- An effective way to preserve the integrity of the tooth and prevent the spread of infection.
- Modern painless methods of performing the procedure.
- The fastest possible return to normal life.
Sign up for a consultation
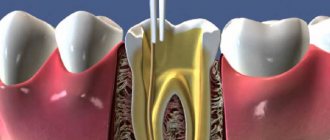
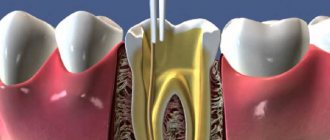
Once the pulp (nerve tissue and blood vessels) is removed, the tooth becomes hollow. If it is not filled with filling material, then the process of spreading caries and other infections will continue. Pathogenic microflora can lead to damage to the periodontium - the tissues surrounding the root of the tooth, in which case there is a high probability of its loss. In addition, the spread of infection can lead to the formation of cysts and fistulas, the appearance of sinusitis and osteomyelitis. In order to prevent this, obturation (filling) of the canal of the pulpless tooth is performed.
Indications and contraindications
|
|
Any intervention associated with the treatment of dental root canals leads to a response from the body, expressed in local and general manifestations [11].
Pain is the body’s protective reaction to various damaging influences. The problem of pain relief in patients with pulpitis and periodontitis at the stages of endodontic root canal treatment remains very relevant in modern medical practice [2, 10].
Pulpitis is an inflammation of the pulp associated with the ingress of microorganisms into it. During the treatment stages of pulpitis, pain may occur, which is most often associated with the fact that:
— during the process of pulp removal, the neurovascular bundle is torn off;
— during mechanical treatment of root canals, the instrument may slightly penetrate the periapical tissues, injuring them;
— during medicinal treatment of root canals, antiseptic substances can enter in small quantities into the tissues in the area of the root apex, causing an irritating effect on them [8].
Another nosological form requiring endodontic root canal treatment is periodontitis. One of the reasons for the occurrence of periodontitis may be poor-quality previously performed mechanical, medicinal treatment and subsequent obturation, as a result of which a certain amount of microflora may remain in the root canal. Most likely, these remaining microorganisms will multiply, enter surrounding tissues and maintain inflammation (Figure 1).
Figure 1. Chronic periodontitis of teeth 3.6, 3.7. X-ray. And inflammation is the cause of pain [1].
Many authors acknowledge that the determining factors in the development of post-filling pain may be the method of root canal preparation, the nature of medicinal treatment, the level of filling, and obturation material [3, 4].
In addition, during endodontic treatment, trauma to periapical tissues often occurs and soluble inflammatory mediators are released, which can influence the development of pain in different ways and/or at different levels of signal transduction [5].
Among the mediators of inflammation, eicosanoids (prostaglandins - PG, thromboxanes and leukotrienes) play a key role in the pathophysiology of pain. All eicosanoids are produced from arachidonic acid through activation of lipoxygenase-dependent or cyclooxygenase (COX)-dependent biotransformation pathways. COX catalyzes the synthesis of PGE2, which is a precursor of biologically active PGs and thromboxanes.
Thus, the management of the period of post-endodontic treatment of patients must be carried out taking into account adequate pain relief and the effect on the phases of inflammation.
The use of non-steroidal anti-inflammatory drugs (NSAIDs) has become widespread in the clinical practice of dentists [7].
As is known, the mechanism of pathogenetic action of NSAIDs is:
— stabilization of cellular and intracellular membranes;
- suppression of the synthesis of PGs and oligopeptides responsible for the occurrence of pain;
— reducing the level of free radicals in tissues;
- direct effect on cells directly involved in inflammatory reactions.
The purpose of the study was to reduce pain in patients with pulpitis and periodontitis in the postendodontic period after temporary and permanent obturation of the root canals by prescribing the drug dexalgin 25.
NSAIDs are a group of drugs widely used in clinical practice. The great “popularity” of NSAIDs is explained by the fact that they have anti-inflammatory, analgesic and antipyretic properties and bring relief to patients with corresponding symptoms (inflammation, pain, fever) [10]. Thanks to this, their use in the practice of an endodontist is possible.
Over the past 30 years, the number of NSAIDs, differing in their characteristics of action and use, has increased significantly.
NSAIDs include several chemically heterogeneous classes of drugs that differ in their mechanism of action and the severity of anti-inflammatory activity [13].
Classification of NSAIDs by mechanism of action
Selective COX-1 inhibitors: acetylsalicylic acid.
Non-selective COX-1 and COX-2 inhibitors: most NSAIDs.
Drugs with a predominant effect on COX-2: meloxicam, nimesulide.
Highly selective COX-2 inhibitors: celecoxib, rofecoxib.
The main and general element of the mechanism of action of NSAIDs is the inhibition of PG synthesis from arachidonic acid by inhibiting the COX enzyme (PG synthetase). Although all NSAIDs inhibit both COX-1 and COX-2, the level of this action varies and can be attributed predominantly to one of the isoenzymes. Additionally, NSAIDs exert their effects through various peripheral mechanisms, such as modulation of membrane receptors, signal transporters and mediators, as well as by influencing the “inflammatory cascade” [9] (see diagram).
Scheme 1. Scheme. Synthesis of prostaglandins (PG).
Material and methods
To manage patients in the postendodontic period and achieve an analgesic effect, we chose the drug dexketoprofen trometamol (Dexalgin 25, Berlin-Chemie/Menarini Pharma GmbH, Germany) (Fig. 2),
Figure 2. The drug dexalgin 25 has a pronounced analgesic effect [12].
The mechanism of the analgesic effect of the drug Dexalgin 25 is a blockade of:
- production of pain mediators in the periphery due to inhibition of COX activity;
- conduction of pain along peripheral nerves and pathways of the central nervous system due to depolarization of neuron membranes;
— production of pain mediators in the central nervous system, including the cortex and deep parts of the brain, due to inhibition of COX activity in these parts [6].
The study involved 33 patients (15 men and 18 women) aged from 18 to 65 years. The inclusion criterion was the presence of pain after root canal filling and treatment for pulpitis and periodontitis of teeth of various groups.
Exclusion criteria from the study were: age under 18 years and over 65 years, history of severe somatic pathology, allergy to NSAIDs.
The diagnosis was established in accordance with the ICD-10 classification. Acute pulpitis was in 6 patients, chronic pulpitis - in 8, chronic apical periodontitis - in 9 and acute apical periodontitis - in 10.
Using randomization, patients were divided into two groups.
Endodontic treatment of 39 teeth was carried out: primary treatment of pulpitis - 18 teeth and secondary treatment (root canal retreatment) - 21 teeth (Table 1).
Patients in the main group (23 people) received dexalgin 25 25 mg orally as an anesthetic drug during meals, repeating the dose after 8 hours as needed; patients in the control group (10 people) did not take any analgesic drugs.
All patients had their blood pressure and heart rate measured before taking the drugs and 30 and 60 minutes after taking them. A control examination was carried out on the 2nd and 3rd days of the study. During the visit, patients were interviewed, the oral cavity was examined, and the effectiveness and side effects of the drug were assessed based on subjective and objective data.
To study the frequency and characteristics of post-filling pain, a patient survey method was used.
The severity of pain was assessed using a 4-point system (1 - no pain, 2 - mild pain, 3 - moderate, 4 - unbearable) on days 1, 2 and 3 after endodontic treatment.
To obtain an accurate subjective assessment, the nature of post-filling pain was studied:
- pain at rest and its intensity (weak, moderate, severe);
- pain when biting on a tooth (mild, moderate, severe);
- presence of night pain;
— how many days there was pain (Table 2).
Research results
According to the results of the survey, patients who did not take the drug dexalgin 25 noted spontaneous pain at rest and pain when biting within 2-3 days after completion of endodontic treatment 2 times more often than patients in the main group. 3 patients in the control group had severe pain when biting, which did not completely go away by the 3rd day without taking analgesics. Pain at rest of mild and moderate intensity was observed in 80% of all patients in the control group.
In patients of the main group who received the drug Dexalgin 25, the onset of analgesia was quite rapid; there were no cases of lack of analgesia effect.
In 19 patients of the main group, mild pain was noted when biting on the 1st day after endodontic treatment. After a single dose of 25 mg of the drug, the full analgesic effect occurred within 2 hours and persisted for 6-8 hours. In 5 of 19 patients, it became necessary to re-administer 25 mg of the drug after 8 hours. On the 2nd day of examination, none of these patients experienced pain or discomfort from the treated tooth, and chewing function was restored in full. In 4 patients, on the first day after treatment, pain was noted at rest, which was relieved 2 hours after taking 25 mg of the drug Dexalgin 25. We also established the relationship between the intensity and nature of pain in teeth treated in one or two visits. At the same time, during dental treatment in one visit, the drug dexalgin 25 was prescribed once at a dose of 25 mg; in only one case, the patient re-took the analgesic 8 hours after treatment. But even in this case, after 24 hours, the pain syndrome was completely relieved. When treating in two visits, after the first stage (temporary filling), the drug dexalgin 25 was prescribed 25 mg 1-2 times a day with an 8-hour interval, and after the second stage (permanent obturation), in 90% of cases the prescription of NSAIDs was not required.
When comparing the condition of the teeth after treatment for pulpitis and periodontitis, we did not obtain any significant differences; in both cases, on the 2nd day after taking the drug Dexalgin 25, post-filling pain disappeared.
However, we found that in multi-canal teeth, especially in the upper jaw, pain when biting, pain at rest and night pain were 1.5 times more common than in the treatment of single-canal teeth. In all cases, the patient took the drug again within 1 day.
An analysis of side effects showed that the drug Dexalgin 25 was well tolerated by patients. No adverse reactions such as skin rash, itching, nausea, or dizziness were noted. According to the patients, the rehabilitation period was gentle and quick, lasting 2-3 days.
Clinical studies have shown that the analgesic effect was achieved in all patients taking the drug Dexalgin 25.
Clinical examples
Example No. 1
Patient A. was admitted with complaints of spontaneous sharp unbearable pain, intensifying in the evening, in the area of the upper jaw teeth on the left.
Objectively: on the contact-distal surface of tooth 2.7 there is a deep carious cavity filled with softened pigmented dentin. Probing the bottom of the cavity is sharply painful.
The radiograph shows that the carious cavity of tooth 2.7 communicates with the tooth cavity. An expansion of the periodontal fissure of tooth 2.8 was detected (Fig. 3).
Figure 3. Chronic apical periodontitis of tooth 2.8, acute pulpitis of tooth 2.7. X-ray.
Based on the patient's complaints, clinical and radiological picture, a diagnosis was made according to the ICD-10 classification: acute pulpitis of tooth 2.7, chronic apical periodontitis of tooth 2.8.
It was decided to remove tooth 2.8 and perform endodontic treatment on tooth 2.7 (Fig. 4).
Figure 4. Situation after removal of tooth 2.8 and endodontic treatment of tooth 2.7. X-ray.
Patient A. was prescribed the drug Dexalgin 25, one tablet (25 mg) orally with meals for 3 days after filling the root canals of tooth 2.7. On the 1st day after endodontic treatment, the patient noted minor pain when biting, which stopped the very next day.
Example No. 2
Patient B. complained of constant aching pain and pain when biting in the area of the upper jaw tooth on the right.
Objectively: there is a filling on the chewing-medial surface of tooth 1.6 with signs of a violation of the marginal seal. Percussion of the tooth is painful.
The radiograph clearly shows the expansion of the periodontal fissure of tooth 1.6 (Fig. 5).
Figure 5. Chronic apical periodontitis of tooth 1.6. X-ray.
Based on complaints and clinical and radiological picture, a diagnosis was made: chronic apical periodontitis of tooth 1.6.
After temporary filling of root canals (Fig. 6)
Figure 6. Condition of tooth 1.6 after root canal filling. X-ray. the patient was recommended to take the drug dexalgin 25, 25 mg each, during the first 2 days. After the permanent obturation stage there was no need to prescribe NSAIDs, the patient had no complaints.
Conclusion
A randomized, open-label study of the effectiveness and tolerability of the drug dexalgin 25 (dexketoprofen trometamol) revealed its high analgesic efficacy and good tolerability.
The advantages of the drug are ease of use and low incidence of undesirable effects on the circulatory system. The drug is usually well tolerated and has relatively weak ulcerogenic activity, which is considered one of its main advantages over acetylsalicylic acid.
Thus, the management of the period of post-endodontic treatment of patients must be carried out taking into account adequate pain relief and the effect on the phases of inflammation. The use of dexketoprofen trometamol (Dexalgin 25, Berlin-Chemie/Menarini Pharma GmbH, Germany) at a dose of 25 mg per dose helps reduce post-filling pain.
Materials for root fillings
Prices for dental canal filling depend on the chosen procedure method and the consumables used. We, as modern dentistry, use:
- plastic material, gutta-percha, for the main filling of the tooth canal
- and special sealers and pastes to ensure maximum tightness.
Gutta-percha is the most modern material with antibacterial activity. It does not dissolve and does not lose its properties throughout the life of the tooth. The sealer we use (AH plus, Dentsply, USA) is recognized as the “gold standard” for root canal treatment all over the world.
Canal filling techniques
Lateral condensation method
Vertical condensation of gutta-percha
A simple and effective way to fill root canals. The doctor applies a liquid paste to the gutta-percha pin, after which the latter is inserted into the tooth cavity. Using the tool, the cavity is filled with additional pins, which completely seal the canal.
This is a method of filling tooth canals with a complex shape (anatomy). Using a special thermal nozzle, the doctor introduces heated and softened gutta-percha into the canal.
Instrumental treatment of formed dental root canals
Endodontic treatment of permanent teeth that already have a fully developed root canal system is carried out using methods used for adult patients. During the treatment process, the doctor’s main tasks are to give the cavity a funnel shape with minimal expansion in the area of physiological narrowing and maximum expansion at the entrance. The specialist also needs to ensure that the position of the apical foramen remains unchanged and form a reliable stop for the filling material. During the instrumental treatment of permanent teeth, it is recommended to regularly rinse the cavity. K-reamers, as well as H- and K-files can be used to scrape tissue from the canal walls. The preparation technique can be based on one of the following methods:
- Step-back. Also known as the apical-coronal technique or “step back”. Involves the expansion of root canals from the apical foramen towards the orifices. Requires the use of tools with ever increasing diameter sizes.
- Step-down. This technique is also called “step forward” or coronal-apical. In this case, canal processing is performed in the opposite direction to the previous method: from the root orifices to the apex.
- Combined. This hybrid method involves the use of two techniques at once. As a rule, at the initial stage, the crown is processed using the step-back principle, after which the canals are developed using the step-down method.
Treatment regimen
- Diagnostics Before treatment, an x-ray or computed tomography must be done to determine the number of channels, their location and shape.
- Anesthesia The doctor selects an anesthetic and, if necessary, conducts sensitivity tests to various drugs.
- Installation of a rubber dam An obligatory aspect of modern treatment is the isolation of the tooth from oral fluid using a special latex scarf (rubber dam).
- Instrumental and medicinal canal treatment The essence of root canal treatment is high-quality disinfection of the tooth cavity. To do this, the doctor expands the canal with instruments, gives it the desired shape and rinses it with disinfectant solutions to destroy the infection.
- Preparing the canals The doctor measures the length of the canals using an apex locator, after which they are mechanically expanded and smoothed out the walls.
- Filling canals Cement, a pin, or a combination of both are injected into the prepared cavities, depending on the chosen treatment method.
- Control image The doctor evaluates the quality of canal filling, after which he performs tooth filling and other necessary procedures. In addition, the patient receives recommendations for further oral care.
Instrumental treatment of root canals of temporary teeth
In this case, specialists do not need to give the cavity being treated a standard cone shape, since this can lead to dangerous thinning of the very fragile walls. The main task in the canal treatment process is to remove infected predentin and create an apical stop. However, reamers are used only when it is necessary to process very narrow cavities. In most cases, H-files are used during the treatment process. The diameter of the instrument increases as it goes deeper into the root canal. There is no standard for the amount of expansion of the internal root cavity. But in practice, the canals of molars are usually increased to 25-35 sizes, and of the front teeth - to 70-90 or more. The main requirement is that the expansion of the cavity should not exceed 2-3 times the size of the original size of the apical section. It is also recommended to correctly prioritize by preparing the more complex mesial and buccal canals of molars first.
Temporary canal filling
If indicated, the doctor can fill the canals after depulpation not with filling material, but with a medicinal agent (antibacterial, anti-inflammatory). The drug remains in the tooth cavity for a certain time, after which it is removed, and the vacated canal is sealed.
The procedure can be prescribed:
- if there is a need to sanitize the canals if a deep infectious process is suspected;
- if the patient has acute periodontitis;
- for temporary sealing of the canal, if it is necessary to monitor the condition of the tooth cavity after removal of the inflamed pulp.
In addition, the procedure can be prescribed for tooth injuries, for example, a fracture of the crown or root.