Advantages and disadvantages
For simple surgical interventions, local anesthesia is indispensable; it has advantages over other types of sensitivity suppression. The drug that is used, an anesthetic solution, acts strictly at the injection site, which helps to avoid severe complications and adverse reactions.
The blockade of pain sensitivity develops on average in 10-15 minutes. The effect lasts for an hour or more, so local anesthesia can reduce pain in the area of the postoperative wound. The patient’s consciousness does not suffer from the action of the local anesthetic, so after the manipulation he can leave the clinic and not be in the ward.
But local anesthesia has its drawbacks. Just a few years ago, it was widely used for operations on superficial tissues and extremities; methods for intravenous administration of drugs with simultaneous application of a tourniquet were developed. Intraosseous anesthesia was widely used. But due to the large number of adverse reactions and complications, these methods began to be used less frequently. And after receiving high-quality drugs for anesthesia, dangerous methods of pain relief were practically abandoned.
The disadvantage of the local method is its limited scope of application. It is effective for anesthesia of mucous membranes, skin and superficial tissues, but is not used for operations on the abdominal and pelvic organs, neck and head.
The infiltration type of local anesthesia cannot be used when operating on malignant tumors due to the possibility of tumor cells entering beyond the wound into other tissues. This increases the risk of developing metastases.
Types of local anesthesia
Several types of local anesthesia are used in surgical practice, but some of them already have historical significance. The main methods of pain relief are the following:
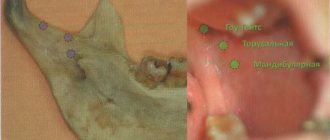
- superficial anesthesia - pain sensitivity is suppressed after the anesthetic comes into contact with the surface of the tissue, most often used to anesthetize the mucous membranes. The anesthetic solution is applied by lubrication or irrigation, the effect lasts for 10 minutes;
- infiltration anesthesia - anesthesia by impregnation, or infiltration of tissue layers with a local anesthetic. The technique allows you to control the depth and width of the drug injection, depending on the intended incision. The medicine is injected carefully first into the subcutaneous area until the lemon peel effect appears, then the needle is gradually moved inward and an additional dose of the drug is injected;
- anesthesia according to Vishnevsky is an improved version of the infiltration method. A weak anesthetic solution is injected layer by layer under high pressure. A tight creeping infiltrate forms in the tissues. It spreads through the interfascial spaces and disrupts the conduction of impulses along the nerves passing through them. After cutting the wound, the liquid gradually flows out of the wound, so there is no risk of its absorption into the systemic circulation and the development of toxic reactions;
- conduction anesthesia is the essence of the method in anesthetizing a specific area of the body innervated by the nerve trunk. An anesthetic drug is injected into the tissue around the nerve; the technique is used for operations on the limbs;
- spinal anesthesia - the analgesic effect is achieved by injecting an anesthetic drug under the choroid of the spinal cord, the main place of drug administration is the lumbar region, and pain sensitivity in the pelvic organs and lower extremities disappears. But tactile sensitivity does not suffer;
- epidural anesthesia is a type of anesthesia in which a local anesthetic is injected into the space over the dura mater of the spinal cord, and a puncture is also performed in the lumbar region. Sensitivity is lost after 15-20 minutes, but the effect lasts for 3-4 hours. The use of this type of anesthesia allows you to resume activity early after surgery;
- bone anesthesia is a type of anesthesia in which an anesthetic solution is injected into spongy bone. Currently, it is practically not used; previously it was used for operations on the limbs.
Clinical pharmacology of local anesthetics
A.M. Ovechkin*, S.A. Osipov** Moscow Medical Academy named after I.M. Sechenov*, Russian Medical Academy of Postgraduate Education**, Moscow
Local anesthetics (LAs) are the pharmacological cornerstone of regional anesthesia.
Chemical structure of MA.
The local anesthetic molecule consists of three components: a lipophilic aromatic benzene ring, a hydrophilic tertiary amine and a chain connecting them. The chemical bond between this chain and the aromatic ring allows MAs to be classified into “ether” and “amide”. Amide anesthetics are more stable and, unlike ether ones, practically do not cause allergic reactions.
In addition to the basic molecular structure, some amide MAs (bupivacaine and ropivacaine) also differ as stereoisomers, which determines the characteristics of their pharmacodynamics. Steroidisomers have the same chemical formula, but differ in the order of the atoms around the main carbon atom. Isomers can be designated as (+) and (-), or as R and S (right- and left-handed. The designation (+) and (-) indicates in which direction the molecule rotates polarized light - to the right (+, R), i.e. i.e. clockwise and left (-, S), counterclockwise.In particular, bupivacaine exists simultaneously in S (-) and R (+) form (racemic mixture), ropivacaine - in the form of pure S (-) isomer.
Clinical pharmacology of MA.
Currently, ester MAs are not used in our country for neuraxial blockades, therefore, when discussing the advantages and disadvantages of modern MAs, we will talk mainly about amide anesthetics. The intermediate-acting anesthetic lidocaine (Xylocaine), as well as the long-acting MAs bupivacaine (Marcaine) and ropivacaine (Naropine), are available in clinical practice today.
As is known, the main clinical characteristics of MA are:
- power
- speed of development of the effect (latent period)
- duration of action
- toxicity
The physicochemical properties of MA (which, in turn, depend on the chemical structure) largely determine their potency, toxicity and clinical effectiveness.
The main properties of local anesthetics are presented in Table 1.
Table 1. Physicochemical properties of local anesthetics
.
Lipid solubility MA
The potency of MAs primarily depends on their ability to dissolve in fats, since neuronal membranes are a lipoprotein matrix consisting of 90% lipids. LAs with greater lipid soluble properties are more potent. The lipophilicity of anesthetics facilitates their penetration through neuronal membranes, which accelerates binding to proteins of the intracellular part of the sodium channel.
Ionization and dissociation constant (pK)
MA are weak bases (pK = 7.6-9.0). The pK value (dissociation constant) is determined by the pH at which half of the drug molecules are in ionized and half in non-ionized (basic) form. The pK value is constant for each MA. The properties of the ionized and basic forms are different. Predominantly non-ionized molecules penetrate the cell membrane. The higher the pK of the anesthetic, the fewer its molecules are in non-ionized form.
MAs with a higher pK (bupivacaine, ropivacaine) are characterized by a delayed onset of action, due to a smaller number of non-ionized molecules at the body pH. The pK value of bupivacaine (8.1) corresponds to a 20% share of the basic form of the drug at tissue pH.
The ability of MA to bind proteins
One of the most important characteristics of MAs is their duration of action. It largely depends on the ability to bind to proteins (mainly β-acid glycoprotein (AGP)). Long-acting LAs such as bupivacaine and ropivacaine have a high protein binding potential. This feature determines their long-term binding to proteins of neuronal sodium channels, and therefore a longer duration of action. Patients with low plasma protein levels have an increased risk of systemic toxicity of LA. The plasma concentration of KAGP increases under various pathological conditions (surgery, trauma, serious illness), which increases the degree of binding of MA by plasma proteins, i.e. plays a protective role.
The ability to bind to plasma proteins also affects the systemic toxicity of MA, which is caused exclusively by the free, unbound fraction of the drug. It should be remembered that when plasma proteins become “saturated” with MA molecules, their binding capacity is exhausted. In this case, the introduction of an additional dose of anesthetic (or its absorption from the epidural space) can quickly cause a toxic effect.
Systemic absorption of MA
The duration of neuronal blockade, as well as the manifestations of systemic toxicity, largely depend on the rate of systemic absorption of MA from the point of its administration. The degree of vascularization of the area of the body into which the drug is injected affects the rate of its absorption into the systemic circulation, as well as the peak plasma concentration. The value of the latter can be presented in the following order: with intrapleural block > intercostal block > lumbar EA > brachial plexus block from the axillary approach.
Factors influencing the rate of absorption are the degree of ionization of the drug (pK), its lipid solubility, ability to bind to plasma proteins, as well as the nature of vascularization and perfusion of surrounding tissues. In addition, the rate of absorption of MAs is influenced by the degree of their vasodilating effect. It is generally accepted that all MAs, with the exception of cocaine, are vasodilators. This effect is especially pronounced in lidocaine, which makes it advisable to add adrenaline to prolong its action. It was recently established that ropivacaine has its own vasoconstrictor effect, so the duration of its action does not depend on the addition of external vasoconstrictors.
In late pregnancy, the initial peak plasma concentration of LA may be higher than normal. Due to hormonal changes, increased permeability of tissue membranes to LA, decreased binding of MA to plasma proteins, and their increased cardiotoxicity against the background of increased progesterone synthesis increase the risk of systemic toxic effects of LA (especially bupivacaine).
Metabolism of MA
Amide MAs are destroyed in the liver, with the participation of the cytochrome P450 system, from 1 to 5% of the drug is excreted unchanged in the urine. The half-life of amide MAs is significantly longer than that of ether MAs. The clearance of amide MAs is largely dependent on hepatic blood flow and enzyme activity. It may be impaired by heart failure, liver failure, or taking b-blockers or H2-receptor blockers.
Renal failure does not have a significant effect on the clearance of LA, since the process of their inactivation occurs mainly in the liver. However, accumulation of metabolites is possible.
Differentiated blockade
The ideal LA used for postoperative pain relief should selectively block nociceptive fibers A? and C, without affecting motor fibers A? and A?. It has been established that ropivacaine in low concentrations (0.2%) causes a predominant blockade of A-delta and C-fibers, while it blocks C-fibers faster than A-fibers (Wildsmith J., 1997). Reducing the concentration of anesthetic (0.125%) increases the selectivity of sensory blockade. At higher concentrations (0.5-0.75%), bupivacaine and ropivacaine exhibit similar effects on motor and sensory fibers. The ability of ropivacaine to cause differentiated sensorimotor block is its clinical advantage over bupivacaine.
MA dosing. Is the concept of “maximum recommended dose” acceptable?
The issue of choosing the optimal dose of LA for a particular method of regional anesthesia still remains controversial. The situation with spinal anesthesia is most clear - we have the only anesthetic spinal marcaine 0.5% (simple and heavy), there is a minimum effective dose of 10 mg and a maximum possible dose of 20 mg. Within this framework, we must operate with doses, taking into account the patient’s age, his volume status, the volume of surgical intervention, etc.
The situation with the choice of dose of LA for brachial plexus block is more or less clear, since it is known that its effectiveness is determined by the volume of the administered LA solution (35-40 ml). Thus, the total dose depends on the concentration of the drug chosen (lidocaine 1-1.5%, bupivacaine 0.25%-0.5%, ropivacaine 0.75%).
The greatest difficulty is in choosing the optimal dose of MA for EA. At present, the long-standing recommendations on the dosage of LA for EA in milliliters per segment, milligrams per kilogram, etc., have been recognized as completely untenable. What should you be guided by, the maximum dose of the drug recommended by its manufacturer?
The MA maximum recommended dose (MRD), often listed in package inserts or catalog text, is widely used as a simple quantitative measure of the safe use of a drug, usually expressed in mg/kg body weight. At the same time, none of the recommended doses are scientifically justified. The main goal of all existing recommendations is to avoid the administration of an excessive dose of anesthetic that can have a systemic toxic effect. However, this usually does not take into account the site of drug administration, as well as the factors influencing its metabolism and excretion.
Most experts currently reject the concept of MRD, as they consider it to be misleading due to:
- The existence of pronounced individual differences in drug tolerability.
- Possibility of a severe toxic reaction in case of unintentional intravenous injection of a dose significantly lower than the MRD.
- The MRL concept may create the illusion of safety when doses below the MRL are used, as well as the false impression that higher doses are inherently dangerous.
As an example, we will give some MRDs of local anesthetics presented in fundamental foreign guidelines on anesthesiology.
Maximum doses of MA in adults (Cousins M. & Bridenbaugh P. Neural Blockade in Clinical Anesthesia and Management of Pain, 3rd ed., 1998, Miller R. Anesthesia, 5th ed., 2000)
| Drug (trade name) | Type and year of implementation | Relative power | rK | Fat solubility | Protein binding |
| Procaine (Novocaine) | Essential, 1905 | 1 | 8,9 | 0,6 | 5,8 |
| Amidny, 1947 | 4 | 7,7 | 2,9 | 64,3 | |
| Bupivacaine (marcaine, anecaine) | Amidny, 1963 | 8 | 8,1 | 27,5 | 95,6 |
| Ropivacaine (naropin) | Amidny, 1996 | 7 | 8,1 | 14 | 94 |
| Local anesthetic | Simple | With adrenaline | |||
| Lidocaine | 300 mg | 500 mg | |||
| Bupivacaine | 175 mg | 225 mg |
It is interesting to note that in Europe the MDI of simple lidocaine throughout the entire period of use of the drug did not exceed 200 mg, while in the USA it was 300 mg. A number of reports of severe complications associated with the use of bupivacaine (including death) have led to a reduction in the recommended dose.
Maximum doses of bupivacaine and ropivacaine in adults (Pharmaca Fennica 2002, Finland,
Rosenberg P. )
| Local anesthetic | Single dose | Daily dose |
| Lidocaine | 150 mg (2 mg/kg) | 400 mg |
| Bupivacaine | 225 mg | 800 mg |
In this regard, today it is more correct to talk about the range of doses acceptable for the average adult. In addition, the dose should be adjusted taking into account the condition (age) of the patient, as well as the type and extent of the planned operation. In all cases, it is necessary to strive to use the lowest effective dose.
Thus, the concept of a “maximum recommended dose” should now be abandoned, or at least revised.
Most authors have recently avoided the term “maximum recommended dose” of MA, citing instead the effective doses of various MA in relation to a particular RA technique.
As for EA, in our opinion, in a real clinical situation, choosing the optimal dosage regimen for MA does not pose any particular problems. In modern anesthesiology, EA is most often used as a component of: a) combined spinal-epidural anesthesia, b) a component of general anesthesia (high EA during operations on the upper floor of the abdominal cavity, chest organs). In the first case, anesthesia during surgery is achieved mainly through the spinal component and only sometimes epidural administration of LA boluses is required (6-7 ml of 0.5% bupivacaine or 0.75% ropivacaine). In the second case, the administration of LA during the operation is also carried out in small boluses (8-10 ml of 0.5% bupivacaine or 0.75-1% ropivacaine), in a “step by step” mode, focusing on the stage of the operation, the volume of blood loss, hemodynamic indicators, etc. In those rare cases when EA is an independent method of anesthesia, its induction is carried out in a similar mode, through bolus administration of small doses of LA through a catheter, with monitoring of hemodynamics and the rate of development of sensory block. Simultaneous EA (without catheterization of the epidural space) today should be excluded from the anesthesiological arsenal, since SA is a technically simpler, more effective, safe and economically feasible alternative.
Allergic potential of MA
In most cases, reports of allergic reactions caused by LA represent a false interpretation of various clinical situations caused by the action of these drugs. Most often they come from dental practice and, upon closer examination, turn out to be the result of accidental intravascular injection of LA (especially adrenaline-containing ones).
True allergic reactions to MA are extremely rare and, in the vast majority of cases, are associated with the use of essential MA. Most often they are caused by para-aminobenzoic acid, which is one of the degradation products of essential MAs.
In the literature there are literally isolated reports of allergic complications caused by amide MAs.
Toxicity of MA
The toxicity of LA manifests itself in the form of systemic (effects on the central nervous system and cardiotoxicity) and local toxic reactions (direct neurotoxic effects). Systemic toxicity occurs mainly with accidental intravascular administration of LA and is characterized by central nervous system stimulation, as well as convulsive activity.
Large doses of LA increase the risk of systemic toxicity, while high anesthetic concentrations and prolonged exposure (to a greater extent than the total dose) determine the direct neurotoxic effect.
Neurotoxicity of MA
Histological criteria for the neurotoxic effect of LA are damage to Schwann cells, as well as axonal degeneration and vacuolization of neonic membranes.
Lidocaine, in comparison with bupivacaine (Marcaine), has a significantly higher direct neurotoxic effect. The extreme degree of neurotoxicity is the development of transient neurological syndrome (TNS). In the vast majority of cases, the development of TNS is caused by the use of lidocaine (regardless of the dose and concentration) in SA and, to a lesser extent, in EA.
Systemic toxicity of LA (effects on the central nervous system)
Depending on the injection site, signs of systemic toxicity may appear immediately or several hours after injection of the drug. Experimental studies have shown that the higher the rate of administration of MA, the lower its dose that causes seizures.
In clinical settings, seizures most often occur due to systemic absorption when large doses of LA are used to block peripheral nerves and plexuses, as well as when LA is inadvertently administered intravenously in doses intended for regional anesthesia. The latter situation is possible when the epidural catheter is inserted into the vertebral vein unrecognized. SA from this point of view seems to be the safest (maximum dose - 20 mg of spinal marcaine).
Manifestations of systemic toxicity are directly related to plasma concentrations of MA. Administration of LA into highly vascularized areas (intercostal nerve block) is associated with a greater increase in plasma concentrations of anesthetic compared with the same dose of drug used for femoral nerve block.
It is important to remember that the systemic toxicity of lidocaine progresses with increasing doses from signs of CNS toxicity to cardiotoxicity. At the same time, the toxic effect of powerful MAs (bupivacaine) can immediately manifest itself as severe cardiovascular failure.
Cardiotoxicity of MA
The cardiotoxic effect of MA is determined by several components. First of all, blockade of Na channels disrupts normal atrioventricular conduction. Another factor determining the cardiotoxicity of LA is their inhibitory effect on ATP synthesis in mitochondria.
In vitro, it was found that the high cardiotoxicity of bupivacaine is associated with its extremely slow dissociation from Na channels. In particular, the period of binding of bupivacaine to the Na channels of the cardiac conduction system is 1000 times longer than that of lidocaine. Na channel blockade caused by bupivacaine is very persistent, which significantly reduces the effectiveness of resuscitation measures for ventricular fibrillation (McClure J.1996). It was later found that the cardiotoxic effect has a pronounced stereospecificity (bupivacaine is a racemic S- and R-rotating isomer), since the S-isomer has significantly less toxicity compared to the R-isomer.
After this, a new amide anesthetic, ropivacaine, was created and introduced into the clinic in 1996, which is a pure S-isomer and is an analogue of bupivacaine, in which the butyl group is replaced by propyl.
Ropivacaine's affinity for Na channels is intermediate between lidocaine, which binds rapidly to an open Na channel and rapidly dissociates during the relative refractory period, and bupivacaine.
It has been established that ropivacaine-induced myocardial depression and arrhythmia are less pronounced than the similar effect of bupivacaine, while a 10-fold increase in the concentration of ropivacaine does not significantly enhance its cardiotoxic effect (Carpenter R., 1997).
Under experimental conditions, it was found that ropivacaine suppresses ATP synthesis in myocardial mitochondria to a lesser extent than bupivacaine (Sztarc, 1998). Similar data were obtained when comparing the effect of these anesthetics on ATP synthesis in the mitochondria of liver cells. The minimal inhibitory effect of ropivacaine on ATP synthesis in mitochondria explains the fairly high effectiveness of resuscitation measures in case of accidental intravascular administration of a toxic dose of this anesthetic.
There are reports of accidental intravenous administration of ropivacaine (up to 150 mg) in 6 patients when attempting to perform EA (Selander., 1997). In no case were cardiotoxic effects or other manifestations of systemic toxicity observed. It is important to note that a similar dose of bupivacaine administered intravenously would be fatal in 100% of cases.
Overall, ropivacaine is » 40% less cardiotoxic and » 30% less neurotoxic than bupivacaine.
Methods for preventing the toxic effects of MA:
- The use of techniques that reduce the likelihood of intravenous administration of LA
- Mandatory aspiration tests at all stages of manipulation
- Administration of anesthetic in small doses with step-by-step assessment of signs of systemic toxicity
- Mandatory adherence to the maximum recommended doses, especially when blocking peripheral nerves and plexuses
- If it is necessary to administer significant doses of LA into heavily vascularized areas (nerve plexus blockade), it is recommended to use drugs with a low cardiotoxic effect (ropivacaine)
- Any regional blockade must be performed in conditions that provide the availability of drugs and equipment for cardiopulmonary resuscitation
Treatment of toxic manifestations of the action of MA.
Treatment of toxic manifestations of the action of MA depends on their intensity. The usual sequence of treatment actions is as follows:
- Ensuring patency of the upper respiratory tract, inhalation of 100% oxygen (assisted ventilation in hyperventilation mode). The seizure threshold decreases against the background of metabolic acidosis and increased pCO2. In addition, acidosis enhances the cardiotoxic effect of LA.
- If seizures occur, midazolam 0.05-0.1 mg/kg or sodium thiopental 1-1.5 mg/kg
- If ineffective - succinylcholine 1-1.5 mg/kg and tracheal intubation
- In case of severe hypotension, expand the volume of infusion therapy + adrenaline 0.02-0.2 mcg/kg/min
- In case of circulatory arrest - cardiopulmonary resuscitation. In pregnant women >24 weeks' gestation, emergency caesarean section is indicated. This operation is life-saving because it eliminates compression of the inferior vena cava. In addition, uteroplacental blood flow is minimal during CPR, especially when large doses of epinephrine are used.
LITERATURE
- Butterworth J. Local anesthetics: pharmacology and clinical use. // Anesth. Analg.- 2002.-V.94 (3 Suppl S).- P.22-26.
- Carpenter R. Local anesthetic toxicity: the case for ropivacaine. // Am.J.Anesthesiol.- 1997.- V.24 (5, Suppl).- P.4-7.
- McClure J. Ropivacaine. // Br. J. Anaesth. –1996. –V.76. – P.300-307.
- Rosenberg P. Maximum recommended doses of local anaesthetics – need for new recommendations? // Highlights in Regional Anaesthesia and Pain Therapy. XI. – Special Edition World Congress on Regional Anaesthesia and Pain Therapy – Barselona, Spain, 2002. – P.30-34.
- Selander D. Accidental IV injection of ropivacaine: clinical experiences of six cases. //Regional Anesthesia. – 1997. – V.22 (2S). – P.70.
- Thomas J., Schug S. Recent advances in the pharmacokinetics of local anesthetics. // Clin.Pharmacokinet. – 1999.- V.36.- P.67-83.
- Wang R., Dangler L., Greengrass R. Update on ropivacaine. // Expert Opin. Pharmacother. – 2001.- V.2 (12).- P.2051-2063.
- Wildsmith J. Peripheral nerve block and ropivacaine. //Am. J.Anesthesiol.-1997.- V.24 (5; Suppl).- P.14-17.
Regional anesthesia and pain management. Thematic collection. Moscow-Tver 2004, pp.23-34
Preparations for local anesthesia
Local anesthetics are drugs from the group of neurotropic drugs that completely or partially block the flow of signals along nerve fibers from the site of painful manipulation or surgery to the central parts of the nervous system.
The peculiarity of the action of drugs is related to their spectrum of action. They suppress the transmission of signals along myelinated type A nerve fibers, which transmit feelings of pain, smell, and temperature. Tactile sensations are carried out through type B fibers, and anesthetics do not affect them. Therefore, when using local anesthesia, the patient does not feel pain, but feels the touch of the doctor and the surgical instrument.
Local anesthetic drugs are divided into 3 groups depending on the duration of action:
- short-acting - the effect lasts 30-50 minutes, these include Novocain;
- average duration - up to 90 minutes, these are drugs Lidocaine, Trimecaine, Ultracaine;
- long-acting – the effect lasts more than 90 minutes, typical for Bupivacaine.
Local anesthetic drugs affect the electrochemical processes of ion exchange in nerve endings. Medicines work effectively in an alkaline environment and tissues rich in lipids, which include nerves. But the analgesic effect decreases with severe tissue inflammation, which is associated with a transition of pH to the acidic side.
The effect of local anesthetics is enhanced by drugs that affect vascular tone. Therefore, they are often combined with adrenaline to prolong the effect. This allows you to reduce the dose of pain medication and avoid toxic reactions.
Articainum
Synonyms: ultracaine, ubistezin, articaine INIBSA, alfacaine, brilocaine, septonest. 4-Methyl-3-[2-propylamnopropionamido]-2-thiophenecarboxylic acid methyl ester. The first local anesthetic of the amide group, having a thiophene ring instead of a benzene ring and an additional ether group, was synthesized in 1969 by H. Rushing et al.
The drug is inferior to lidocaine in fat solubility, which makes it less likely to be absorbed into the blood and enter tissues and organs. To obtain adequate local anesthesia in dentistry, it is used in the form of a 4% solution. Articaine has the highest ratio of activity and toxicity, i.e. has a wide range of therapeutic effects, which makes it the drug of choice for children, the elderly and those with a history of liver and kidney pathology. Compared to other amide anesthetics, it has the largest plasma clearance (3.9 l/min) and the shortest half-life. T1/2 of articaine is about 20 minutes and depends on the content of the vasoconstrictor in the solution. It is not found in breast milk in clinically significant concentrations, indicating its benefits when choosing local anesthetic agents for nursing mothers. The rapidity of metabolism and excretion of articaine determines the absence of accumulation when it is re-administered during a large volume of dental care. Despite the short half-life compared to other amide local anesthetics and high plasma clearance, the drug has an average duration of action. In terms of vasodilatory activity, articaine is similar to lidocaine, which necessitates its use with vasoconstrictors. The high local anesthetic activity of the drug makes it possible to reduce the vasoconstrictor content in its solution to 1:200,000. The low toxicity of articaine allows it to be used in a 4% solution, which has high anesthetic activity. Indications for use • Infiltration anesthesia of interventions on the upper jaw and in the anterior region, including premolars, of the lower jaw.
• Conduction anesthesia. • Intraligamentary anesthesia. • Intraosseous anesthesia. In commonly used concentrations, articaine does not have a surface anesthetic effect, but is superior to lidocaine, prilocaine and mepivacaine in activity during infiltration and conduction anesthesia, allowing the effectiveness of local anesthesia in dentistry in adults to be brought closer to 95-100%. Articaine has a higher activity in inflammation compared to other anesthetics used in dental practice. Since articaine loses its activity to a lesser extent during inflammation, it is the drug of choice for tissue anesthesia in severe purulent-inflammatory processes. Cautions In dental practice, before administering a local anesthetic, it is recommended to carry out an aspiration test to prevent intravascular administration of the drug. All articaine solutions containing vasoconstrictors should be prescribed with caution to patients with cardiovascular and endocrine diseases (thyrotoxicosis, diabetes mellitus, heart defects, hypertension, etc.), as well as those receiving β-blockers, tricyclic antidepressants and MAO inhibitors. If it is necessary to use articaine during pregnancy, lactation, for cardiovascular failure, diabetes mellitus, thyrotoxicosis, the drug of choice is a 4% solution of articaine with adrenaline 1:200,000 or articaine without a vasoconstrictor. Side effects Side effects on articaine preparations are observed in 0.13-0.26% of patients. • Allergic reactions (urticaria, angioedema, anaphylactic shock). • Swelling and inflammation at the injection site. • Moderately severe disturbances of hemodynamics and heart rhythm, headache and nausea.
• With accidental intravascular administration (especially 4% articaine solution containing 1:100,000 adrenaline), ischemia of the injection zone is possible, sometimes progressing to tissue necrosis. When using infiltration methods of administering articaine preparations with adrenaline 1:100,000, changes in hemodynamic parameters in patients are unlikely. To exclude an increase in blood pressure and an increase in heart rate (pulse) when using conduction anesthesia, which may be associated with intravascular entry of the drug, an aspiration test is required before administering the entire dose of the drug. Method of administration and dosage Articaine preparations are used for infiltration and conduction anesthesia. To achieve complete anesthesia when using a 4% solution of articaine with adrenaline 1:200,000 or 1:100,000, from 0.5 to 1.8 ml is used, in some cases an additional injection of 1.0-1.8 ml may be required. Reducing the concentration of articaine solution to 2-3% reduces the effect of the local anesthetic. The maximum dose for adults is 7 mg/kg. The maximum dose for children is 5 mg/kg. It is recommended to use no more than 1/2 of the maximum allowable dose.
What is operated under local anesthesia in mammology?
The mammary glands are located superficially, they do not have muscles and large nerve trunks. Breast tissue is loosely located; in young women, glandular tissue predominates, which is replaced by fatty tissue with age. Therefore, for numerous manipulations and operations, local anesthesia can be used.
In mammology, anesthesia is used to perform invasive diagnostics, which include breast tissue biopsy. To do this, a local anesthetic is injected with a thin needle into the area of the intended puncture. After 10-15 minutes, the doctor can take breast tissue for examination without fear of causing pain to the patient.
Local infiltration anesthesia in mammology is used for small, minimally invasive operations. A woman can undergo puncture of a breast cyst after preliminary infiltration anesthesia. A similar approach can be used when removing small benign breast tumors.
In men, anesthesia is used during surgery for type 1 gynecomastia, when the size of the gland is still small. Infiltration of tissues increases hydrostatic pressure in them, thanks to which the doctor can easily separate pathological tissues from healthy ones.
Is it painful to do local infiltration anesthesia?
When performing anesthesia, a standard disposable syringe with a thin needle is used. Whether local anesthesia is painful depends on your general pain threshold. The patient feels the moment of the first puncture of the skin and a slight feeling of fullness when the drug is administered. After the medication begins to act, sensitivity disappears. The doctor checks how effective the injection is by tapping the skin. In response, there is a feeling that the injection site has become woody.
After the end of anesthesia, sensitivity gradually increases, and a slight tingling sensation may appear. If anesthesia was performed for surgery, pain in the wound area begins to bother you, which can be reduced with the help of non-steroidal anti-inflammatory drugs.
Contraindications for local anesthesia
Local infiltration anesthesia is a relatively safe method of pain relief. But to reduce risks during and after surgery, it is necessary to take into account contraindications to the use of the method. The main ones are the following:
- allergy to anesthetic - if earlier during dental treatment under local anesthesia an allergy to an anesthetic appeared, then during breast surgery the effect will repeat, and may be more pronounced, up to anaphylactic shock;
- psychomotor agitation and mental illness, reaction to the administration of an anesthetic and the surgical procedure itself can cause unpredictable behavior of the patient;
- during operations on malignant tumors - when infiltration anesthesia does not allow compliance with the ablastic rule;
- during long operations that require the use of microsurgical equipment;
- during interventions on areas of the body with a pronounced vascular network, for example, on the neck.
If local anesthesia is contraindicated, general anesthesia is preferred.
Additives to anesthetics:
1) Vasoconstrictors
Vasoconstrictors - added to increase the effectiveness of local anesthesia, as well as to slow down the entry of anesthetics into the bloodstream.
Adrenalin
Adrenaline is used most often. A relatively safe dilution of adrenaline is a concentration of 1:200,000, which can only be achieved in capsule preparations.
Norepinephrine
Norepinephrine is used less frequently as a vasoconstrictor. Norepinephrine, unlike adrenaline, is less dangerous in patients with cardiac pathology (coronary heart disease), but the risk of developing a hypertensive crisis with concomitant hypertension is higher.
Used instead of adrenaline for thyrotoxicosis and diabetes. Contraindicated in glaucoma.
Filipressin (octapressin)
Filipressin is a synthetic drug that does not have a direct effect on the heart. The effect is associated with its direct effect on the smooth muscles of blood vessels. Contraindicated during pregnancy, because may cause myometrial contractions.
Undesirable systemic effects of vasoconstrictors:
- rise in blood pressure,
- tachycardia,
- heart rhythm disturbances,
- angina attacks,
- centralization of blood circulation,
- headache.
Risk group when using vasoconstrictors
: patients with glaucoma, thyrotoxicosis, diabetes mellitus; patients taking drugs rauwolfine, thyroid hormones, tricyclic antidepressants, antidepressants - MAO inhibitors.
2) Preservatives
Parabens
(methylparaben
–
methyl 4-hydroxybenzonate, ethylparaben)
Parahydroxybenzoic acid esters (parabens) are used as preservatives, which have antibacterial and antifungal effects.
It must be remembered that parabens are included in various cosmetics, creams, toothpastes and can provoke contact dermatitis, so there is a real danger of an allergy to the local anesthetic drug.
Para-aminobenzoic acid (PABA), which is a metabolite of novocaine, has a similar structure to parabens, which can cause cross-allergic reactions. Many drugs (sulfonamides, oral antidiabetic drugs, furosemide, etc.) are derivatives of PABA. Therefore, it is not advisable to use drugs containing parabens if you have a drug allergy to the listed medications.
The presence or absence of parabens in the local anesthetic drug is indicated by the manufacturer. Parabens can cause sensitization of the body and anaphylactic shock.
3) Stabilizers
Sulfites
(sodium or potassium disulfite) are used as vasoconstrictor stabilizers. Allergy to sulfites is most common in patients with bronchial asthma (frequency - about 5%), so you should be especially careful when treating such patients. Sulfites cause edema, urticaria, bronchospasm through irritant receptors, nervous and vagal reflexes.