What is mandibular anesthesia
Dentistry today has a large selection of types of pain relief. This opens up wide opportunities for the dental surgeon, especially in terms of treating young patients. Mandibular anesthesia is a conduction-type local anesthesia. Provodnikova - temporary blocking of the transmission of nerve impulses through a large nerve trunk. It is used when there is a need for an absolute block of pain while keeping the patient fully conscious.
Mandibular anesthesia is required if surgical intervention on the lower jaw is planned. An unpleasant moment of injection is a short-term feeling of fullness, pain and burning in the injection area. This sensation lasts a few seconds and is comparable to a prick when blood is drawn from a vein.
Apodactyl mandibular anesthesia according to A. E. Verlotsky
It is performed similarly to the previous anesthesia. Injection site : the outer part of the pterygomaxillary fold in the middle of the distance between the chewing surfaces of the upper and lower molars (in the absence of molars - in the middle of the distance between the posterior ends of the alveolar processes of the lower and upper jaws). If the width of the pterygomaxillary fold is significant, the needle is inserted in its middle. If this fold is narrow and located near the mucous membrane of the cheek, the needle is inserted into its inner edge (Fig. 97).
Rice. 97. Apodactyl mandibular anesthesia according to A.E. Verlotsky (V.I. Zausaev et al., 1981)
Note : apodactylic methods of mandibular anesthesia are not very common in the USA and Europe, since dentists consider this technique to be inaccurate. Anesthesia zone for mandibular anesthesia : all teeth of the corresponding side of the jaw, alveolar process, gums on the vestibular and lingual sides, mucous membrane of the floor of the mouth, anterior 2/3 of the tongue, half of the lower lip, skin of the chin on the side of anesthesia. On the vestibular side, the gums from the middle of the second premolar to the middle of the second molar are innervated by the buccal nerve. To anesthetize them, you need to turn off the buccal nerve or additionally inject 0.3-0.5 ml of anesthetic into the transitional fold near the corresponding tooth. Anesthesia of the incisors and canines is incomplete due to the anastomoses of the opposite side (Fig. 98 A).
Rice. 98. A - zone of anesthesia during mandibular anesthesia . B - zone of anesthesia during torusal anesthesia (explanation in the text)
Duration of anesthesia : from 1.2-2 to 4-6 hours (when using a medium-acting anesthetic (lidocaine), anesthesia lasts an average of 2 hours, when using a strong anesthetic (articaine) - 4-6 hours. Application : for long-term, traumatic interventions (operations) on the teeth and in the area of the alveolar process of the lower jaw, during inflammatory processes (periostitis, osteomyelitis), during interventions on the lower molars. COMPLICATIONS :
1. Contracture of the lower jaw. Occurs when a low-quality anesthetic solution is administered, when the pterygomaxillary muscle is injured (insertion of a needle medial to the pterygomaxillary fold, repeated, 2-5 times, repetition of anesthesia with subsequent injury to the muscle, periosteum and bone). 2. Damage to blood vessels with the formation of a hematoma, entry of anesthetic into the bloodstream, injury to the inferior alveolar nerve. 3. Fracture of the needle in the cannula area. Prevention of complications Mandatory aspiration test. Do not use low-quality (little-known companies) and short needles, use needles 41.5-50 mm long, then the needle fragment can be easily grabbed with a tool (tweezers, clamp) and immediately removed from the soft tissues.
Methods of mandibular anesthesia
There are two common methods of performing mandibular anesthesia. The first method is intraoral and is carried out according to the modification of Gou-Gates and Akinosi. The second method is extraoral, carried out in three ways - mandibular, retromaxillary or subzygomatic.
From a technical point of view, there are the apodactyl (without palpation) method, the finger method, as well as modifications of Go-Gates and Akinosi.
Mandibular anesthesia using the apodactyl technique is performed most often. In the area of the required tooth in the lower jaw, infiltration anesthesia is first performed to anesthetize the buccal space. Then, with the maximum opening of the mouth, the patient feels the line between the lower and middle third of the pterygomandibular fold in its lateral slope. This is the place where the needle is inserted. First, it is inserted all the way into the bone, then it is turned in the opposite direction and one milliliter is injected at the level of the incisors. A total of 2 to 2.5 ml of anesthetic is injected.
With the finger method, an injection of an anesthetic solution in an amount of 3-4 ml is carried out in the area of the retromolar space and temporal ridge. The anesthetic is administered, as with the apodactylic technique, in two stages with a change in the position of the needle.
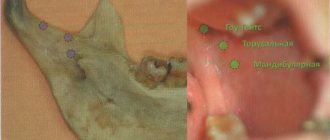
The Go-Gates modification involves anesthesia of three branches of the mandibular nerve at once. For this purpose, an injection of an anesthetic solution is administered in the area of the condylar process of the mandible.
If the patient has limited ability to open his mouth, mandibular anesthesia is performed using the Akinosi method. The patient does not open his mouth and closes his teeth. The injection is placed at the border of the buccal mucosa and the retromolar region of the upper jaw.
To perform mandibular anesthesia, the doctor must be highly qualified and have deep anatomical knowledge of the structure of the lower jaw.
Apodactyl mandibular anesthesia (well-known method)
When performing anesthesia using the apodactylic method, the main landmark is the pterygomaxillary fold. It is located in the middle of the temporal ridge and can be wide, narrow, or have a normal (medium) transverse size. 1. The patient opens his mouth as wide as possible. Using a dental mirror, held in the left hand, move the corner of the mouth and the cheek in the middle. Injection site : behind the lower molars the pterygomaxillary fold is visible, laterally (behind this fold) there is a groove, which is divided into three equal parts and an injection is made in front of it between the upper and middle thirds of its length 10 mm above the chewing surface of the lower molars (Fig. 96) . 2. The syringe is placed on the premolars or on the first lower molar, the needle is directed perpendicular to the plane of the lower jaw branch; for this, the syringe barrel must be used to move the corner of the mouth posteriorly. 3. The needle is deepened into the soft tissue by 20-25 mm until it touches the bone. An aspiration test is performed and 1.5-2 ml of anesthetic is injected. Pain relief occurs within 5-10 minutes.
Rice. 96. Apodactyl mandibular anesthesia (N. Evers, G. Haegerstam, 1990): - the cheek is moved to the side with a dental mirror; — the syringe cylinder pulls the corner of the mouth posteriorly, the syringe is located at the level of the lower molars of the opposite side; — there is a mark on the cannula from the side of the needle tip (the cut of the needle is directed towards the bone). DISADVANTAGES: anesthesia is performed with a short needle 25 mm long. If the needle is fractured in the cannula area, the fragment is difficult to remove from the soft tissue (surgery may have to be used)
Possible complications
Mandibular anesthesia in rare cases leads to the development of complications. One of them is numbness of the tissues of the pharynx with subsequent limitation of movements of the lower jaw. Physiotherapy, mechanical therapy and administration of medicinal solutions are prescribed as treatment. A hematoma can occur as a result of damage to a vessel. If it does not resolve on its own, a puncture may be required. When a nerve is damaged, neuritis sometimes develops, the treatment of which requires physiotherapeutic procedures using heating elements or electric current. A very rare complication is temporary muscle paralysis as a result of medical error. If the injection technique is violated, the needle rarely breaks off and gets stuck in soft or tendon tissue. In such cases, surgical removal is used after an X-ray examination. If the needle does not cause concern to the patient and has grown into the tissue, it does not need to be removed.
Anesthesia of the inferior alveolar nerve at the mandibular foramen
To perform anesthesia correctly, you need to know where the inferior socket opening is located. By the way, the location of the lower hole in adults and children, as well as citizens of retirement age, varies somewhat. In the former, it covers the inner part of the ramus of the lower jaw, comparable to the chewing region of the lower molars, and in the latter, it is slightly lower. The accessibility of the inferior alveolar nerve for drug anesthesia with solutions is due to its placement in front of the entrance to the bone canal, located in the bone groove. The area of the bone groove consists of loose fiber, which allows the injected anesthetic solution to be evenly distributed.
Anesthesia is carried out using two methods that differ from each other in the type of access to the anesthetized area - extraoral and intraoral. The anesthesia affects not only the area of the lower jaw where interventions are performed, but also its alveolar part, as well as the gums, mucous membrane and skin of the lower lip, the sublingual area, the skin of the sublingual part and most of the tongue.
The essence of the intraoral approach is as follows: first, a palpation determination of the injection site is carried out, located slightly further than the molar fossa and the temporal crest. The injection is given with the mouth wide open. In this case, the needle is located inside the temporal crest 0.7-1.0 cm higher than the chewing surface of the molars in order to cover their outer and posterior parts up to contact with the bone. The inferior alveolar nerve is blocked by moving the needle inward a couple of centimeters to the bony groove and injecting the rest of the anesthetic into it.
Anesthesia using the apodactyl method involves selecting the pterygomaxillary fold as a landmark, which is inward from the temporal crest. The injection is also carried out with the mouth wide open and the position of the needle identical to the one described above, which is inserted into the area of the outer slope of the pterygomaxillary fold approximately in the middle of the distance between the chewing surface of the upper and lower molars. Then it is advanced 1.5-2 cm deep, reaching the bone. An anesthetic is administered to block the inferior alveolar and lingual nerves.
Both methods of intraoral access to anesthesia have an analgesic effect after 3-5 minutes, maintaining the effect for up to an hour and a half.
Among the intraoral methods of anesthesia, there are two main ones - the Gow-Gates method and the Vazirani-Akinosi method. The most effective is the Gou-Gates method, in which it is possible to block the inferior alveolar nerve, and with it the lingual, auriculotemporal, mylohyoid, and buccal nerves. The sequence of manipulations with this method is as follows: a section of the lateral edge of the pterygomaxillary recess is selected as the injection site, and the injection itself is made with the mouth wide open into the mucous membrane under the medial palatal tubercle in the area of the second molar of the upper jaw. The trajectory of the needle movement is to the tragus of the ear or the neck of the condylar process to the bone stop at a depth of 2.5 cm. The patient’s mouth does not close for another 2-3 minutes. You can begin operational actions in 8-10 minutes.
The immobilized lower jaw prompts the specialist to use the Vazirani-Akinosi method, which is activated when the teeth are closed.
The anesthetic effect in both cases occurs within 5-10 minutes, but the Vazirani-Akinosi method requires special care to avoid deepening the needle into the mucous membrane along the medial surface of the mandibular ramus. The consequences of such an oversight can be disastrous - damage to the branches of the facial nerve must not be allowed.
Recommendations after the event
Any type of anesthesia is stress for the body, which must be minimized. Immediately after applying anesthesia, you must rise from the dental chair carefully to avoid dizziness. After pain relief, you must avoid drinking hot and alcoholic drinks. Do not massage the injection area or eat hot food. It is necessary to rinse your mouth with soda-salt or any other solution as prescribed by your doctor several times a day. It is better to sleep on the side opposite to the injection.
Contraindications for mandibular anesthesia
Mandibular anesthesia is not used for liver diseases, which is associated with a large load on it. Novocaine is the only anesthetic that is not subject to this contraindication. If a major operation is required, local anesthesia is not suitable due to the need to administer a large amount of it. Epilepsy and mental illness, as well as problems of the cardiovascular system are contraindications to mandibular anesthesia. During pregnancy, it is necessary to weigh the risk to the fetus when exposed to drugs. For blood diseases and bronchial asthma, mandibular anesthesia is not performed. Contraindications to anesthesia must be considered individually; sometimes their list can be shortened or, conversely, expanded at the discretion of the attending physician.