Diagnosis of maxillary sinusitis of odontogenic nature is an urgent problem in otorhinolaryngology, dentistry and maxillofacial surgery, since their occurrence is a consequence of the disease and treatment of the teeth and jaws [1]. In the structure of sinusitis, according to a number of researchers, the proportion of odontogenic sinusitis ranges from 14 to 24% [2, 3].
The prevalence of various forms of caries among the working population and the poor organization of dental services make this problem not only medical, but also economic and social.
X-ray computed tomography (XCT) is the best option for studying the alveolar process, nasal cavity, paranasal sinuses and surrounding soft tissues if the odontogenic nature of sinusitis is suspected. Despite the high radiation exposure, X-ray CT allows one to immediately assess the condition of the bones of the facial zone and determine their anatomical features, identify the connection with the “causal” tooth, clarify the localization of the foreign inclusion and the degree of inflammatory changes in the mucosa. In cases of prolonged inflammation in combination with canal refilling, surgical removal of the material is the only effective treatment method, for planning of which it is necessary to know the spatial anatomy [4]. These data can be obtained by performing RCT.
As sinusitis progresses, depending on the nature of the inflammation, the thickness of the adjacent bone wall changes: in acute purulent processes, osteoporosis occurs, in chronic recurrent processes - osteosclerosis, in complicated forms - osteomyelitis and destruction of the bone wall [5].
Retromaxillary (retroantral) fiber also changes as a structure intimately located to the transformed bone wall. Anatomically, it is represented by most of the pterygopalatine process of the fatty body of the cheek, located in the infratemporal space and the pterygopalatine fossa. The fat body, which is adjacent to the upper and lower jaws, serves as a conductor of inflammatory processes of odontogenic origin, which primarily develop in the jaws [6].
Magnetic resonance imaging (MRI) can detect more “subtle” changes in soft tissues. If an early stage of fungal sinusitis is suspected, it is recommended to use MRI as the method most sensitive to bone wall invasion [7]. But this method has a number of disadvantages: “unreliability” of the spatial anatomy of bone structures, difficulties in identifying the bone walls of odontogenic cysts, filling material, artifacts from metal structures, as well as a high frequency of overdiagnosis, etc., which seriously limit its use [8].
The objectives of the study were to study the variations in the fatty tissue and posterolateral bone wall of the maxillary sinus and to determine the differential diagnostic value of changes in the retromaxillary fatty tissue and the posterior bone wall of the maxillary sinus in patients with odontogenic sinusitis according to CT and MRI data.
Introduction
The maxillary sinus (MSS) is a pyramidal-shaped cavity in the upper jaw, lined with single-layer multirow ciliated epithelium.
Of course, it plays a role in improving nasal breathing, but, contrary to popular belief, according to HL Sieron et al., it is not involved in the movement of inhaled air [1]. In addition, a significant immune function of the sinus in the production of nitrogen monoxide (NO) has been proven. It plays an important role in protecting the orbit and brain in the event of a facial skull fracture, as well as in reducing the mass of the skull. The immune function of the sinus is performed in the case of adequate functioning of mucociliary transport. The functioning of the ciliated epithelium may be disrupted due to congenital disorders, entry of a foreign object into the sinus cavity and further development of the inflammatory process, dysfunction of the natural anastomosis and the formation of a vicious circle, the presence of a neoplasm, etc. The VChP is not involved in the circulation of inhaled air, so the appearance of its cavity of various dense inclusions located under the mucous membrane often does not manifest itself with clinical symptoms. Thus, after sinus lift surgery, most patients do not notice changes in nasal breathing, and osteomas of the maxillary sinus are often an accidental finding.
The sinus lift operation (or alveolar ridge augmentation) is performed on patients with insufficient alveolar ridge height for the installation of dental implants in the area of the molars and/or premolars of the upper jaw. The operation is performed by creating a trapezoidal mucoperiosteal flap in the area of the upper arch of the vestibule, forming a bone “window” in the area of the lateral part of the upper jaw. Through the “window”, the mucous membrane of the sinus bottom is peeled off from the jaw bone in the projection of the planned dental implantation. Bone material is introduced into the resulting space, the “window” is closed with a collagen membrane, the flap is placed in place, and the wound is tightly sutured [2]. As a result of surgical treatment, additional volume of the alveolar process is created by reducing the volume of the upper jaw.
According to various authors, delayed complications in the area of alveolar process augmentation in the form of sinusitis occur extremely rarely [3]. Inflammatory complications most often relate to early postoperative complications. Patients with a history of chronic rhinosinusitis, as well as thick mucous membrane of the upper jaw, are most at risk for intra- and postoperative complications.
Osteoma of the upper jaw is a rare pathology. The incidence of osteomas of the maxillary sinus among all osteomas of the paranasal sinuses is only 2% [4], among all tumors of this area - 5% [5]. Osteoma is a benign tumor originating from bone tissue. The tumor may have a predominant compact or spongy component, or they may be of a mixed nature. A feature of osteoma is uncontrolled but slow growth. Asymptomatic course of the disease is the most common option. Clinical manifestations occur after a long period of time after the start of growth of pathological tissue, when the tumor reaches a certain size and acquires a special location in relation to nearby organs and structures. Osteomas are characterized by extensive growth and are usually located on a wide or narrow base growing from unchanged bone tissue. The wide base of osteoma is not an unambiguous sign of its malignancy.
The disease can be diagnosed using radiation methods. Osteoma can be recognized on planar images, such as teleradiography in various projections, orthopantomography, and even targeted images. The techniques only allow one to see the pathological process, but do not give an idea of the extent of the spread of the tumor, its location in relation to neighboring cavities and structures. The most complete picture of the topography of sinus osteoma is provided by computed tomography - cone beam CT (CBCT) and multislice CT (MSCT). The advantage of MSCT is the ability to assess the density characteristics of a bone tumor in Hounsfield units. In addition, when using CT data in a surgical navigation station, MSCT will create less “noise” than CBCT, which will significantly increase the accuracy of intraoperative navigation [6].
Fibrous dysplasia has radiological manifestations similar to osteomas of the upper jaw. A distinctive feature of fibrous dysplasia is its repetition of the contour of the bone involved in the pathological process [7]. The growth of osteoma is usually extensive, not following the contours of anatomical structures.
Like any tumor, osteoma of the upper jaw is subject to mandatory surgical removal, primarily to obtain a morphological result. Due to the active development of endoscopic technologies these days, it has become possible to excise osteoma of the maxillary sinus using an endoscopic transnasal approach. Depending on the location of the tumor, the following approaches to the sinus are used: through the lower nasal passage, through the area of the natural anastomosis, and a combination of approaches. In case of extensive growth of the bone tumor, severe clinical manifestations and the absence of endoscopic equipment in the clinic, it is possible to use access through the anterior wall of the upper quadrant. The combination of transnasal and transoral approaches is also used in practical sinus surgery. Navigation equipment makes it possible to determine the tumor resection boundary as accurately as possible intraoperatively.
Navigation stations make it possible to visualize the tip of the navigated instrument in the lumen of the sinus as accurately as possible (according to some authors, the error is 0.6 mm [8]). The device uses electromagnetic or infrared radiation to compare the location of the instrument tip and the preoperative CBCT or MSCT data loaded into the system. In addition, some navigators allow the use of navigable drills. It must be remembered that intraoperative changes occur only in the surgical field; in the CT image in the navigator, the structures remain intact. The use of this equipment is possible only in the hands of an experienced surgeon who perfectly knows the anatomy of the maxillary sinus and is proficient in the endoscopic technique of its surgical treatment.
Why shouldn’t you treat perforation of the maxillary sinus yourself?
To date, there are no effective treatments for perforation other than surgery. An attempt to cure yourself at home using “traditional medicine” means that time will be lost and the situation will become neglected. You can start the problem before complications arise:
- the sinus cavity becomes inflamed, the infection spreads to the bone tissue, the patient begins to suffer from osteomyelitis of the upper jaw;
- inflammation penetrates into other intracranial sinuses, and there are more foci of infection;
- next to the untreated perforation, the alveolar process is weakened, as a result of which healthy teeth may fall out;
- foci of suppuration develop.
The maxillary sinus is also located in close proximity to the brain. The lack of a timely response and the development of suppuration inside the sinus is fraught with meningitis and meningoencephalitis - these are diagnoses that directly threaten life.
Clinical observation
Patient K., 39 years old, consulted an otorhinolaryngologist with complaints of discomfort in the projection of the left upper quadrant and recurrent left-sided sinusitis over the past 5 years. According to CBCT data, a formation of bone density with a heterogeneous structure, approximately 5 × 11.5 mm in size, is determined in the left upper jaw (Fig. 1A).
On examination, the face is symmetrical, without pathological rashes. Breathing through the nose is free, there is no free discharge from the nose. The mucous membrane of the nasal cavity is pale pink. Palpation in the projection of the left upper quadrant is painless.
The patient underwent surgical treatment
. Under conditions of general anesthesia, under the control of an electromagnetic navigation station and endoscopes of 0, 30, 45, 70 degrees, access to the left upper nasal sinus was performed through the lower nasal meatus. The sinus cavity is visualized. In the area of the alveolar sinus bay, the formation of bone density was visualized. Using curved diamond burs, the tumor was reduced to the base. Fragments of the formation were sent for histological examination. The operating window is closed. Lateralization of the inferior turbinate was performed. Anterior nasal tamponade with hemostatic tampons. Blood loss is minimal.
In order to prevent possible postoperative infectious and inflammatory complications, irrigation of the nasal cavity with saline solutions and the use of MestaMidin-nos nasal drops were consistently performed. This drug has a good antiseptic effect against, including multi-resistant microorganisms [9]. In addition, the product promotes faster regeneration of the nasal mucosa [10]. Places Midin-nose is easy to use, so the patient can independently perform treatment of the nasal cavity. Antibacterial therapy was not required in the postoperative period.
7 days after surgery, patient K underwent a follow-up CBCT scan (Fig. 1B, C). According to the study: surgical access in the area of the lower nasal meatus is visualized; there are no signs of a formation in the lumen of the left upper nasal passage.
The result of histological examination: intertwined bone beams and connective tissue. The formation is represented by mixed osteoma (Fig. 2).
The patient has been observed on an outpatient basis for 2 years since surgical treatment. There are no signs of osteoma growth or maxillary sinusitis.
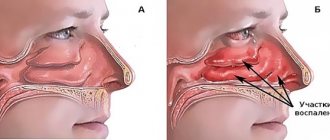
How do the paranasal sinuses work?
The nose is one of the most important human organs. This system is complex and quite fragile, which leads to frequent illnesses. But without the maxillary sinuses, normal nose function would be impossible. They perform the following functions:
- provide full breathing;
- warm and humidify the inhaled air;
- clean the inhaled air from dust and allergens;
- allow you to recognize many aromas and smells;
- form an individual timbre and other voice parameters.
The sinuses have other tasks as well. For example, they quickly respond to changes in environmental pressure (act as baroreceptor organs) and reliably protect the eyeballs, tooth roots and skull bones from injury.
conclusions
The most objective way to diagnose dense space-occupying formations of the upper jaw is computed tomography (CBCT or MSCT).
If signs of osteoma are detected in the cavity of the upper jaw, the patient must be recommended to undergo surgical excision of the formation. Morphological verification of the removed material is mandatory.
The combination of an endoscopic transnasal approach and navigation equipment in the removal of osteomas of the upper jaw is the most modern and optimal option for treating the pathology.
MestaMidin-nos has proven itself in local therapy as a means to prevent possible postoperative infectious and inflammatory complications. The use of MestaMidin-nos allows you to avoid a course of systemic antibacterial therapy.
The publication was carried out with the support of Solopharm in accordance with internal policy and current legislation of the Russian Federation.
How to cure sinusitis, sinusitis and other inflammations?
What you definitely shouldn’t do is diagnose yourself and buy medications without a prescription or doctor’s recommendations. If sinusitis is mild, then the body will quickly cope with the source of the problem and defeat the infection or virus. But if sinusitis has become chronic, special therapy is needed:
- medicines that clear the air passages;
- antibacterial drugs to eliminate infection;
- rinsing the sinuses with antibiotics;
- surgical intervention in selected cases;
- regular preventive measures.
Of course, it is better to prevent sinusitis from becoming severe. Indeed, in this case, surgical intervention cannot be avoided. Why is this scary?? Just look at the image below, the hand-drawn picture of surgical techniques will give you a chill between your shoulder blades!