Causes of obliteration of tooth canals
The main and most common causes of tooth root obliteration are:
- injuries;
- chronic inflammatory processes;
- age-related changes;
- poor quality treatment;
- the presence of cancer associated with the proliferation of connective tissue.
There are also factors that increase the likelihood of root canal obliteration. These include:
- malocclusion;
- heredity (in particular with marble disease and Stanton-Capdepont syndrome);
- metabolic and endocrine system disorders;
- exposure to chemicals on teeth over a long period of time;
- decreased functionality or inactivity of the tooth during chewing.
Difficulties in root canal treatment
Author: Bobby Patel
Translation: Zvorykin Sergey
Denticles and calcifications
To locate the sclerosed canal orifices, the clinician must first visualize and evaluate the size of the pulp chamber on a two-dimensional radiographic film. You should begin preparation by mentally imagining a picture of their location and directing the bur to the expected location of the root canal mouths.
Before starting treatment, it is necessary to obtain a high-quality targeted x-ray so that you can imagine the depth to which the bur should be immersed (usually the distance from the occlusal surface to the bottom of the pulp chamber is approximately 6.5 mm). Teeth that have undergone a pronounced process of obliteration and with a small volume of the pulp chamber require special attention and caution during the preparation process. Preparation to reach the tooth cavity should be less diligent, as overzealous preparation can lead to iatrogenic perforation. Teeth that have been crowned also require appropriate assessment of the crown-root orientation to allow proper preparation to access the canals (see Figures 1, 2 and 3).
Figure 1. Clinical radiograph and photographs showing (a) preoperative radiograph showing the radiolucent area associated with the 36th tooth. The referring physician performed emergency pulp extirpation but had difficulty identifying the “calcified canals.” Intraoperative photographs obtained using a microscope show
Figure 1 (b) Intraoperative microscopic images show an intact pulp chamber.
Figure 1 (c, d) view after complete removal of the chamber roof and operation of ultrasonic tips to determine the internal anatomy with direct access to all four channels. The canals can be easily processed along their entire length.
Figure 1(d) (continued).
Figure 2. Clinical radiograph and photographs showing (a) preoperative radiograph showing an obliterated pulp chamber (black arrow). Tooth 16 with irreversible pulpitis and a history of cracking.
Figure 2 (b) Bitewing radiograph confirms the presence of a radiopaque mass in the coronal portion of the pulp chamber and is suggestive of denticles. The preparation depth can be measured before the access begins.
Figure 2 (c) After opening
Obliteration of root canals. Clinical case.
A patient contacted us. The orthopantomogram image clearly shows complete obliteration of the lumen of the root canal of the 21st tooth.
Fig. 1 Complete obliteration of the root canal of the 21st tooth on an orthopantomogram
Diagnosis was made using cone beam computed tomography (CBCT).
Rice. 2 Sagittal section of the area of the 21st tooth on a CBCT image
Taking into account the skeletal asymmetry of the lower jaw in the image, the main cause of obliteration of the root canal in this case can be assumed to be trauma.
Rice. 3 Axial section of the upper jaw area with obliteration of the root canal of tooth 21
Medical Internet conferences
Tooth perforation is the formation of a pathological communication between the internal cavities and canals of the tooth with the surrounding tissues.
The reasons for the development of this complication:
1. Insufficient opening of the tooth cavity;
2. Insufficient knowledge of the topography of the dental cavity;
3. Wrong choice of tool and violation of the methodology for its use;
4. Excessive expansion of the mouths;
5. Significant bends of the root canals.
Clinically, perforation of the bottom or walls of a tooth manifests itself in the form of a characteristic “sinking” of the instrument, bleeding and sharp pain in the patient in the case of treatment without anesthesia, and probing in the perforation area also causes acute pain. However, for a more accurate diagnosis of perforation, an apex locator and x-ray should be used. The best prognosis is observed in cases where the perforation is closed immediately, which minimizes trauma and infection of surrounding tissue. The most unfavorable localization of perforation is the area of root furcation. Almost any perforation in this area leads to destructive changes in the periodontium [1].
The main goal of endodontic treatment is to eliminate infection and restore the integrity of the body's tissue barriers against microbial invasion. Materials that come into contact with living tissues must be biocompatible. There are many materials available for closing perforations: amalgam, composites, and glass ionomer cements. The main negative properties of these materials are microleakage, toxicity, and sensitivity to moisture. The ProRoot MTA material does not have all these disadvantages.
This material was developed at Loma Linda University (USA, California) by Professor of the Department of Endodontics Mahmoud Torabinejad [2].
The ProRoot MTA (Mineral Trioxide Aggregate) system is a powder consisting of small hydrophilic particles that turn into a solid cement paste in the presence of water due to hydration of the powder in less than four hours.
Composition: 75% Portland cement, 20% bismuth oxide, 5% dehydrated calcium sulfate [3].
Indications for use of the material:
1. perforation of the root and bifurcation area;
2. vital amputation;
3. apexification;
4. retrograde filling of the root apex;
5. elimination of root resorption [4].
Method of using the ProRoot MTA system to restore root canal perforation:
1. Having applied a rubber dam, we clean the root canal of sawdust and half-life products;
2. Dry the root canal system with paper points and isolate the perforation site;
3. Obturate all canals located apically from the perforation;
4. Prepare the ProRoot MTA material in accordance with the attached instructions;
5. Using the supplied application probe, place the material in the defect area. We compact the material in the cavity;
6. We make sure that the material is placed correctly using an x-ray;
7. Place a moistened cotton swab into the cavity and fill the canal with temporary restoration material for at least 4 hours;
8. After 4 hours, or during the next appointment, we inspect the ProRoot MTA material. The material must be hard. If this is not the case, wash and repeat application;
9. When the material has hardened, we obturate the remaining part of the canals. ProRoot MTA should remain as a permanent part of the root canal filling [5, 6].
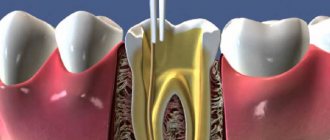
Treatment methods for root canal obliteration
Treatment of a tooth with root canal obliteration is quite difficult. Most often, in such cases, surgical removal of the part of the tooth affected by the pathological process is used, as well as chemical devitalization, in which tissue mummification is performed using special injections.
Treatment of root canal obliteration is a rather painful procedure, since due to the obstruction of the tooth patency, injection anesthesia is ineffective. The complexity of treatment causes the possibility of complications. These include perforation of the root canal and/or dental crown and possible pain due to incomplete elimination of canal obstruction.
Posted in Articles | Tags: 3-D CT, clinical case, CBCT
Search for the mouths of heavily sclerotic canals
Clinical case of endodontic treatment of upper incisors with heavily sclerotic canals. How to navigate a situation where there are “no mouths.”
Today I would like to share a clinical case that will demonstrate how a seemingly trivial situation can lead to serious complications, as well as how to avoid these complications.
The reference patient was referred by a colleague with a request to help carry out endodontic treatment before prosthetics in teeth 12 and 21. The doctor made an independent attempt at treatment, but unexpectedly the problem of severe obliteration of the orifices in both teeth was revealed, which did not allow the doctor to find the entrances to the root canals. The referring dentist only had binoculars in his arsenal, which, alas, did not allow him to confidently navigate inside the tooth.
This is how these teeth came to me. What do we see?
Firstly, we see that the doctor is great for realizing in time the risk of searching for the mouths “blindly”, without magnification. Since in both cases there were a couple of strokes of the tip left before the root wall was perforated.
Secondly, the search vector was shifted to the palatal side in both cases.
Thirdly, the obliteration really did not leave even a hint of the mouth where it should have already appeared. The situation in tooth 21 turned out to be especially difficult.
The green line shows the outline of the actual root canal. And here you can clearly see how the search for the mouth was carried out away from the true course of the root canal, threatening to end in perforation.
How to find the entrance to the canal when even the thinnest file (No. 6, No. 8) does not “catch” anything? It is necessary to remove sclerotic dentin. This can be done with a rotating instrument on a long stem or with an ultrasonic nozzle. But the main thing to remember is 2 important rules:
1. Any actions with aggressive instruments inside the tooth (canal) can ONLY be carried out under visual control. Ideally, under the control of armed vision, i.e. good lighting and magnification. We predictably can only do what we see with our eyes. If we work virtually, by touch, “by experience” - predictably, we can only do perforation, which will significantly worsen the future prospects of the tooth and the confidence of your patients.
2. Use practical laws of orientation in the pulp chamber when searching for orifices. One of the most important is the color of the fabrics...
This helps to understand where to “dig” to find the entrance. By removing a certain amount of sclerotic dentin under a microscope, we obtained a point that was barely noticeable at high magnification.
However, this turned out to be quite enough to make sure that this was the entrance to the root canal. Further work on processing and expanding channels in this situation was quite simple. The working length was determined using manual K-files No. 10, No. 15. Further instrumentation of the channels was carried out with the BioRaCe system to sizes No. 50.04.
Filling of the canal in the 12th tooth was carried out only in the apical third using hot gutta-percha (for subsequent restoration of the tooth using a pin structure). In 21 teeth, cold hydraulic obturation of gutta-percha with a bioceramic coating and a bioceramic sealer was used.
Progress of treatment of both teeth according to radiographs:
The patient was returned to the referring doctor for continued treatment and prosthetics.
Conclusions from this case, especially for young doctors:
- Inside the channels, do only what you see, do not work by touch!
- If you encounter a problem, stop on time! There is no need to be a hero if you do not have enough equipment, skills, or experience to cope with the situation. Refer the patient to more experienced and equipped colleagues, or at least warn the patient of the significant risk to him if he continues. This will be better for both of you and will save you from unnecessary conflict situations.
- use the rules of orientation in the pulp chamber! They are very effective, there are only a few of them, we talked about one of them today.
In subsequent articles and cases, I will tell you about other rules of orientation inside the tooth, which will help you not to make any mistakes. Stay tuned!
Endodontics under a microscope at Dentistry on Smolenskaya
Treatment of root canals of teeth under a microscope allows you to control the process of tooth treatment at any stage. Firstly, it is initially important to determine how many canals there are in the tooth so as not to miss any. High-precision expert equipment with ZOOM magnification at Dentistry on Smolenskaya gives a clear result, and the doctor can confidently say what condition the tooth tissue is in.
Secondly, during treatment under a microscope, any perforations of the root walls, violation of the integrity or incomplete filling of the canal are clearly visible. If the canals were initially sealed, a microscope will make it possible to qualitatively unseal the cavity. In addition, the microscope will help remove the remainder of a previously broken instrument, regardless of when it was broken off in the canal.
Dentistry on Smolenskaya employs doctors who are members of the expert community of the Russian Dental Association. Our specialists not only treat teeth, but also write books about trends in modern dentistry and its development. Attend symposia and conferences at the global and European level. They share their original developments in dental practice with colleagues.
Dental treatment should be trusted to professionals! At the Dentistry on Smolenskaya clinic, you are guaranteed to receive the best medical care, provided by doctors recognized for their services in the field of dentistry in Russia and in other countries of the world. To clarify prices for root canal treatment, please contact our specialists.