The working length of the root canal is the distance from the end point at the apex to the external landmark chosen by the doctor (tubercle, filling on the coronal part).
Doctors still cannot come to a consensus and say what should be taken as a guide: the physiological foramen (the transition of root cement into dentin), the apical foramen (the hole itself), the radiographic apex (the most distant point on the image) or the anatomical apex (the most distant area from the crown). The distance between them is up to 2 mm, and this is the difference between a well-sealed canal and the preservation of a source of infection.
The most important task is to find this end point, which is complicated due to the large number of different anatomical structures.
There are 4 methods for determining the working length of the root canal:
- x-ray
- tactile
- using an apex locator
- tabular
X-ray
The doctor determines the radiological apex from the image and the working length of the root canal is set 1 mm before it. The problem is that the channel is a three-dimensional structure, and the image is presented to us in a two-dimensional projection. There are cases when the doctor perforated the canal wall, while on the x-ray everything looks within normal limits. In almost 50% of all cases, the instrument is deeper than it appears in the photo.
Features of determining the working length of temporary teeth
If it is necessary to measure canals at the stage of active root formation in young patients, the specialist needs to take into account some nuances. For example, in this case, the X-ray method will be the most accurate. In this case, keeping the rudiments of permanent teeth intact is of great importance. For this purpose, doctors and dentists are advised to adhere to the following recommendations:
- Instrumental treatment of primary teeth should be carried out at a greater distance from the extreme radiographic line than in the case of treatment of permanent teeth.
- Even if there are signs of root resorption on the images, the size of the endodontic instruments should be 2-3 mm shorter than the radiographic length of the tooth.
- When processing canals, it is important not to reach the boundary line of about 2 mm, which will preserve the integrity of the root growth zone.
The correct choice of treatment method and competent calculation of the length of dental canals in children of different ages is a key factor in successful therapy and prevention of complications.
Tactile method
The least reliable option for determining the length of the root canal, the quality of such diagnostics depends on the doctor’s “insight” and his experience, which, you see, is an unacceptable argument. A thin instrument is inserted into the canal and the location of the hole is determined by touch. Another method is to use a paper point. Where it is saturated with blood or other contents is considered the exit point. If not a small part, but a significant area is saturated with blood, then it should be concluded that it has gone beyond the apex. This can also include pain. When the instrument goes beyond the top, the patient feels a prick, which is what the doctor focuses on.
The main stages on which the quality of root canal filling depends:
Determination of the working length of each root canal –
High-quality root canal treatment requires that the root canals be filled to the apex of the root. If you fill a tooth not to the top of the tooth root, then microflora begins to multiply in the lumen of the unsealed part of the canal. Its growth and extension beyond the root apex will lead to the destruction of bone tissue at the root apex and the development of purulent inflammation there.
The most common reason for unfilled tooth root canals is that the dentist initially determined their length incorrectly. Incorrect determination of the length of the canals leads to the fact that both mechanical treatment of the canals and their subsequent filling are carried out at the wrong depth.
If the channel length is determined incorrectly, then two options are possible:
- if the root canal is not filled properly, this will lead to inflammatory complications, the development of periodontitis, cysts and, in the absence of retreatment of the tooth, to its removal.
- If the root canal is refilled (the filling material is excessively extended beyond the apex of the root), this can lead to long-term pain, neuralgia, and the development of inflammation.
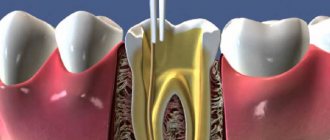
Therefore, it is necessary to carefully measure the length of each canal in the tooth. This is done in good clinics as follows: after removing the pulp from the root canals, the doctor, using special thin hand instruments (for example, K-files), tries to go through each root canal to the apex. Such a tool is schematically shown in the root canal in Fig. 4,9,10.
The advancement of the instrument deep into the canal is carried out under the control of a special Apex Locator device (Fig. 6), which is connected using an electrode to the K-file located in the canal (Fig. 5). The Apex Locator display shows the depth of the instrument's immersion, as well as the moment the instrument tip reaches the root apex.
The apex locator shows only an approximately accurate picture, therefore, according to the rules (immediately after measuring the length of the canals with the apex locator), it is necessary to take an X-ray of the tooth with K-files inserted into the root canals. These files are radio-opaque, so the X-ray can clearly see whether the tip of the instrument has reached the apex of the root.
Mechanical treatment of root canals –
The purpose of mechanical treatment is to expand the root canal and make it suitable for filling. In most cases, untreated canals are very narrow, have many imperceptible narrowings and expansions, which will not allow the canal to be properly filled with filling material along its entire length. Thus, mechanical treatment should remove all narrowings and irregularities throughout the root canal, and expand it to a certain size.
There are 2 methods of mechanical treatment of root canals:
- With hand instruments, the doctor rotates such instruments in the root canal with his fingertips.
- Using an endodontic tip, special titanium Pro-files are inserted into such tips (Fig. 12). Endodontic tips rotate the Pro-files in the root canal, and the Pro-files, with their sharp edges, gradually remove chips from the walls of the canal, expanding it.

Everything important about pulpitis What is pulpitis. Types of pulpitis. Treatment. Read more about the disease at uniksperm.u There are contraindications. Consult your doctor. Sensitive gums? Parodontax can help! 70% active ingredients for healthy gums Am I at risk · Gum care Causes of periodontitis · Frequently asked questions unikspperiodontal diseaseserm.ru
The advantages of processing canals with such machine Pro-files over hand tools:
- The quality of canal treatment is many times higher - the surface of the canal after such treatment is smooth, as if polished, and this facilitates the insertion of gutta-percha pins for filling the canal.
- Safety - the endodontic handpiece comes complete with a smart micromotor that controls the movement of the file in the canal, and if a certain load is exceeded, which threatens to break the Pro-file in the canal, the micromotor stops the rotation of the Pro-file and turns on auto-reverse.
Therefore, the threat of the tool tip breaking off in this case is minimal, which cannot be said about manual files. After all, the doctor’s fingers, with which he rotates the “manual” file, feel the resistance to the movement of the instrument quite weakly, and therefore very often this ends in the instrument breaking off and the impossibility of filling the tooth canal properly. As a result, inflammatory complications arise, which very often end in the removal of such a tooth.If your clinic performs mechanical treatment of canals using such smart devices, this is a big plus (by the way, such treatment costs more). However, it is worth remembering that in any case such treatment is performed by a doctor, and even the smartest and best device in the wrong hands can cause more harm than good.
Apex locator
The electronic method is considered the most reliable of all mentioned. The most popular brands of devices are: Russian Geosoft (EndoEst), Japanese NSK (iPex), German VDW (Raypex).
Determination of the working length of the root canal:
- one wire with a hook at the end is hung on the patient’s lip
- diagnostic tool (for example, K-file) is installed in the holder
- then the doctor slowly moves it along the canal; numbers are displayed on the device screen indicating how much is left to the top. An intermittent beep will also sound. Some models have a graphic display: green - far, yellow - close, red - in place
- When the instrument reaches its destination, APEX will appear on the screen and the alarm will beep continuously.
X-ray determination of working length
The most popular and in demand method for determining the depth of dental canals in children is radiography. This method can be used if the root system is well visualized on preoperative photographs and there is free access to it. This method also requires information about the average length and location of the canals of a particular patient, which can be obtained during the treatment of other teeth. The radiographic method usually requires the absence of complex bevels and thinned enamel on the crown, which will ensure ease of tooth preparation and reliable fixation of the stop at different depths. Also, the doctor should have the opportunity to use diagnostic files or reamers of size 15-20 or larger, which will not be able to extend beyond the apical foramen, but will be clearly visible on the images. The correct placement of the film and the direction of the beam are of great importance.
The process of determining the working length of a child’s tooth using this method is performed as follows:
- The size of the canal is measured using preoperative photographs.
- 1 mm is subtracted from the obtained value.
- A limiter is installed on the diagnostic tool according to the known length.
- The instrument is inserted into the dental canal, after which an x-ray is taken.
- The image is used to measure the distance between the tips of the tooth and the instrument.
- The resulting value and the length of the tool are summed up.
- Subtract 1 mm from the resulting figure.
- A limiter is installed on the tool according to the new length value.
- A repeat X-ray is performed.
- If necessary, another measurement and calculation of the tooth length is performed.
Table method
Over a long period of clinical observations, doctors have accumulated an extensive database on the working length of root canals. So, if there are no other options, you can take a conventional cutter and check the readings in the table. If there is no apex locator and x-ray, then this method should be supplemented with tactile. However, the anatomy of each person is individual, so the reliability of the table values is also not high.
So what is the most effective method for determining the working length of a root canal?
Alas, there is no one ideal technique. At the moment, it is customary to rely on the “apex locator + x-ray” combination.
Step Down Technology
The essence of this technique is to form a cone-shaped working tubule. This shape allows you to conveniently work with apical constriction and efficiently fill gaps.
Processing stages
- Determination of the working length of the tubule. To do this, the patient needs to take an x-ray of the tooth. From this image, the doctor determines how many root canals are in the tooth, how they are located and what their length is.
- Expansion of the mouth. The orifice is expanded using a set of K-files. First, the doctor works with K-files No. 8 and No. 10, depending on the extent of the damage. They pass almost the entire depression, not reaching approximately 0.4 - 0.5 cm to its end or to the place where it bends. To widen the canal, the dentist uses H-files or K-files. First he works with the thinnest tool, gradually changing it to a thicker one. Usually the following files are used: No. 15, then No. 20, No. 25, No. 30 and so on. As processing progresses, the canal increases in diameter, becoming more passable. The expansion does not reach the apical foramen by about 0.5 cm. After manual processing, the doctor proceeds to use a drill and uses Gates Glidden burs to form the orifice. At the same time, he also starts work with a small tool, moving on to a larger one.
- Establishing the working length of the recess. First, the doctor passes the pathfinder or K-reamer along the entire canal, and then sends the patient for a repeat x-ray to see the length and width of the treated cavity in the image.
- Cleaning the apical zone. It is carried out using the Step-back technique. Work begins with a large tool, gradually reaching the smallest one - No. 25. At the bottom, the recess takes on a cone-shaped shape, it has an apical stop in the area of the natural apex
- If the treatment proceeds easily, then it is advisable for the doctor to avoid filing movements. In this case, it is necessary to repeatedly advance the main apical file until the lumen is complete. This will avoid clogging. A smooth transition between the inner and intermediate parts of the tubule will make it passable and facilitate filling and penetration of filling material into all recesses. It is very important to seal the canal tightly, leaving no gaps. Otherwise, an infection may develop in it, and the procedure will have to be repeated.
Titanium-nickel profiles allow you to create a smooth intra-canal surface
This method can effectively clean and expand the root canals. For work, nickel-titanium profiles are used, which help to form a smooth intra-canal surface without notches or sharp transitions. These profiles are durable and chemical resistant.
One of the advantages of the method is that the waste material is immediately removed and does not fall deep into the tubule. This reduces the risk of infection to a minimum.