A. Zorian , Candidate of Medical Sciences, Department of Hospital Therapeutic Dentistry, Moscow State Medical University
A. Hovsepyan , director of dental clinical training, dentist V. Chilikin , associate professor, candidate of medical sciences, Honored Doctor of the Russian Federation, Department of Hospital Therapeutic Dentistry of Moscow State Medical University
The success of endodontic treatment is largely determined by the quality of root canal filling. High-quality filling today means three-dimensional sealing of the entire branched root canal system, which plays the role of a reliable barrier between the tooth cavity and periodontal tissues.
Over the long history of endodontics, various techniques and materials have been used to fill the root canal.
Until recently, the main method of filling root canals in Russia was the method of filling with one paste. At the same time, pastes based on zinc oxide and eugenol, as well as preparations containing resorcinol and formaldehyde, were very popular. The technique of filling a root canal with paste is quite simple and does not require significant time and material costs. However, filling canals with one paste has a number of significant disadvantages: 1. With this technique, only the main canal is filled with the material, and numerous branches of the root canal system remain open. 2. Very often the paste is discharged beyond the root apex, since there is no adequate control over the filling of the root canal with material. 3. The paste fills the root canal unevenly, leaving voids and not providing adequate sealing. 4. All pastes shrink and dissolve upon contact with tissue fluid. 5. Most pastes have an irritating effect on the periodontium.
Considering all of the above, it is not surprising that the International Dental Association and the American Dental Association do not recommend the use of the root canal obturation technique with one paste.
Endodontic materials
An ideal root canal filling material must meet the following parameters: 1. Provide a reliable seal throughout the entire root canal system. 2. Be non-toxic and have good biocompatibility. 3. Do not irritate the periodontium. 4. Do not shrink in the canal. It is desirable that it expands slightly when introduced into the canal or during the curing process. 5. Have a bacteriostatic effect or at least not support the growth of bacteria. 6. Easy to sterilize before use. 7. Be radiopaque. 8. Do not change the color of the tooth. 9. If necessary, it can be easily removed from the canal. 10. Have a curing time sufficient for comfortable work. 11. Do not dissolve in tissue fluid. 12. Have good adhesion to dentin and filling material.
Such an ideal material does not exist today. However, these requirements are best met by the methods of filling root canals with gutta-percha and sealer. The vast majority of root canals around the world today are filled using gutta-percha.
Preparation for filling
Before filling the canals with filling material, the doctor must thoroughly clean them and prepare the cavity in a special way. This process takes place in several stages:
- Removal of affected tissue
Most often, the need for root canal treatment arises as a consequence of another pathological process, in particular caries. To destroy the source of infection and open access to the mouths of the canals, the dentist removes dead and diseased tissue using a bur. - removal
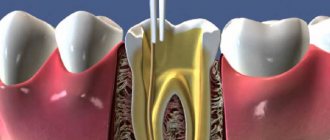
Pulp is the sensitive tissue of the tooth, a plexus of blood vessels and nerves located in the coronal part and inside the roots. The method of filling root canals involves removing the pulp using a special tool. Most often, this procedure, like the previous one, is performed under local anesthesia to eliminate pain and discomfort when removing the pulp. - Measuring canals
In order to perform a quality filling, the doctor needs to obtain as accurate information as possible about the properties and current condition of the canals. For this purpose, before treatment, as a rule, a targeted radiograph is performed. An important procedure is also measuring the length of the channels. The length is individual and depends not only on the size of the root, but also on the degree of curvature of the canal. - Mechanical processing
Before filling, the channels are cleaned and expanded using special tools. This is necessary to completely remove the affected tissue, as well as to more densely and evenly fill the canal cavity with filling material. Mechanical processing is performed using special thin tools - files. With the help of a file, the canal is passed completely, from the mouth to the apex.
Only after completing all the preparatory steps can the doctor proceed to filling.
Filling root canals with gutta-percha
Gutta-percha is a hard, but at the same time elastic and flexible coagulation product of the latex of tropical gutta-percha plants. Gutta-percha is divided into two types - alpha and beta - which differ greatly in physical properties.
For the production of gutta-percha points, beta-gutta-percha is traditionally used, which has greater hardness and spatial stability and less stickiness. Beta gutta percha requires higher temperatures to soften. However, recently, more fluid and sticky alpha gutta-percha has become increasingly popular, providing, when used in a heated state, a more homogeneous filling of the entire branched root canal system.
Alpha gutta-percha is used for techniques that involve working with thermoplasticized (heated) gutta-percha: vertical condensation and thermoplastic injection techniques. In addition, there is a special type of gutta-percha used to produce Thermafil obturators. This patented type of gutta-percha is similar in chemical properties to beta-gutta-percha, but at the same time has the physical characteristics of alpha-gutta-percha.
The production of gutta-percha points is mainly concentrated in Southeast Asia. One of the largest suppliers of gutta-percha is Korea. However, recently gutta-percha points have begun to be produced in Brazil.
Pins are divided into standard pins, which have a 2% taper and ISO sizes from 10 to 140, and tapered pins, which have a 2% to 12% taper and sizes from 20 to 30.
Gutta-percha points are made either manually (“hand-rolled”) or by machine. It is believed that the manual method provides higher precision in making pins. Machine-made pins often do not guarantee accurate calibration. It should be especially noted that all pins made in Brazil are machine-made.
The commercial name “gutta-percha pins” has taken root well and is used everywhere, although the content of gutta-percha itself in these pins is about 20%. The main component of the pins (60-70%) is zinc oxide. The remaining 10% consists of barium sulfate, wax, dyes and other additives.
The main advantage of gutta-percha is the predictability of root canal obturation. Its advantages also include good biocompatibility and low toxicity, the ability to condense, ensuring dense and uniform filling of the root canal, softening when heated, which allows for three-dimensional obturation of the root canal system, spatial stability (in the hardened state it practically does not change its volume) and ease of its removal from the root canal if re-treatment is necessary.
Despite all the obvious advantages, gutta-percha also has a number of disadvantages associated with the peculiarities of its physical and chemical properties and the technology of application. The disadvantages of gutta-percha are as follows: 1. It cannot be used without a sealer, since it does not have adhesion to dentin. 2. Gutta-percha does not have a bactericidal or bacteriostatic effect. 3. Thin pins have very high flexibility and softness, which requires high qualifications and experience of the doctor, especially when filling narrow canals, and can also lead to deformation of the pins during their fitting. 4. Thermoplasticized gutta-percha shrinks when cooled. To compensate for this shrinkage, it is necessary to continue the condensation process until it cools.
Injection methods, Ultrafil, Thermafil
Recently, the method of introducing heated (liquid) gutta-percha using special syringe systems directly into the canal (Obtura system) has also begun to be used. In this case, gutta-percha, heated to a temperature of 160-200 ° C (!), is introduced directly into the root canal using a special injection needle (cannula) of sizes 40 and 60 according to ISO standards.
With this method of canal filling, there is no need to use a sealer. However, the high temperatures used can, in direct contact with tissues, lead to burn damage to surrounding tissues (at the root apex?).
The dentist also has some other systems at his disposal, in which only slightly heated gutta-percha is used, rather than heated to a molten state (Ultrafil, Thermafil). With this method of application, gutta-percha softens a little, after which it is very easy to apply it to those parts of the root canal of the tooth that are not round in cross section.
Thermafil and Thermafil-Plus systems are widely used. This method uses plastic pins coated with gutta-percha. Pin sizes are standardized according to ISO standards. Such a pin is heated for a short time in a small electric oven and, during a short plastic phase, the heated gutta-percha is inserted into the root canal. The protruding excess pin is cut off. But even with this method, accidental pushing of heated gutta-percha into the apical region is possible.
The method of filling root canals using the Thermafil system is quite economical, therefore, in some dental offices aimed at a certain social contingent, patients do not need to pay an additional amount: the treatment is carried out within the framework of state health insurance.
Charging additional fees for endodontic treatment as part of “cash” services from patients insured by public health insurance funds can sometimes be quite problematic. So, unfortunately, the question once again arises: are innovations like the Thermafil system applicable in everyday dental care, if this is associated with even minor additional costs?
The “Central Pin Technique” and Thermafil or Ultrafil systems are economical, effective and realistically applicable in the provision of services within the framework of public health insurance. A dental office that primarily serves patients under public health insurance is faced with a difficult dilemma. And in such a situation, it is the Thermafil system that could find its application within the framework of “generally available endodontic treatment”. However, the question of whether with this method it is necessary to additionally use sealers or whether heated gutta-percha ensures sufficient tightness of the root filling is still being discussed. Saving time does not always benefit the patient.
In dental offices, mainly serving patients under public health insurance, the most often used, described in detail at the beginning of the article, is the very economical “central pin method” in combination with two-component paste sealers.
The author came to these conclusions after numerous discussions on this issue with colleagues during numerous master classes and meetings of quality control groups.
As mentioned above, this standard method of root canal obturation, if necessary, can be easily modified by using additional gutta-percha pins of the “lateral condensation” type, for example in the distal root canals of molars that are very wide or do not have a round cross-section, as well as for filling “large caliber” root canals in incisors and canines.
The author successfully uses the central pin method, as well as the method of “partial” lateral condensation, in his practice and has obtained good treatment results when filling root canals within the framework of state health insurance services (more than 4000 root fillings).
The author uses AH Plus sealer to fill root canals. The only question that remains is which of the many described methods can be considered standard for endodontic treatment within the framework of public health insurance.
The author is convinced that such a method could be the “central pin technique” in combination with a two-component sealer (containing calcium hydroxide), as well as the use of Thermafil or Ultrafil systems. These methods are economical, effective and therefore really applicable in the provision of services within the framework of public health insurance.
This topic should be discussed in professional circles in order to resolve the question of how endodontic treatment can be included in the list of services provided under public health insurance. And it is possible that, based on methods confirmed by evidence-based medicine, such endodontic treatment can be carried out at a much higher quality level. This is certainly doable.
Sealers for root canal obturation
It should be noted that the need to use a sealer is a relative disadvantage, since there is currently no material that can provide predictable filling of the main channel, and at the same time be fluid enough to fill all its branches.
The sealer acts not only as a sealant that fills all branches of the root canal system and ensures adhesion of gutta-percha to the canal walls, but also as a lubricant that ensures free sliding of gutta-percha pins in the root canal.
The sealer must meet the following requirements: 1. After mixing, it must have a sticky consistency in order to ensure good adhesion to the canal walls after curing. 2. Seal the canal hermetically. 3. Be radiopaque. 4. Do not shrink during the curing process. 5. Do not stain tooth tissue. 6. Have a bacteriostatic effect or at least not support the growth of microorganisms. 7. Harden slowly. 8. Do not dissolve in tissue fluids. 9. Do not irritate periapical tissues. 10. Dissolve in standard solvents if it is necessary to unseal the canal. 11. Do not cause immune reactions in periapical tissues. 12. Do not have a mutagenic or carcinogenic effect.
None of the sealers presented on the modern market can meet all the requirements placed on it. Basically, either natural root cements or polymeric materials are used as sealers today. Natural sealers – Endomethasone (Septodont), Cortisomol (Pierre Rolland), Tubli-seal (Kerr), etc. – which are based on zinc oxide, dissolve in tissue fluid, which can lead to disruption of the tightness of the root canal system. In addition, they have low adhesion to dentin and can cause staining of tooth tissue. At the same time, polymer sealers - AH Plus (Dentsply), Adseal (META Biomed), etc. - are less soluble in tissue fluid, do not stain tooth tissue and have better adhesion to root dentin.
Until now, the question to what level to fill the root canal remains open. There is intense debate as to whether gutta-percha should not reach the anatomical apex by 0.5 mm or stop directly at it. Today, the only indisputable fact is that the less we expand the apical narrowing, the better the quality of obturation, the more reliable the isolation of periodontal tissues. In addition, it must be remembered that the theory of active apical therapy has shown its inconsistency. In modern endodontics, removal of sealer beyond the root apex is not encouraged, even in the presence of inflammatory processes in the periodontium, although studies have shown that when a small amount of sealer is removed into the periapical tissue, no serious complications are observed after treatment.
***
There are various methods for filling root canals with gutta-percha: the single (central) pin method, lateral condensation, thermomechanical condensation, filling the root canal with chemically softened cold gutta-percha, intracanal hot vertical condensation, thermoplastic injection technique and the use of thermophiles.
Possible complications
After canal filling, complications may develop. In practice, the following cases are often recorded:
- perforation of the root wall. This complication is characterized by severe pain and bleeding;
- infectious damage caused by insufficient treatment;
- development of infection in the tooth, which is the result of incomplete filling of the canal;
- exit of the filling material beyond the root apex. Manifested by intense pain and severe sensitivity;
- response to channel temperature changes;
- pain due to instrument breakage during treatment;
- development of a cyst or granuloma;
- periodic inflammatory processes;
- change in tooth shade due to improper treatment;
- inflammation of the supporting tooth;
- loss of filling;
- development of an allergic reaction.
The likelihood of developing complications depends on the actions of the doctor and the patient. Therefore, when choosing a dental clinic, it is recommended to study reviews and select highly qualified specialists. But there are a number of rules for the patient that will help reduce complications after treatment to a minimum:
- See a doctor if pain and discomfort develops;
- consult a doctor if an allergic reaction develops;
- urgently consult a doctor in case of acute pain, severe swelling, fever;
- follow the doctor's recommendations;
- do not self-medicate.
Remember, self-medication is fraught with the development of serious complications! If you experience severe discomfort, contact your doctor! Modern filling materials in the hands of a qualified specialist minimize the likelihood of developing any complications.
There are contraindications. Specialist consultation is required.
Filling root canals with cold gutta-percha
Single pin method
This method consists in the fact that after appropriate treatment of the canal, which means giving it a taper of 4, 6 or 8%, a sealer is applied to its walls using a paper point. After this, a pre-selected pin with an appropriate taper and tip size is inserted into the canal. The pin should fit snugly against the canal walls. Some authors recommend shortening the tip of the pin by 0.5 mm. Using a heated tool, the pin is cut at the level of the mouth and its condensation is carried out in the vertical direction.
This technique can be a good alternative for doctors who prefer to fill canals with monopaste, but this only ensures filling the lumen of the main canal, and not three-dimensional obturation of the entire root canal system.
Features of temporary filling with pastes
In the case of a specific degree of development of the disease, the techniques for temporary filling of root canals may differ. This is justified by the peculiarity of the technique used during treatment. In acute forms of the disease, potassium hydroxide is injected into the canal, often without compaction and for a period of 1 to 7 days based on the clinical picture.
The main goal of the procedure is to prevent the appearance of inflammatory processes and harmful microorganisms inside the canal. In case of chronic diseases, the drug is most often administered with compactions for a period of up to 2 months. If necessary, the material used can be periodically replaced until the desired result is achieved. Based on general practice, treatment can last from six months to 1 year, depending on the extent of the disease, as well as the characteristics of the individual patient’s body.
The application of a temporary filling is also aimed at stimulating the processes of regeneration of damaged cells. To do this, the following filling techniques are used:
- the canal is cleaned and prepared, after which paste is placed in it for a period of 7 to 10 days;
- at the end of the period, the old layer of paste is removed and replaced with a new one;
- After a certain time, the manipulations are repeated (the exact timing is announced by the dentist).
To provide a clear picture of the treatment, an x-ray is taken. It must be performed no earlier than 3 months from the date of the patient’s first visit. The fact is that in the first stages of treatment the result can be variable.
X-ray of teeth
At the end of all procedures, restoration of damaged tissue takes about 3-5 years. During this period, it is recommended to follow all the doctor’s recommendations so as not to repeat the next development of the disease.
Modern Moscow dentistry uses potassium hydroxide-based preparations with various antiseptic additives.
Method of lateral condensation of cold gutta-percha
This scheme involves filling with gutta-percha pins with lateral pressing of each of the pins against the canal walls. For a long time, this technique was the “gold standard” with which all other canal obturation techniques were compared.
After drying the root canal using paper points, its walls are coated with sealer. Then a master pin selected to size is inserted into the canal, the tip of which is moistened in the same sealant. A spreader is then used to condense the master pin against the canal walls, providing sufficient space for the insertion of additional pins. The density of canal obturation depends on the depth of penetration and the shape of the spreader. According to Chohayeb (1993), ISO-standardized hand spreaders should be inserted into the root canal up to 1 mm from the tip of the gutta-percha point, which improves the homogeneity and density of the filling. After the master pin condenses, additional pins are condensed to it and the channel walls, the tips of which are also wetted in the sealant. Each subsequent pin enters the canal to a shallower depth. Lateral compaction of the pins is carried out until the canal is homogeneously filled, the criterion for which is the impossibility of inserting the spreader into the canal. The recommended time for pressing the pins against the canal walls with a spreader, according to various authors, is 15–30 seconds. After this, the protruding ends of the gutta-percha pins are cut off using a heated instrument, and the mouth of the canal is closed by vertical condensation of gutta-percha.
The quality of root canal obturation during lateral condensation of cold gutta-percha is influenced by many factors. First of all, this is the shape of the processed channel. The root canal must have a uniform taper along its entire length and an apical ledge that prevents material from being removed beyond the apex during condensation. The ratio of gutta-percha to sealer is also of great importance. The following ratio is recommended: 95% gutta-percha, 5% sealer.
Long-term use of the lateral condensation technique of gutta-percha has shown its high clinical effectiveness, ease of use and reliability. Many researchers point to the high filling density of the root canal when performing lateral condensation. However, other authors demonstrate that when performing lateral condensation, there is a risk of longitudinal root fracture due to the forces applied, especially when the root is weakened (for example, when the canals in thin roots are over-expanded). In addition, with this technique it is not possible to achieve homogeneity of the material and filling the lateral and apical branches of the canal with gutta-percha, which can lead to the development of complications from periodontal tissues - the development (or maintenance) of an inflammatory reaction, destruction of bone tissue.
It should be added that when working with cold gutta-percha, in order to adequately seal the mouth of the root canal, it is advisable to use a heated instrument to cut off the pins 2-3 mm deeper than the mouth of the canal and fill the remaining part with heated gutta-percha by injecting it.
In order to improve technologies for filling root canals with cold gutta-percha, various techniques have been proposed, which are currently of interest mainly only from the point of view of the history of the development of endodontics. Such techniques include thermomechanical condensation and filling with chemically softened cold gutta-percha.
Sealers
Pastes for filling root canals are usually self-hardening. They consist of two mixing components and have different chemical compositions.
The dental materials market offers a large number of sealers of the most varied composition from various competing manufacturers. Below the author provides a list of sealers currently used, and also mentions some materials that are no longer used.
Table No. 1. Sealers currently available on the market and their composition (in alphabetical order).
| 1. Acroseal (Septodont) | epoxy resin matrix containing calcium hydroxide |
| 2. AH 26, two versions (Dentsply) | matrix based on epoxy resin; composition options: with and without silver additives |
| 3. AH plus/AH plus Jet (Dentsply) | based on epoxy-amine polymers (AH plus Jet: automatic mixing system) |
| 4. Apexit Plus (Ivoclar Vivadent) | contains calcium hydroxide (base?) |
| 5. Endomethasone N (Septodont) | based on zinc oxide eugenol, currently free of formaldehyde |
| 6. Gangraena-Merz N (Merz Dental) | calcium hydroxide-based material that can be used for both temporary and permanent filling of root canals |
| 7. Hermetic (lege artis) | cement based on zinc oxide-eugenol for permanent filling of root canals |
| 8. Ledermix MTA | MTA cement for endodontic treatment of perforations or retrograde filling of root canals, as well as for apexification in the treatment of teeth with incomplete root formation |
| 9. N2 Endodontic Cement (Hager & Werken) | based on zinc oxide eugenol, with a reduced (!) formaldehyde content compared to the previous version of the composition (but still contains formaldehyde) |
| 10. Perma Evolution (Becht) | polymer based on epoxy resins |
| 11. RealSeal (Sybron Endo / Kerr) | thermoplastic synthetic polymer with bioactive (?) and radiopaque glass fillers |
| 12. rocanal r2 permanent vital (la Maison Dentaire) | cement based on zinc oxide-eugenol for permanent filling of root canals after vital pulp extirpation |
| 13. rocanal r3 permanent gangrene (la Maison Dentaire) | cement based on zinc oxide eugenol for permanent filling of root canals after treatment of gangrenous pulpitis, contains 5% orthophenylphenol (!) and 0.5% nitrofurazone (?) |
| 14. Sealapex (Sybron Endo / Kerr) | polymer, contains calcium hydroxide |
| 15. 2Seal (VDW) | based on epoxy-amine resin |
| 16. GuttaFlow (Roeko) | system for filling canals with cold gutta-percha in combination with a central gutta-percha pin (Master-Point) |
| 17. RoekoSeal (roeko company) | based on polymethylsiloxane (silicone), expands slightly during curing (0.2%) |
The list, for example, mentions material N 2 (, Sargenti), containing toxic formaldehyde. Currently, the material is no longer used in Germany. The list also includes the still widely popular material Endomethasone N (Septodont). Currently, the composition of the material has been slightly changed compared to the previously used original Endomethasone material. In the Endomethasone N material, the content of anti-inflammatory drug components (corticoids, diiodothymol) is significantly lower. These components in sealers have been subject to intense criticism for several decades in student textbooks and scientific papers.
Pastes for filling root canals are usually self-hardening. They consist of two mixing components and have different chemical compositions. The list of materials for filling root canals also includes hardening two-component sealers based on polymers (the polyketone-based material Diaket is no longer produced). The dentist has at his disposal various polymer-based sealer systems (AH plus, Sealapex, Apexit, etc.), as well as silicone-based systems (Roeko Seal). Such materials are highly elastic and have a relatively low final hardness. Due to this property, root fillings made from such materials are easily removed during endodontic revision (retreatment).
It is surprising that the nature of the chemical composition of sealers is completely different. There is no evidence-based medicine yet on whether calcium hydroxide (Ca(OH)2) additives are advisable in such materials.
According to the author, the “favorite” material of German dentists in clinics and dental offices is currently AH plus (Dentsply). Many scientific articles are devoted to this material. AH plus consists of two paste-like components mixed in equal parts and is very easy to use. The material replaced the previously widely used sealer AH 26 several years ago. The sealer AH 26 was developed back in 1954 (Schroeder), it released a small amount of formaldehyde (!) (Schäfer, Hickel, 2000). For this reason, the material in its original composition is no longer used.
However, this drug has its advantages and its adherents. Modern material AH 26 supposedly does not contain formaldehyde. And the currently used N2 Endodontic Cement material based on zinc oxide eugenol still (!) contains formaldehyde, but in a “reduced” concentration compared to the previously used similar material.
It is the use of formaldehyde, as well as chlorophenol-camphor-menthol (ChKM) drugs, that is the subject of debate in university circles. All eminent university teachers do not recommend the use of these drugs.
However, at present there is a time of “renaissance” for the Jodoform-Paste material, which contains the drug chlorophenol-camphor-menthol and has long been considered obsolete. According to modern publications, this material is again recommended for use in pediatric dentistry (endodontic treatment of baby teeth).
New materials based on glass ionomers and salicylates with calcium hydroxide additives, as well as MTA (mineral trioxide aggregate) cement, are currently undergoing the test of time in endodontics.
It is noteworthy that there is no single concept regarding the composition of a good “standard” sealer. Each manufacturer offers its own composition options.
There is no single concept regarding the composition of a good sealer. Each manufacturer offers its own option. Rubber-like, highly elastic preparations based on silicones are also advertised and used as materials for filling root canals. For example, the fairly commonly used material Roeko Seal has the property of expanding in volume by approximately 0.2% when cured. This property of the material should ensure a particularly good fit of the root filling to the walls of the root canal.
On the other hand, silicones have the ability to absorb moisture in small quantities. Are root fillings made from silicone-based materials really impervious to bacteria? The author still has serious doubts about this.
Thus, the variety of paste sealers offered for filling root canals is very large. And not only because they are represented on the market by a large number of competing manufacturers, but also due to the diversity of the composition of materials.
Endodontics is still a broad field of experimentation, especially in the field of root canal fillings.
Thermo-mechanical condensation (or filling root canals with a rotating condenser)
This method is currently practically not used. With this technique, a tool that has in its design elements of an H-file (but with a reverse thread) and a channel filler is used to soften the gutta-percha and move it in the apical direction. This instrument is called a condenser or gutta condenser. To soften the gutta-percha and condense it, the instrument must be rotated clockwise at a speed of at least 8000 rpm.
A standard gutta-percha pin should be 1–2 sizes larger than the last instrument used to process the canal, that is, 1–2 mm shorter than the working length. Control of the level of gutta-percha filling is ensured by inserting the instrument, 1.5 mm short of the apical constriction.
The disadvantages of the method are the unpredictability of the level of filling, the high risk of breaking off the instrument in the canal, and the likelihood of voids forming in the gutta-percha due to its gluing to the instrument. In addition, this technique also does not provide reliable obturation of the lateral branches of the canal.
Materials for temporary canal filling
There are conflicting opinions about the need to replace calcium hydroxide paste in the canal with new portions. HSChawla suggests that a single application is sufficient. A. Chosack et al. It is believed that repeated administration of calcium hydroxide is necessary after 1-3 weeks. Proponents of one-time fillings point to the fact that the hydroxide is only needed to initiate the reparative reaction, so no replacement of the drug is required. Many authors suggest re-introducing calcium hydroxide paste into the canal only when symptoms worsen.
The results of the study showed that Ca(OH)2 in its pure form is not always effective in destroying microbes, for example E.faecalis, C.albicans. A paste of calcium hydroxide with iodoform turned out to be more effective, penetrating into the tubules to a depth of more than 300 microns.
Calcium hydroxide paste with paramonochlorophenol and glycerol killed bacteria, including E. faecalis, within 24 hours of use. Calcium hydroxide in combination with 2% chlorhexidine gel has increased antimicrobial activity against resistant microorganisms.
The question of how long the hydroxide remains in the channel remains controversial.
In accordance with the recommendations of most companies, the duration of stay of the products in the tooth is up to 14 days, which creates some inconvenience in the work, namely, some patients do not complete the treatment, forgetting about the need to visit the dentist again. On the other hand, research results have shown that the paste creates an antibacterial effect after just 1 day of use. Calcium hydroxide causes complete inactivation of various types of microorganisms within 12-72 hours (Stuart et al., Estrela et al.). The combination of chlorhexidine and hydroxide inhibits the growth of E. faecalis 100% after 1-2 days of contact.
These results are confirmed by our own microbiological studies of the contents of the root canal after each of the three stages: standard mechanical and medicinal treatment; additional medicinal effects with a 2% solution of chlorhexidine for 2-3 minutes; temporary filling with calcium hydroxide or hydroxide in combination with iodoform for 48 hours. For this purpose, scraping was carried out from the walls of the root canals with an H-file, which was placed in a sterile tube with a transport system (2 ml of trypticase soy broth). The latter was delivered in thermal containers to the microbiological laboratory (40 samples).
0.1 ml of the prepared homogenizate was continuously inoculated onto a blood agar plate. Petri dishes were placed in a thermostat. Cultivation was carried out at 35-37 0C for 48 hours. When growth appeared, colonies were counted by determining CFU per 1 ml. Gram-stained smears were examined under a light microscope for the purpose of generic identification of microorganisms. In root canals with an initially low degree of contamination after standard mechanical and medicinal treatment, the number of microorganisms was 100 CFU/ml. Temporary filling of the canals with a paste based on calcium hydroxide made it possible to reduce the number of microorganisms to the level of 0[0/0] CFU/ml.
With an initially high degree of contamination, the contamination of the canals decreased significantly at each stage of the study. Thus, after standard treatment, the microbial number was 1,400 CFU, after drug treatment with a 2% chlorhexidine solution - 200 CFU, after temporary filling (for 48 hours) - 0 [0/100] CFU.
Thus, the use of additional medicinal treatment and temporary filling makes it possible to reduce the number of microorganisms in the root canal to a minimum.
Preliminary clinical trials have shown that reducing the residence time of calcium hydroxide in the canal under a temporary filling to 48 hours reduces the risk of incomplete treatment of pulpitis and periodontitis by 8-11%, and the combined use of calcium hydroxide preparations with iodoform reduces the number of complications by 5-25%.
Filling root canals with chemically softened cold gutta-percha
Filling techniques using chemically softened cold gutta-percha are also called “immersion methods.” Historically, these methods appeared almost simultaneously with the beginning of the use of gutta-percha. For obturation of gutta-percha softened with solvents (chloroform, some oils), no sealer was used. This led to micro-seepage due to shrinkage of the gutta-percha after the solvent evaporated and the root filling hardened. Therefore, the incidence of complications when using such techniques was very high. Despite the fact that later various sealers began to be used with “immersion” methods, these techniques are currently practically not used due to the inability to control the shrinkage and deformation of gutta-percha and the quality of canal obturation.
Indications and contraindications
|
|