of the bottom or walls of the tooth manifest themselves in the form of a characteristic “sinking” of the instrument, bleeding and a sharp pain in the patient during treatment without anesthesia. Touching the site of a fresh perforation with a probe also causes acute pain.
Perforation of the tooth crown at the level of the neck, walls of the crown cavity, bottom of the crown cavity and in the bifurcation area (Fig. 2, 3):
Causes:
- poor knowledge of topographical features of teeth;
- rough preparation without taking into account the position of the tooth and its working length;
- excessive expansion of the root canal orifices, sometimes as a result of an attempt to detect the orifice of a sclerotic canal;
- incorrect choice of tool and violation of the methodology for its use;
- an attempt to prepare curved root canals.
Prevention:
- indication of root canal orifices using dyes;
- compliance with the principles of preparation taking into account the topography of the teeth;
- compliance with the rules for using endodontic instruments;
- knowledge of topographical features of teeth;
- avoiding forced passage of narrow and obliterated root canals and irrational use of machine instruments;
- periodic x-ray monitoring during the passage of root canals.
Rice.
2. Perforation of the tooth cavity Fig. 3. Perforation of the bottom of the tooth cavity. Fracture of the vestibular or lingual wall of the tooth.
Causes:
- wrong direction of bur;
- excessive pressure on the boron.
Prevention: careful use of a boron.
Indications for dental canal treatment
Tooth canal treatment is a specific dental procedure that is advisable to perform in the following clinical cases:
When an active inflammatory process is detected inside the root of a dental unit. The inflammatory process in this part of the tooth can lead to gradual tissue necrosis. If tissue necrosis begins, the diseased tooth will have to be removed.
The condition is diagnosed by radiography;
Treatment of tooth canals is required for pulpitis - inflammation affecting the pulp bundle;
Endodontic treatment is carried out for periodontitis, a disease affecting the apical part of the tooth root;
In some cases, cleaning and treatment of dental canals is required for advanced forms of caries.
Dental canal treatment is also indicated for abscesses, the onset of an inflammatory process under an old filling, or a fractured tooth root. The need for measures to treat tooth canals may be indicated by such symptoms as: severe, excruciating pain in the tooth, occurring mainly at night, swelling of soft tissues, discoloration of the gums and tooth enamel.
In some cases, tooth canal treatment is carried out before prosthetics. The nerve is removed from the tooth, and the canal cavities are cleaned, treated with antiseptic drugs and filled.
Results of a study of gels for chemical expansion of dental root canals
O. P. Krasnikova Ph.D., assistant at the Department of Clinical and Pediatric Dentistry of VSMA
E. A. Alferova Candidate of Medical Sciences, Assistant of the Department of Clinical and Pediatric Dentistry of VSMA
E. V. Vusataya Candidate of Medical Sciences, Assistant of the Department of Clinical and Pediatric Dentistry of VSMA
S. Yu. Khavantsev Assistant, Department of Clinical and Pediatric Dentistry, VSMA
A. V. Sushchenko Doctor of Medical Sciences, Professor, Head of the Department of Clinical and Pediatric Dentistry of VSMA
Today, endodontics has extensive information about the structure of the root canal system. It is known that the overwhelming majority of root canals have an irregular shape, different diameters in the buccolingual and mesiodistal directions, numerous lateral canals, anastomoses and isthmuses, the presence of a delta in the apical part, the formation of not one, but several apical foramina, etc.
In this regard, it becomes obvious that such a complex system is not possible to clean only mechanically [4]. It is known that one of the most important stages of endodontic treatment, which has a significant impact on its prognosis, is mechanical and medicinal treatment of the root canal system [1, 2, 5].
To facilitate the passage and expansion of narrow and obliterated root canals during instrumental treatment, complexons or so-called chelates with an affinity for alkaline earth metals are used. Expansion of the canal using chelates is based on their ability to form complex compounds with dentine calcium, as a result of which the latter goes into solution.
As a result of this reaction, the walls of the root canal are decalcified and softened, which facilitates the process of instrumental treatment of the root canal. Complexons are non-toxic, easy to use, do not require special storage conditions, and remain active for a long period of time [3].
The pre-marked instrument is lubricated with gel, inserted into the canal, and mechanical processing is carried out with the prepared file. Alternately, you should irrigate the root canal with a solution of sodium hypochlorite and perform mechanical treatment of the canal with a file lubricated with gel. During irrigation with sodium hypochlorite, foam will form, which will help remove the contents of the canal.
You cannot leave the gel in the canal until the next visit. Finally, it is necessary to thoroughly rinse with water and dry the canal with a liquid for drying and degreasing the root canals, after which you can begin filling.
Today, the dental market offers a wide range of EDTA-based products, which are produced in the form of gels, solutions, and liquids. We conducted a comparative analysis of agents for chemical expansion of root canals RC-prep (USA), Canal + (Septodont), Edetal (Omega) and Dilaton+ (Celite). In the experiment, such properties of the preparations as fluidity, the pH value of the gel, the ability to remove dentin particles, the foaming effect when adding sodium hypochlorite, etc. were studied (Table No. 1).
Table No. 1. Comparative analysis of gels for chemical expansion of root canals
| Indicators | Rc—prep(USA) | Canal+ (“Septodont”) | "Edetal" ("Omega") | "Dilaton+" ("Celite") |
| Package | Syringe without rubber piston, plastic bag, label, 1 pc., cannula (curved), no instructions | Syringe without rubber piston, box, label, instructions, 5 cannulas | Syringe with rubber piston, label, instructions, box | Syringe with rubber piston, label, instructions, box |
| Weight | 9 g | 5 g | 5 ml | 5 g |
| Appearance, consistency | Homogeneous viscous gel, opaque, white, well lubricates endodontic instruments | Homogeneous viscous gel, opaque, white, well lubricates endodontic instruments | Homogeneous thick gel, opaque, white | Homogeneous viscous gel, opaque, white, well lubricates endodontic instruments |
| Fluidity of 0.1 g gel, mm at a load of 2.5 kg | 32—34 | 28—30 | 25—26 | 34—35 |
| pH value of the gel | 6 | 6 | 6 | 6 |
| Floating agent content (ability to remove dentin particles), % | 11,5 | 5 | 5 | 5 |
| Foaming effect when adding sodium hypochlorite | Active foaming | Moderate foaming | Moderate foaming | Moderate foaming |
| Amount of main substance Trilon B, wt % | 17,5 | 15,5 | 14,5 | 15 |
| Water washability | + | + | + | + |
| Dissolution in water | Dissolves slowly, presence of undissolved sediment, cloudy solution | Dissolves quickly, presence of undissolved sediment, transparent solution | Dissolves slowly, the solution is transparent, there is no sediment | Dissolves quickly, the solution is transparent, there is no sediment |
All presented drugs demonstrated similar values. The study found that the highest content of floating agents that promote the removal of dentin particles was found in RC-prep (USA). In addition, a comparative study of the clinical effectiveness of the use of drugs RC-prep (USA), Canal + (Septodont), Edetal (Omega) and Dilaton+ (Celite) was conducted. Chemical expansion of 20 root canals of teeth in 15 patients was performed (5 canals per preparation).
To obtain comparable results, chemical expansion of the canals was carried out only on teeth of the lower jaw that had not previously been treated endodontically. The method of administration of the drugs was identical. Each of them was introduced into the root canal using a hand-held endodontic instrument, and mechanical expansion of the canal immediately began.
The procedure was repeated 3-5 times. At the end of the procedure, the tooth cavity was washed with water. The effectiveness of the intervention was assessed by the time spent on expanding the canal (Table No. 2).
Table No. 2.
| A drug | Average time spent on one root canal (min.) |
| RC-prep(USA) | 2,6 |
| "Dilaton+" ("Celite") | 3,4 |
| Canal+ (Septodont) | 4 |
| "Edetal" ("Omega") | 4,2 |
When using RC-prep (USA), all root canals were completed to the apical foramen within 1-5 minutes from the start of expansion, an average of 2.6 minutes. When using Canal + (Septodont), all root canals were completed to the apical foramen within 1-8 minutes from the start of expansion, an average of 4 minutes.
When using "Edetal" ("Omega"), all root canals were passed to the apical foramen within 1-9 minutes from the start of expansion, an average of 4.2 minutes. The time spent using the drug “Dilaton +” (“Celite”) ranged from 1 to 7 minutes, with an average of 3.4 minutes. It should be noted that when using all drugs, no side effects were observed in patients; no irritation of periapical tissues was observed in the immediate period after treatment (1-7 days).
Thus, our study indicates a higher efficiency of the drug RC-prep (USA), and, apparently, it should be given preference when choosing a gel for chemical expansion of the root canal. However, the cost of drugs must also be taken into account - when analyzing price categories, domestic drugs undoubtedly win. Therefore, when choosing a particular drug, a practicing dentist must take into account all the parameters.
- Cohen S., Burns R. Endodontics: Trans. from English - St. Petersburg, 2000.
- Krammer I., Schlepper H. Guide to endodontics. User of endodontic instruments. Per. with him. - M., 1999. - 96 p.
- Makeeva I.M., Pimenov A.B. Smear layer of the root canal and its removal Endodontics today. - 2002. - T.2, - No. 1-2. — P. 5-10.
- Pimenov A. B. Areas of root canals inaccessible for instrumentation // Endodontics today. - 2003. - T. 3, - No. 1-2. — P. 23-25.
- Poltavsky V. P. Intracanal medicine: Modern methods. - M.: Medical Information Agency, 2007. - 88 p.
- Information materials, "VladMiVa", "Omega-Dent", "Raduga-R", Septodont.
Main stages of root canal treatment
Treatment of tooth canals is a complex, specific process that includes several successive stages. Below we will consider all stages of the treatment process in detail.
Diagnostics
During the initial visit to the dentist, the doctor will conduct a thorough examination of the patient’s oral cavity and will also prescribe x-rays. An image of the tooth will allow you to assess the condition of the dental canals, see their number, determine the stage of development of the inflammatory process, and also select adequate treatment for a specific clinical case.
Anesthesia
To gain access to the canals of a tooth, the dentist will drill out the coronal part of the tooth to reach the pulp chamber, behind which the canals are located. Both the pulp and the canals are penetrated by nerve fibers and therefore the specialist’s actions can cause some discomfort to the patient. To relieve a person of discomfort, local anesthesia is performed before starting root canal treatment. The drug is selected individually for each patient.
Moisture insulation of the area of the diseased tooth
To prevent pathogenic microorganisms that may be contained in saliva from entering the internal space of the tooth, the area of the diseased tooth is first protected from moisture by covering with a special latex bandage - a rubber dam.
Reaming a tooth
To gain access to the dental canals, the doctor will drill the tooth, removing all tissue affected by caries. The access hole is made either on the chewing surface of the tooth (when treating molars) or on the inside (when treating incisors and canines). After drilling, the doctor will remove either the entire pulp bundle or only part of the tissue affected by the inflammatory process.
Treatment of dental canal cavities
For high-quality treatment of dental canals, a specialized tool is used - files. Before the cleaning process, it is important to obtain detailed information on the structure of the dental canals, as well as their length. To do this, a photograph of the diseased tooth is taken, and a special type of device is used - an apex locator. The dentist will use the files to clean the canal cavities, and then rinse them with an antiseptic solution and treat them with antibacterial agents. During cleaning and antiseptic treatment, the dentist will expand the cavity of the canals, clean and smooth their internal surfaces. Then the cavities of the dental canals are thoroughly dried with paper points.
Next, the doctor puts medicine into the canal cavity, places a temporary filling on the tooth and sends the patient home. After a few days, you should come back to the dentist to evaluate the results of the treatment. If the image shows that the inflammation has been stopped, the canals are filled.
Sealing
Gutta-percha pins are used to fill dental canals. It is important that the dental canal is sealed correctly and efficiently, otherwise a recurrence of inflammation is possible and the tooth cannot be saved. After filling the canals, the crown part of the tooth is restored with a photopolymer filling or orthopedic structures. It will be useful to know that mild pain in the tooth within 14 days after the procedure is considered normal by dentists. Taking painkillers prescribed by your doctor will help eliminate discomfort. However, if the pain does not go away, its character is sharp, and does not subside even after taking anesthetics, you should immediately contact the dentist!
When is root canal treatment necessary?
Treatment and filling of canals are stages of endodontic treatment. The doctor opens the tooth to treat the following diseases:
- deep caries - the last stage of the disease, characterized by extensive damage to dentin, accompanied by severe toothache that appears when chewing, pressing on the tooth, eating cold and hot foods and drinks;
- pulpitis - inflammation of the neurovascular bundles located in the tooth cavity, most often occurs against the background of advanced caries, characterized by paroxysmal pain, which intensifies when eating hot or cold food;
- periodontitis - inflammation of the apex or edge of the tooth root, develops due to damage to the connective tissue that holds the dental unit; symptoms of the disease are acute pain, swelling of the gums, swelling of the lip or cheek, as well as pathological mobility of the tooth.
The main reason for the development of these diseases is non-compliance with the rules of oral hygiene. If you brush your teeth twice a day and visit the dentist regularly, these problems can be avoided. Experts recommend undergoing a preventive examination every six months. In this case, the doctor will be able to detect caries at an early stage and promptly eliminate it, thereby preventing the development of pulpitis and other complications.
How long does root canal treatment take?
The duration of tooth canal treatment depends on the complexity and characteristics of the clinical case, as well as the number of canals that the specialist will have to treat. On average, the duration of the procedure can range from 20 minutes to 1.5 hours.
It is also worth considering that for high-quality root canal treatment, you will have to visit the dentist’s office several times.
Preparing canals for filling –
High-quality filling of root canals in the treatment of pulpitis and periodontitis is the key to the absence of complications. But in order to fill the root canals, they must first be prepared for this. Since the root canals are very narrow, preparation for filling will consist of widening the canals and extending them along their entire length to the apex of the root.
Let's imagine that there is a deep carious cavity on the chewing surface of the tooth, and the tooth pulp is inflamed.
Main stages (preparation for filling):
- Removal of all tissues affected by caries (Fig. 1b) - at the same time, healthy tooth tissues can be partially removed in order to create convenient access to the mouths of the root canals.
- Removal of dental pulp – pulp is removed from both the coronal part and the root canals.
- Determining the length of each root canal - each canal has its own length and depends on the length of the root and bends.
- Mechanical treatment of root canals (Fig. 1c) - it is necessary to use special tools to go through the root canals the entire length to the apex of the root, and then expand the diameter of the canals to the desired size.
If this is not done, it will not be possible to qualitatively seal the canal along its entire length, especially its far third at the apex of the root. Only after this can the doctor proceed to the next stage: - Filling canals with gutta-percha is the final stage of working with root canals. The quality of this stage directly depends, first of all, on the correct measurement of the length of the root canals and on the quality of their mechanical processing.
Is it painful to treat root canals?
Thanks to the use of modern anesthetics, root canal treatment has become a painless procedure. The patient may feel mild discomfort only during the injection of the anesthetic.
Therefore, there is no need to be afraid of root canal treatment; moreover, you must remember that you should never postpone the procedure due to fear of the dentist! Inflammation in a tooth that has progressed to a certain stage of development cannot be cured, which means that the diseased tooth will have to be removed and a prosthesis put in its place. In addition, more serious complications may occur.
Modern method of treating tooth canals: treatment of the canal cavity under a microscope
The quality of dental canal treatment depends on the correctness and accuracy of cleaning and processing of their internal space. This is a very painstaking work, since the channels themselves are quite narrow (no more than one millimeter), and in addition, they can have bends and turns. If a specialist makes a mistake when treating the canals and does not remove particles of the affected dentin, a relapse of the inflammatory process is guaranteed. The use of a special tool in treatment - a dental microscope - will help eliminate possible errors and inaccuracies in the treatment of dental canals.
Using a microscope, the dentist will perform a high-quality removal of all infected tissues, while preventing injury to healthy tooth tissues. The use of the device simplifies the process of cleaning and processing channels with significant lengths, anomalous structure,
with curvatures and branches. In addition, the use of a dental microscope during the treatment of tooth canals improves the quality of tooth restoration as a whole, and also contributes to the timely detection of hidden caries.
At our dental clinic “Uni Dent” in St. Petersburg, you can receive services for dental canal treatment under a microscope. The procedure is carried out by highly qualified doctors using modern instruments and materials, and therefore when you contact us, you can rest assured that the treatment result will be of high quality! Dentistry "Uni Dent" - come to us for a beautiful smile and painless dental treatment!
Stages of treatment
There are two approaches to root canal therapy: surgical and therapeutic.
Therapeutic treatment is aimed at complete or partial preservation of the pulp. It involves placing a medicinal composition containing antibiotics and other active components into the pulp chamber. The method is used only in the initial stages of inflammation; in other situations it will be ineffective.
Surgical treatment involves complete cleaning of the canals, their disinfection and filling. Consists of 4 stages:
- Diagnostics. The specialist conducts a direct examination of the patient and prescribes an X-ray examination. X-ray images allow you to clarify the severity and extent of inflammation and choose the optimal treatment method.
- Depulpation. The doctor performs local anesthesia; after anesthesia, the tooth cavity is opened and all inflamed tissue is removed. Next, the cavity is given a convenient shape, and it is disinfected by washing with special solutions.
- Filling. The canal cavity and pulp chamber are filled with filling materials. In modern dentistry, solid pins are used in combination with plastic or quickly hardening cements and polymers.
- Restoration. After the treatment procedures, the tooth is given its original shape, and all previously formed defects are eliminated. This is achieved by filling, or in difficult cases by installing a crown.
After completing the treatment procedures, you need to consolidate the results obtained. Recommended:
- Avoid eating cold/hot food for several days.
- Carefully monitor oral hygiene.
- Eliminate solid food for 1-2 days.
After endodontic treatment, pain and increased sensitivity of the tooth may persist for 2-5 days. This is a normal phenomenon and is associated with the body’s reaction to therapeutic intervention and adaptation to the filling material in the canals.