Dental clinic No. 2
In order to always anticipate surprises, the doctor must be prepared to expand access to the dental cavity to facilitate the preparation of complex root canals and carefully examine the floor of the tooth cavity to look for such anatomical variations.
Endodontic dogma is that careful cavity and root canal preparation and obturation is the key to successful canal therapy. Endodontic preparation can be divided into cavity preparation (coronal preparation) and root canal preparation (radicular preparation). Transferring the principles of preparation of carious cavities according to Black in relation to endodontics, the following endodontic principles of preparation can be distinguished: creation of external, comfortable, retention (holding) and resistant forms. A complete preparation along the entire length of the tooth is the external form. In turn, the external shape can be modified for a comfortable shape to accommodate anatomy, canal curves and instrumentation. In some endodontic techniques, the canal can be prepared with slight retention of the first gutta-percha point (retention form). But the most important is the resistant form, in which the so-called “apical stop” is prepared in the apical section, a barrier that protects the tissues of the apical periodontium from the removal of the filling material and irrigating solution beyond the apex and creates a limit for the compaction of gutta-percha in the canal (Fig. 1).
| pic 1 |
Basic tools for preparing a tooth cavity. For trephination of an intact tooth crown, Ingle JI suggests using a cone-shaped fissure bur with a working rounded top for a turbine tip (Fig. 2 B). It is first directed at a right angle in the long axis of the tooth to remove only the enamel. Then it should be located parallel to the longitudinal axis of the tooth (Fig. 2 C, D). The roof of the tooth is removed using a low-speed tip with a round bur (Fig. 2 E, F) No. 2, 4 less often No. 6 of regular length (9 mm) for molars and premolars or surgical length (14 mm) for incisors and canines. The protrusion (“shoulder”) inside the cavity of the anterior teeth, which prevents the direct passage of the endodontic instrument into the root canal, is eliminated using a long, conical diamond bur on a turbine drill (Fig. 2 G). The remaining pulp from the pulp chamber is removed using a spherical bur No. 1 or 2 (Fig. 2 H).
| pic 2 |
It is necessary to remember the following axioms of the structure of the coronal cavity of the tooth and root canals when searching for root canal orifices (Ingle JI). 1. The two root canal orifices of the first maxillary premolars are located further buccal and lingually than is usually realized (Fig. 3 A). 2. The orifices of the mesiobuccal canals of the upper and lower molars are located under the mesiobuccal cusps, and the external shape should often be more expanded due to these cusps (Fig. 3 B, C). 3. The mouth of the palatal canal in the upper molars is located not so far to the palatal wall of the tooth cavity, but in the center of the medial half of the tooth (Fig. 3 B). 4. The orifice of the distal-buccal canal of the upper molars is not located so distally-buccally, but almost directly to the buccal side of the palatal canal (Fig. 3 B). 5. The orifice of the distal canal in mandibular molars is not so distally located, but in fact almost exactly in the center of the tooth (Fig. 3 C, E). 6. The orifice of the mesial-lingual canal of the lower molars is not so far mesial-lingual, but in fact directly buccally from the orifice of the distal canal (Fig. 3 B). 7. Certain anatomical variations that occur quite often: The mesial buccal root of the maxillary first molar often (up to 95% [4]) has an additional mesiopalatal canal located exactly oral to the orifice of the main canal. The mouth of the additional channel is located in the groove, which forms the mouth of the main channel like a “comma tail”. This entire groove should be examined to locate the mouth of the accessory canal (Fig. 3 B). The lower second molar often has a common mesial orifice, which divides approximately 1 mm below the floor of the dental cavity into mesial buccal and mesial lingual canals (Fig. 3 D). The lower first and second molars may have two distal canals with separate orifices or a common one. orifice, like the previously described medial canals (Fig. 3 E). The mandibular first premolar often has a second canal that branches off from the main canal buccally or lingually a few millimeters below the floor of the dental cavity (Fig. 3 E). The lower incisors and canines often have two canals. The medial lingual canal is hidden under the internal protrusion (“shoulder”), which corresponds to the lingual girdle. This protrusion should be removed with a #2 long shank round bur or finishing diamond cone bur to allow proper exploration of the root canals (Figure 3 G).
| pic 3 |
Table 1. Degree of deviation of teeth from the central axis
When preparing a tooth cavity, it is necessary to take into account the degree of deviation of the tooth from the central axis in the vestibulo-oral and medio-distal projections (Table 1). The upper incisors and canines are inclined palatally by 29°, the lower incisors are inclined lingually by 20°. The lateral lower and upper incisors are deviated medially at 17 and 16? respectively. If the doctor does not know about these deviations or ignores them, then he can make a perforation and a ledge on the walls of the tooth cavity (Fig. 4. A, B, C)
| pic 4 |
Table 2. Incidence (%) of root canals.
For successful endodontic treatment, it is also extremely important to know the variations in the number of root canals in order to avoid the error of missing a canal. Although back in 1921, Hess W., studying 513 teeth, indicated that four canals were found in 54% of the first molar, this fact was ignored. F. Pineda, J. Cutler (1972), studying the medial buccal roots of the first molars, found that in 39% of cases this root has one canal, in 61% - 2 canals. Later studies (J.K. Kalild and D.D. Peter, 1990) showed that in a study of 51 medial buccal roots of the upper first molars, a two-canal variant of the structure was identified in 95% of cases. Table 2 summarizes information from various authors about the frequency of occurrence of additional channels. As follows from this table, in the lower incisors, canines and premolars it is always necessary to look for the second canal, and the first upper molar should be considered a four-canal. Lower premolars can be extremely difficult teeth to treat endodontically. Two narrow canals are usually located vestibulo-orally; division into two roots can occur in the apical third. At higher magnifications, it is often possible to view more complex anatomy. The dentist’s knowledge of the anatomy of the tooth cavity and root canals is an important part of endodontic treatment, guaranteeing the success of the treatment and avoiding errors and complications.
Author: Trigolos N.N.
Root canal instrumentation techniques in different age groups: a comprehensive narrative review
Introduction
As the world population grows, there is both an increase in life expectancy and a decrease in tooth loss. Because root canal treatment is performed on patients of all ages, clinicians should be aware of differences in root canal system morphology and dentin structure depending on patient age.
It is known that it is almost impossible to create guidelines or instrument calibers that would guarantee adequate root canal preparation in any age group. However, due to differences in canal morphology and dentin structure, as well as the use of different endodontic instruments and techniques available today, the clinician may use different methods to instrument the root canal system. Meanwhile, various tools—especially canal shaping files made from different heat-treated alloys with different geometric characteristics—are reported to have distinctive mechanical properties and resulting positive processing results. The choice of instruments may lead to inadequate clinical results in certain cases, depending on the properties of the instrument and the clinical condition of the patient, including age. Therefore, the purpose of this article is to review age-specific clinical guidelines for root canal instrumentation techniques through a literature search and review.
Review and search of literature
An electronic literature search was conducted, including MEDLINE (Ovid), PubMed, and Web of Science databases. The search used dictionary terms and arbitrary phrases, such as: “root canal treatment depending on age”, “root canal instrumentation depending on age”, “chemomechanical preparation depending on age”, “clinical recommendations in endodontics depending by age”, “toolkit for root canal treatment at different ages”, “geriatric root canal treatment” and “childhood root canal treatment”. However, a review of the literature revealed a lack of studies with practical clinical recommendations when selecting appropriate instruments for age-related root canal treatment.
Therefore, a comprehensive review of canal morphology, dentin structural characteristics, and endodontic outcomes in different age groups was taken from articles that were published from 1925 to 2018, rather than a systematic review. Previous studies have used different approaches to classify age-related morphological and structural changes, either based on statistics (to ensure a larger sample size) or without explanation of the classification. This review categorizes age differences into the following age groups: persons aged 20 years or younger, 21 to 40 years, and 41 years or older.
Morphology of root canals depending on age
- Contour and cross-sectional diameter of the channel
Differentiation of the root canal system due to the deposition of secondary dentin is an age-related process. With age, the pulp cavity usually decreases in size (Fig. 1).
Rice. 1. Panoramic radiographs showing the size of the pulp chamber and root canal depending on age. (A) Persons under 20 years of age (13 years), (B) persons between 20 and 40 years of age (39 years), (C) persons over 40 years of age (64 years). Image (A) shows the large pulp chamber and the direct direction to the canal opening. Image (B) shows the denticulate area and the direction at an angle to the canal orifice. Image (C) shows a small area of the pulp chamber and sclerotic canals.
Typically, people under the age of 20 have roots with one large root canal (mostly oval). Median mesial canals in mandibular molars are found mainly in individuals under 21 years of age. Individuals between the ages of 20 and 40 have several separate canals in one root. The number of root canals was found to increase mainly in the maxillary and mandibular second premolars, the distal root of the mandibular first molars, and the mandibular incisors. In patients over 35 years of age, more round canals were found in the mandibular second molar, while in those under 35 years of age, more oval canals were found.
The C-shaped configuration (type III) is more common in mandibular molars in individuals under the age of 40. In a study using cone beam computed tomography, patients younger than 42 years were 4 times more likely to encounter a mesial canal than patients older than 42 years. In people over 40 years of age, the deposition of secondary dentin leads to a decrease in the diameter of the canal and the disappearance of additional canals. Fewer canals were found in individuals aged 51–70 years. For example, in this age group, the absence of the second mesiobuccal canal in the maxillary molars was observed.
- Isthmuses
The incidence of canal isthmuses appears to be related to age. People under 20 years of age have wide and oval canals without isthmuses in the early stages of root development. In people aged 20 to 40 years, the deposition of secondary dentin in the mesiodistal direction leads to the formation of 2 canals with an isthmus. Up to 81% of mesial roots of mandibular first molars in individuals aged 20-39 years have isthmuses, especially at a distance of 4-6 mm from the apex. In persons over 40 years of age, the extent and number of isthmuses are significantly reduced, and the canal is completely separated. In people over 50 years of age, the incidence of isthmuses was 16.7%, and only 24% of people over 60 years of age had isthmuses in the mesial roots of mandibular molars. The ratio of partial isthmuses to complete isthmuses increases with age. Figure 2 shows isthmus characteristics in different age groups with cone beam computed tomography images.
Rice. 2. Cone beam computed tomography: three images of the mandibular first molar showing isthmus characteristics in different age groups. (A) Persons under 20 years of age (18 years): wide canal without isthmus, (B) persons 20 to 40 years of age (38 years): isthmus in the mesial root, (C) persons 40 years of age or older (62 years) : sclerotic mesial canals without isthmus, similar to one canal.
Age-related changes in dentin structure
With age, normal dentin undergoes physiological changes and turns into transparent (sclerosed) dentin. As the tooth matures, peritubular dentin becomes more mineralized and a decrease in the average number of dentinal tubules is observed. The process of mineralization and dentin sclerosis lead to narrowing of the tubules. In some cases, this process can lead to complete obliteration of the dentinal tubules. Mineralization begins in the third decade of life in the apical zone and develops coronally with age.
The penetration of bacteria into dentinal tubules may be a determining factor in their virulence in the root canal environment. Microbial diversity and microbial load are higher in young people and decrease with age. This decrease may be due to mineralization of the tubules, as well as a decrease in the space of the pulp cavity, isthmuses and accessory canals. Dentinal tubules typically have a larger diameter than the average diameter of Enterococcus faecalis (E. faecalis) cells by approximately 0.8–1 nm. However, due to age-related mineralization of the tubules in old age, the depth of penetration of E. faecalis into dentin through sclerotic or obliterated tubules decreases. On average, bacteria penetrate 65 microns less deeply in people aged 60–77 years than in people aged 18–24 years.
With age, the water content of dentin decreases and collagen modifications, such as cross-linking, increase. Because of these age-related changes, resistance to dental damage decreases in older adults, but significant reductions in dentin strength and fracture strength result in an increased incidence of vertical root fracture (VRF). VRFs are most common in posterior teeth in patients between 40 and 60 years of age. In addition, the growth rate of vertical cracks in “old” dehydrated dentin is 100 times higher than in “young” hydrated dentin. Pre-existing dentinal microcracks in endodontically untreated roots become more common with age (8.3% in persons over 40 years of age, 3.7% in persons over 20–39 years of age). In contrast, in individuals under 20 years of age, the dentin walls are thin, which can lead to coronal or root fractures of the tooth under normal functional stress.
Results depending on age
Data on the effect of patient age on the results of endodontic treatment are contradictory. Some studies reported that age had no statistically significant effect on results, while others stated that patient age significantly affected results. Some studies have shown that treatment in older patients had a higher success rate than in younger patients, while other researchers have found better results in younger patients and have demonstrated that age is a risk factor for complications. For example, older patients are 1.4 times more likely to have teeth removed after root canal treatment. The rate of subsequent removal increases by 1–2% each decade until it reaches a plateau after age 60.
These better results in older people can be explained by the gradual reduction of the pulp space, the disappearance of additional canals and isthmuses and the narrowing of the dentinal tubules up to complete obliteration. These changes limit the volume available for infection, which ensures adequate cleaning of the canal, as well as its formation and medicinal treatment. Reports of better results in younger adults may be explained by the increased prevalence of apical periodontitis with age, which is associated with a lower likelihood of successful endodontic treatment. Another explanation could be that older people have slower and less efficient healing processes or longer healing times. Immunological changes that occur due to aging include changes in pulp cells expressing macrophage-associated antigens. Aging is associated with low levels of expression of genes encoding transcription regulators and high levels of expression of genes involved in apoptolytic processes.
In addition, systemic diseases are more common in older age groups, and it has been reported that some systemic diseases may be associated with endodontic treatment outcome. Diabetes (non-insulin-dependent or insulin-dependent) or an impaired nonspecific immune response leads to decreased success of endodontic treatment in patients with preoperative periradicular lesions.
Table 1 shows the characteristics of canal morphology and dentin structure in different age groups, including the contour and cross-sectional diameter of the canal, the presence and characteristics of isthmuses, accessory canals, the number and diameter of dentinal tubules, and sclerotic dentin. Taken together, these age-related changes suggest that clinicians may choose different clinical approaches for different age groups.
Table 1. Characteristics of the canal morphology and dentin structure in different age groups.
Possible clinical suggestions
Within the limitations of the studies that were reviewed, the following possible clinical recommendations for root canal instrumentation can be made. For persons over 20 years of age, the recommendations are as follows. Large channels do not require additional expansion. Scraping instruments may be preferred to clear the root canal wall of biofilm while simultaneously activating the irrigation solution. Possible tools: Self-Adapting File (SAF; ReDent, Ra'anana, Israel) and XP-Endo Finisher (FKG Dentaire, La Chaux-de-Fonds, Switzerland). These systems are effective in cleaning a relatively large and oval canal lumen with a cleaning action while constantly changing the irrigant for SAF or eccentric movements of memory-controlled instruments such as the XP-Endo Finisher.
For persons aged 20 to 40 years, the following recommendations exist. The channels are generally open and difficulties in creating a carpet are rare. In these root canal systems, conventional nickel titanium (NiTi) rotary systems can be used to shape the canal to size #30–#35 followed by sodium hypochlorite activation. Possible instruments: ProTaper Next (Dentsply Sirona, Ballaigues, Switzerland), XP-Shaper (FKG Dentaire, La Chaux-de-Fonds, Switzerland) and 2Shape (MicroMega, Besançon, France). The use of scraping instruments in this age group may be considered in oval canals.
For people who are 40 years of age or older, the recommendations are as follows. In these root canal systems, after using stainless steel hand K-files (#06, #08 and #10), the NiTi system can be used to create a carpet. Possible tools include G-File (MicroMega), PathFile (Dentsply Sirona), OneG (MicroMega), ProGlider (Dentsply Sirona), Scout RaCe and Race ISO 10 (FKG Dentaire). Thereafter, expansion of the apical diameter of the root canal to size No. 30 or No. 35 is preferably carried out using NiTi instruments, which place less stress on the dentin. Possible instruments for this purpose are instruments with a smaller cross-sectional area (MTwo [VDW, Munich, Germany], Race [FKG Dentaire], ProFile, 2Shape), instruments with a smaller taper (0.02 and 0.04) (Race, ProFile ) ) and made from flexible NiTi (memory controlled file), such as HyFlex (Coltene/Whaledent, Inc, Cuyahoga Falls, OH, USA) and Typhoon (Clinician's Choice Dental Products, New Milford, CT, USA).
Table 2 presents the proposed algorithm for root canal instrumentation in different age groups. The current suggestions are based on available evidence and reflect the limitations of the studies that were included in the review. However, no single algorithm fits all teeth. The clinician may encounter inconsistencies between chronological age and biological age. Pathological or iatrogenic factors can change the contour and cross-sectional diameter of the canal. These factors include carious lesions or extensive restorations, attrition or attrition, occlusal trauma, periodontal disease and treatment, and orthodontic treatment. The irritants that each tooth encounters during its life must be taken into account due to the possible rapid increase in reaction and dentin deposition. In contrast, pulp necrosis in younger patients due to trauma or caries can lead to the formation of wider canals with thin dentin walls as these patients get older.
Table 2. Algorithm for root canal instrumentation in different age groups.
The contents of this review do not necessarily support any specific technique for specific clinical situations in patients of various age groups and root canal conditions. However, it may be generally acceptable to emphasize the importance of chemomechanical preparation, which always improves canal clearance through shaping and activated irrigation, regardless of the patient's age and canal condition. Correct assessment of root canal morphology, coupled with an adequate understanding of the influence of age on these characteristics, can help the clinician select the most appropriate instrumentation technique and irrigation activation.
conclusions
The current review examines age-related differences in canal morphology, dentin structural characteristics, and endodontic outcomes. Depending on age, clinical recommendations for instrumentation should ideally be based on a systematic review of randomized controlled trials, taking into account the quality of evidence and patients' values, preferences and financial resources. However, no studies suitable for this purpose have been conducted. Thus, the present article is the first attempt to interpret age-related morphological and structural changes and make practical clinical suggestions within the limitations of existing studies.
A systematic review is a comprehensive method of finding relevant studies on a specific topic, and then the identified studies are assessed and summarized according to a predetermined and explicit method. In contrast, narrative review is a traditional method of peer review. This method is subjective and there are no formal rules for selecting studies or standard statistical methods for pooling studies. Therefore, when reading and evaluating a narrative review, readers should keep in mind that the author's bias may or may not be present.
An additional limitation of these proposed clinical offerings is that the aforementioned tools are not available to all clinicians due to local market conditions and financial resources. Future research should examine the influence of patient age on other aspects of root canal treatment (eg, access cavity preparation, irrigation techniques, and obturation techniques). It can be concluded that the clinician's awareness of age-related differences in root canal morphology and dentin characteristics may influence the choice of instruments for root canal treatment.
Source : Restorative Dentistry & Endodontics
Translation by Tatiana Chuiko for the BELODENT.ORG portal
Similar articles:
Ibrahim El Naggar
Huge perforation
Cancellation
The physician must be able to assess the current situation from diagnosis, treatment to prognosis, and be able to cope with various clinical surprises.
Ibrahim El Naggar Read Viresh Chopra
Endodontic treatment of the second lower molar
Cancellation
The article presents a case of irreversible pulpitis with symptomatic apical periodontitis of the mandibular second molar.
Viresh Chopra Read Daniel Flynn
Repeated endodontic root canal treatment: pros and cons
Withdrawal
Repeat root canal treatment is a predictable endodontic procedure. In the past, when telling patients about the prospects of retreatment, doctors often pointed to the possibility of failure.
Daniel Flynn Read L. Stephen Buchanan
Obturation using the continuous wave method for greater precision of the procedure
Cancel
I invented the Continuous Wave Obturation Technique (CWOT) in 1986 and continued through the winter of 1988-1989. I used it in combination with the Touch'n Heat device (SybronEndo).
L. Stephen Buchanan Read Mohamad Zaafrany
MB2: The Most Famous Missed Channel
Cancellation
Missed canal is one of the main causes of endodontic failure. During root canal treatment, MB2 is most often not found among the maxillary molars.
Mohamad Zaafrany Read
Calogero Bugea
Continuous wave condensation of gutta-percha
Cancellation
In 1987, Dr. Stephen Buchanan developed the continuous wave condensation technique for obturation of gutta-percha to simplify the Schilder technique of vertical condensation of heated gutta-percha.
Calogero Bugea Read S.S. Grigoriev
Evaluation of the quality of root canal filling with gutta-percha using optical microscopy and cone-beam computed tomography
Cancellation
Despite significant advances in clinical dentistry in the prevention and treatment of caries, complicated caries is a very common pathology of hard dental tissues.
S.S. Grigoriev Read CAE STANDARDS OF PRACTICE
Classification of clinical cases according to the level of complexity and risks
Cancel CAE STANDARDS OF PRACTICE Read Calogero Bugea
Bioceramics and adhesion: root canal preparation for fiberglass using the single cone technique
Cancellation
One of the controversial topics in endodontics and restorative dentistry is the relationship between the properties of endodontic sealers and the concept of adhesion.
Calogero Bugea Read Garima Poddar
Endodontic treatment of the lower first molar with a denticulate obliterating the bottom of the pulp chamber. Clinical case
Cancellation
This article describes a clinical case of endodontic treatment of a lower first molar with a denticulate obliterating the bottom of the pulp chamber.
Garima Poddar Read Mohamed Milad Ganawo
Clinical case of treatment of internal root resorption of the upper central incisor
Cancellation
This article describes a clinical case of internal resorption that began in the pulp and resulted in loss of dentin and possibly cementum from the root of tooth 2.1.
Mohamed Milad Ganawo Read Ahmed Shawky
Regenerative endodontics: a sustainable solution
Withdrawal
This case report describes successful regenerative endodontic treatment with a 42-month follow-up.
Ahmed Shawky Read
- ‹
- 1
Pulpitis: all about pulp, dental canals and their treatment
In general, caries is not so much a disease as a process. You can't just pick it up and get rid of it. Treatment of a hole in a tooth can be delayed for a long time - in most cases there is either no pain at all, or the patient is not very bothered by it. You should not get carried away with delaying treatment of teeth with caries, otherwise you can wait for pulpitis.
Pulpitis is no longer as simple as caries. Pulpitis hurts. The pain from it is acute, lasts a long time, arises from anything. Pulpitis does not go away for long without treatment, so at this stage, as a rule, the patient still consults a doctor. Compared to conventional filling of a carious hole, treatment of pulpitis is hellish torture for both the patient and the doctor. Let's find out why.
What it is?
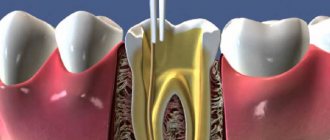
Pulpitis is inflammation of the dental pulp. The pulp is the soft connective tissue inside the tooth. The anatomy of the tooth is presented in Figure 1. Under the hard layers - enamel and dentin - there is a jelly-like amorphous mass with a variety of cells, vessels and nerves.
The most important cells of the pulp are odontoblasts. They communicate with dentine and provide it with the necessary “building” substances. The pulp contains various immune cells: lymphocytes, plasma cells and mast cells.
The pulp has temperature, mechanical and pain receptors, but it converts all signals from the outside into pain. This happens when the pulp is exposed. This can happen with advanced deep caries, when the cavity reaches the “roof” and “falls” into the pulp chamber. Bacteria get there; the disease develops. But this is not the only way inflammation occurs. The pulp can be damaged mechanically, due to tooth trauma or unsuccessful treatment.
You cannot blame the pulp alone for toothache. Normally, enamel and dentin do not transmit irritation to it, but with caries the situation is different. The enamel is destroyed, the cavity reaches the dentin, and dentin is a fairly permeable tissue. It has special tubules with liquid. The movement of this fluid is perceived by the pulp as pain. Therefore, caries can be painful, but the discomfort does not last long. They pass immediately after the cessation of the stimulus.
The pulp occupies not only the crown of the tooth. Teeth have roots, and roots have root canals. They are also filled with pulp. It is this circumstance that complicates the treatment of pulpitis. It is worth noting that not every pulpitis “gets” to the canals. In this case, the treatment method is called vital amputation. There are vital (on living teeth) and devital (after “killing” the pulp) methods of treatment. Both types are divided into amputation (removal of only the coronal pulp) and extirpation (complete removal of the pulp). More details in Figures 2 and 3. Most often, doctors have to use vital extirpation. Devital techniques are currently rarely used.
Classification of pulpitis
Pulpitis is described according to various characteristics. One condition can be characterized from several positions.
- According to the course of the disease: acute, chronic, exacerbation of chronic.
- According to morphology: pulp hyperemia (deep caries), exudative (serous and purulent), alterative, proliferative.
- By origin: microbial, chemical, toxic, thermal, traumatic, hematogenous, lymphogenous and iatrogenic.
Course of the disease
The clinic of pulpitis changes with the progression of the disease. The very initial stage is pulp hyperemia (see Figure 4). According to the domestic classification, it is classified as deep caries. With hyperemia, the pulp is “irritated” and sensitive, but the pain passes quickly and does not occur spontaneously. At this stage there is no need to remove the pulp as it is viable and intact. It is treated similarly to caries: softened pathological tissue is excised with a bur to healthy layers, a medicine (usually calcium hydroxide) is placed at the bottom of the cavity and the tooth is filled with a filling. Gradually, caries approaches the center of the tooth - its pulp. The pulp becomes infected and becomes inflamed. At this stage, the clinical picture is quite typical: paroxysmal spontaneous pain, a sharp reaction to any irritant that does not go away immediately, night pain. This is acute focal pulpitis. It does not spread to the entire pulp, so it can be cured biologically (the same as pulp hyperemia). Vital amputation is also possible. It involves removing part of the pulp that is located in the crown. The root canals are not touched. The cavity is filled with calcium paste and a filling.
As the condition progresses, the next phase will be diffuse pulpitis, purulent in nature. The symptoms are the same, but the pain is stronger and can migrate to the temple. Here, amputation of the pulp is not enough, so they resort to vital extirpation. This option, unfortunately, is most often encountered in practice. Endodontic treatment is required - treatment and filling of root canals to completely remove the inflamed tissue.
When the roof of the tooth cavity cannot resist the carious process, it may collapse. A communication will arise between the carious cavity and the pulp chamber (tooth cavity). This is typical for chronic pulpitis. Symptoms subside by this stage. Chronic pulpitis is divided into:
- Chronic fibrous pulpitis, or chronic pulpitis itself. There may be no symptoms. Characterized by pain when moving from a cold to a warm place, pain from warm food.
- Chronic gangrenous pulpitis, or pulp necrosis. Possible bad breath, pain when changing air temperature and discomfort after eating hot and warm food.
- Chronic hypertrophic pulpitis, or pulp polyp. The complaints are the same. Bleeding from the causative tooth is possible. Pulp tissue grows in the carious cavity.
Without proper treatment, pulpitis can go further, and then get worse.
Pulpitis can lead to periodontitis, which in turn leads to periostitis. The teeth that caused periostitis are removed. You should not wait for a last resort while the tooth can still be cured and saved. Stages of treatment
Consider the treatment of pulpitis, which requires root canal treatment. This is a very common procedure in the practice of a general practitioner. It is called vital extirpation or pulpectomy (complete removal of the pulp).
Before treatment, a targeted x-ray of the causative tooth is required. Later during treatment, X-ray monitoring is also carried out at some stages. However, it is important to know that the anatomy of root canals is individual, and an x-ray image is only a two-dimensional projection of volumetric reality, from which it is not always possible to draw objective conclusions.
Anesthesia. It is mandatory in the treatment of conditions with acute pain. The anesthetic begins to act quite quickly.
Preparation of a carious cavity. All lifeless and infected hard tissues are drilled out and a cavity is formed. Treated with an antiseptic.
Opening the tooth cavity. This is done very carefully so as not to touch the walls of the cavity or its bottom. At the same stage, the pulp inside the crown is removed.
Expansion of entrances to root canals. The mouths of the canals are not so obvious. Firstly, they still need to be found, and secondly, they are very narrow. They are expanded with a special drilling tool at low speeds.
Removal of root pulp. Once the canals can be entered, the pulp is removed from them with a herringbone-shaped instrument that has “spines” on a thin shaft. They cling to the pulp and capture it.
Passage and filling of root canals. All dirt and infected tissue must be removed from them. To do this, they are passed through with endodontic needles. The canal must be completely passed through, processed and dried, and then completely sealed, otherwise the treatment may fail and will have to be re-treated. This stage is the most crucial moment in the treatment of pulpitis.
Sometimes, according to indications, the dentist first fills the canals temporarily and only at the next appointment replaces the temporary material with a permanent one. Temporary calcium-containing material can remain in the canal for up to 14 days.
Gutta-percha is most often used for permanent filling. It is produced in the form of rods (pins), which are placed in the root canals until the latter are completely filled. The excess is cut off with a heated iron, so during treatment there is no need to be alarmed when the doctor lights a match and heats up the instrument.
Next, the cavity is filled with filling material, the anatomy of the tooth is formed, ground, and polished. The treatment is completed.
After treatment
Composite fillings are currently being installed. In this case, you can eat and drink immediately after treatment. Some pain and swelling is normal for the first 24 hours after treatment. They disappear 1-2 days after treatment. In all other cases, you should immediately contact your dentist. Unfortunately, when treating pulpitis, complications are not uncommon, and the doctor is not always to blame for them.
After 2 years, it is advisable to do an X-ray control of changes around the tooth.
Pulpitis can be prevented by timely treatment of carious cavities.
Non-standard anatomy of the mandibular incisor canals in an individual patient
In clinical practice, there is a very significant divergence of tooth root canal systems. Different teeth may have different numbers of root canals, and their anatomy and relationships continue to be the subject of research to this day. This article describes a clinical case of successful endodontic treatment of all four mandibular incisors, with each tooth having four canals of different morphology. X-ray examination revealed the presence of several canals in the central and lateral incisors of the mandible. According to the literature, the presence of several canals in the central and lateral incisors of the mandible is quite rare; The uniqueness of this clinical case lies in the fact that in each of the four incisors two canals of different anatomy and morphology were found.
Introduction
The success of endodontic treatment directly depends on a thorough knowledge of the external and internal anatomy of the tooth. One of the reasons for the negative outcome of endodontic treatment is ignorance of the types of morphological diversity of the tooth root canal system. Mandibular incisors typically have one root and one canal, but anatomical variations occur - two canals with two apical foramina and two canals opening into one apical foramen.
Before commencing endodontic treatment, it is critical to visualize all internal anatomical relationships of the canals. It is mandatory to take and carefully study two or more periapical radiographs. To obtain information about the morphology of the tooth root canal, radiographs must be performed in direct, lateral, and also angular projections. The diagnostic minimum examination of the patient includes:
- Taking two or more radiographs before surgery;
- Assessing the bottom of the pulp chamber with a sharp probe;
- Channeling cracks with an ultrasonic nozzle;
- Staining the bottom of the chamber with a 1% solution of methylene blue;
- Performing a sodium hypochlorite test (“champagne bubble tests”);
- Visualization of the source of bleeding from the canal.
All of these methods are used to identify additional holes in the canal.
Stropko recommends, before beginning a visual inspection of the root canal system, to clean and dry the bottom of the pulp chamber using a 17% aqueous solution of ethylenediaminetetraacetic acid (EDTA), a 95% ethanol solution, and a Stropko irrigator filled with a 27G endodontic needle with lateral perforation.
The use of an intraoperative dental microscope also plays a major role in visualizing the root canals. It saves time and allows the operator to selectively and accurately remove dentin, minimizing the number of errors arising from operating errors.
Rice. 1. X-ray taken before surgery.
Rice. 2. Vertucci classification.
Description of a clinical case
A 45-year-old man was admitted to the clinic with complaints of high tooth wear, which caused the formation of a periapical abscess of both central incisors and irreversible pulpitis of the lateral incisors. X-ray examination revealed the presence of several root canals in each of the four incisors (see Fig. 1). Surgical access was performed, the root canals of the teeth were inspected, after which it turned out that all four teeth had two separate canals - buccal and lingual. According to the Vertucci classification, the canals were classified as type II (31 and 32) and type IV (41 and 42). The working length was determined with an apex locator (Propex, Dentsply) and confirmed by radiographic data. The relationships between the canals within each tooth were determined radiographically (see Fig. 3). [Figure No. 3 is missing from the original document]
Rice. 4. Working length.
Rice. 5. Obturation.
To ensure that no additional root canal was missed, angular radiographs of the teeth were taken. After confirming the presence of two canals in all lower incisors, the canals were prepared using the “Step Back” technique. At each instrument change, 2.5% sodium hypochlorite solution and saline solution (0.9% sodium chloride solution) were used as irrigants. Calcium hydroxide was injected intracanally; the access cavities were temporarily filled with neutral restorative material for 1 week. At the second visit, the cavities were washed and filled (see Fig. 4). After 6 months, a radiograph was taken at the follow-up examination (see Fig. 5).
Rice. 6. After 6 months.
Discussion
The anatomy and morphology of the root canal system is quite complex, and the success of endodontic therapy depends on the timely detection of an additional root or root canal. Canals not detected in time are one of the main reasons for the negative outcome of endodontic therapy. Also, incomplete removal of irritant substances from the pulpous space can lead to a negative outcome of treatment.
In most cases, two root canals merge into one near the apex. In order to be confident in detecting all additional channels, it is necessary to carefully study and interpret radiographic data (which, in turn, must be performed not only in direct, but also in angular projections). If the additional canal ends suddenly, you should think about the presence of two canals in the tooth.
Manual examination of the tooth root canal system using an endodontic probe or guide is also a fairly reliable research method that allows you to determine the configuration of the tooth root canals, in particular the number of holes. Particular care should be taken when accessing the cavity, since it is at this moment that it is easiest to miss the additional canal opening. On the lower front teeth, it makes sense to also examine the buccal and lingual walls of the cavity.
Numerous antibacterial agents are recommended for internal coating. One of the simplest and most accessible methods of cavity disinfection is calcium hydroxide paste, which was also used in the case described above.
This article describes a successful case of root canal treatment for all four mandibular incisors, each with two separate canals, in two teeth (31 and 32) opening into the same apical foramen, and in two teeth (41 and 42) opening into different apical foramina.
Conclusion
The anatomy of the root canal system can be quite complex. There may be differences in canal configuration, number of canals, and presence of narrowing sites. For successful diagnosis and treatment of such canals, it is necessary to carefully study the anatomy and morphology of the tooth root canals before performing surgery, including taking additional angular radiographs. An integrated approach to choosing a method of surgical access will also help in clinical practice.
Authors:
Sudha Mattigatti , Rushikesh Ramesh Mahaparale , Rutuja Vijay Chopade , Vaibhav Garg (Department of Conservative Dentistry and Endodontics, Faculty of Dental Sciences, KIMSDU, Karad, Satara, Maharashtra. India)
Upper jaw:
Central incisor - average length 25.0 (22.5 - 27.5 mm) number of canals - one main, in 10% of cases an additional canal.
Lateral incisor - average length 23.0 (21.0 - 25.0 mm) one main canal, in 9% of cases an additional canal.
Fang - average length 27 mm (24.0 - 29.7 mm) one main canal, in 23% of cases an additional one.
First premolar - average length 21 mm (19.0 - 23.0 mm) 85% two canals; palatal, buccal 9% one canal - main.
6% - three canals: palatal, buccal, accessory.
Second premolar: average length 22 mm (20.0 – 24.00 mm)
75% - one main channel
24% - two canals - palatal, buccal
1% - three canals: palatal, buccal, accessory.
First molar : average length 21 mm (18.0 – 26.0)
86% - three canals: palatal, buccal, distal, buccal - medial.
14% - two canals: palatal, buccal
45% - four canals: palatal, buccal - distal, medial - buccal (MB1), medial - buccal (MB2) this is the most common name for the buccal canals - international.
Second molar - average length 20.5 mm (19.0 - 24.0 mm) 1% - one main canal.
4% - two canals - palatal and buccal.
55% - three canals - palatine, buccal - medial, buccal - distal,
40% - palatal, buccal - distal, medial - buccal (MB1), medial - buccal (MB2).
Third molar - the number of root canals varies from 1 to 5.
A little about the simple and important...
V. D. Karashchuk , endodontist at the Portselyan clinic (Kiev)
I will try to formulate the rules and algorithms for forming an access cavity and searching for root canal orifices in the first and second molars of the upper jaw. I hope this article is helpful.
One of the common mistakes in endodontic treatment of maxillary molars is the “missing” of the 2nd mesiobuccal canal (MB2). According to studies, the prevalence of this anatomical formation ranges from 67% in the first molars of the maxilla, 44% in the second molars [1] to 93.0% and 60.4%, respectively [2]. Identifying MB2 channels is an extremely important aspect of our work. The following is a diagram of the formation of the access cavity and the location of the root canal orifices. According to Sert S et al. [3], the entrance to the MB2 canal is located 0.72 mm mesially (mesial distance) and 1.86 mm palatally (palatal distance) (tooth cut at the level of the neck). In practice, we quite often encounter partial or complete absence of external landmarks, which can lead to inadequate cavity formation and complicate the search for root canal mouths. Let's consider the situation using a clinical example. The patient came with irreversible pulpitis. Before starting work, an impression is taken and all the old restoration is removed. Endodontic treatment is carried out, and a temporary restoration made of self-hardening plastic is reproduced from the impression. In this form, the patient goes to the supervising doctor to complete the treatment. A certain difficulty in this case after the removal of the old restoration, which occupied half the height of the tooth crown, was caused by the complete absence of external anatomical landmarks. The photo (Fig. 1, 2) shows how I did it.
Rice. 1. Pulpitis.
Rice. 2. Pulpitis.
Next (Fig. 3, 4) a case is presented in which all necrotic dentin in the distal-proximal area was removed and the distal wall of the tooth was restored.
Rice. 3. All necrotic dentin is removed.
Rice. 4. The distal wall of the tooth has been restored.
The part of the tooth that does not have a pulp chamber was filled with GIC at the time of endotherapy. The most important thing is to preserve the maximum amount of dentin so that the restored tooth lasts a long time.
Many have encountered similar diagrams and clinical cases of the location of the orifices of the upper molar and know that the orifice of the mesiobuccal canal is located under the tuber of the same name. This is the place from which you can start looking for the pulp horn at the start of treatment. Difficulties arise if, before endodontic treatment, the tooth was damaged by caries and restored with a photopolymer or other material (GIC, amalgam). Due to the production of secondary dentin, when the arch of the pulp chamber moves towards the mouth of the canal and can be very tightly located above the mouth, denticles may form, complicating the entrance to the mouth of the canal. In Fig. Figure 5 shows how the pulp chamber changes if the restoration occupies a large space - in tooth 1.6 the lumen of the pulp chamber is practically closed by secondary dentin, and in tooth 1.7 the pulp chamber is large initially and there will be no problems when searching for canal mouths.
Rice. 5. Modification of the pulp chamber.
A similar situation is in Fig. 6.
Rice. 6. Modification of the pulp chamber.
Often during endodotic intervention we encounter denticles. There are many causes of radiation. They are classified into free and wall. Loose denticles are those that can be located freely in the pulp tissue. The parietal is combined with the inner surface of the dentin. The denticles cover large areas of the pulp chamber and the upper third of the root canal. In Fig. Figure 7 shows a denticle that has not yet united with the wall of the pulp chamber.
Rice. 7. Denticle that has not yet united with the wall of the pulp chamber.
It looks like a bunch of grapes (the dark veins are blood vessels). The next situation is that there is no longer a roof on the pulp chamber. In Fig. 8 The lumen of the tooth cavity is occupied by the denticles.
Rice. 8. The denticle occupies the entire lumen of the tooth cavity.
In such situations there is often a lot of bleeding. When we try to find the mouth of a canal, we begin to doubt, because the probe gets into the space between the denticle and the tooth wall and it seems that there are mouths everywhere. In such situations, sodium hypochlorite for a few minutes and a regular scaling attachment work well. It should simply be inserted into the cavity and passively sound the pulp cavity (PUI) without attempting to extract anything. Next, you can use a thin excavator to easily remove pieces of denticle from the pulp chamber. When initializing an MB2 channel, you should not rush to process it. The entrance to the mouth of this canal is not where its continuation is, and it is possible to perforate or block this canal. In Fig. 9, a 06 s+ file was inserted into the mouth of the MV2 channel.
Rice. 9. A 06 s+ file is inserted into the mouth of the MV2 channel.
If you have blocked the canal, there is only a chance of carefully preparing this area with carbide burs and/or ultrasonic tips with displacement and recess into the mouth. Here I recommend using magnification. If perforation is made (Fig. 10, 11), and you have experience working with MTA, then you can close the perforation with this material.
Rice. 10. Perforation is made.
Rice. 11. Perforation is made.
There are cases when there is no MV2 canal in the first molars, but with the use of an operating microscope and general magnification, there are fewer and fewer such teeth. You can paint over the area of the mouth of the MV2 canal with a caries detector and apply the light of a photopolymer lamp, placing it on the side surface of the tooth. This way you can “grope” the MV2 canal and at the same time check the tooth tissue for cracks in the enamel, which can be a key step in the further restoration of the tooth... Fig. 12-13: this case is confirmation of the “dangerous” location of the mouth of MV2.
Rice. 12. “Dangerous” location of the mouth of MV2.
Rice. 13. “Dangerous” location of the mouth of MV2.
In the patient, the pulp chamber of the second upper molar is flattened and elongated, which is typical for teeth of this accessory. And when identifying the mouth of MV2, I had to resort to special care so as not to transport the mouth and pulp chamber too much, because the mouth was located almost at an angle of 90 degrees. It is necessary to try to preserve all the buttresses of the tooth as much as possible. Almost all maxillary second molars have such a pulp chamber and the diagram I provided at the beginning is often not suitable... In maxillary second molars, the MV2 canal can move depending on how flattened the pulp chamber is. In Fig. 14 — top view of the tooth cavity: flattening of the pulp chamber and displacement of MV2 towards the mouth of the palatal canal.
Rice. 14. Top view of the tooth cavity.
The following case confirms that the MV2 channel is displaced approximately when processed with NiTi files. Rice. 15 and 16 show the location of the mouth of the main channels and the mouth of the MV2 channel, Fig. 17: 06 C+ file for scouting and initial processing has been entered, fig. 18 — the mouths of all channels have been processed and the MV2 channel has shifted to its true position.
Rice. 15. Location of the mouth of the main canals and the mouth of the MV2 channel.
Rice. 16. Location of the mouth of the main canals and the mouth of the MV2 channel.
Rice. 17. 06 C+ file for scouting and initial processing has been introduced.
Rice. 18. The mouths of all canals are processed.
Compare fig. 15 and 18 - how small the mouth of the MV2 canal is at first and what it is like after identification and treatment. This is probably why they used to think that there were only three canals in the upper molars - it was impossible to visually catch or find such an entrance with a tool.
The following is an example of tooth 1.6. The intraoral image (IOS) (Fig. 19) shows how much this patient is suffering: the absence of bony septa, inadequate restorations and secondary caries. Complaints of discomfort after eating and poor sensitivity to irritants. The restoration was done more than seven years ago and requires immediate replacement.
Rice. 19. Intraoral image.
After anesthesia and isolation of the working area with a rubber dam (Fig. 20), we removed all old restorations and almost all necrotic dentin in the approximal areas (Fig. 21).
Rice. 20. Isolation of the working field with a rubber dam.
Rice. 21. Removal of old restorations and necrotic dentin.
The bottom of the carious cavity was easily cut off with a sharp excavator, and it was impossible to keep the tooth alive; it had to be depulped. Before trephination, the missing walls are restored with adhesive flowing contrast material, which was removed before prosthetics. During an autopsy, it is necessary that the IOS is always in front of your eyes, because it is he who dictates the location of the autopsy. I trepanned the roof of the pulp chamber in the middle. Access was made using a carbide surgical extended bur, which does not cover the surgical field during treatment. You cannot make chaotic movements, demolishing everything in your path; it is necessary to move the bur around the circumference of the cavity in the same way as an orthopedist does when treating a tooth for an orthopedic design. Rice. Figure 22 shows an approximate view of the pulp chamber after the roof has been removed.
Rice. 22. Approximate view of the pulp chamber after removing the roof.
If there are no carious lesions, then we preserve all the walls of the pulp chamber as much as possible without over-instrumentation. After removing the roof of the pulp chamber, we were faced with a denticle that was located freely.
The denticle was removed using ultrasound and GC 5.25%. First of all, the main (main) canals are processed, and only after that it is necessary to identify MV2 and additional anatomy. I processed and formed the main canals and only then, when GC 5.25% dissolved the organic component of the pulp chamber as much as possible, did I start searching for the mouth of the MV2 canal. In the place where the mouth of the MV2 channel should have been, there was a dead end. Everything looked like a slot where only small files could be entered. Armed with GC 5.25%, a diamond ultrasonic nozzle and using an endochuck, I “expanded” the entire isthmus (isthmus), and I managed to find the true entrance to the MV2 canal. The mouth was located close to the mouth of the MV channel, as shown in Fig. 23, and the original entrance turned out to be a blindly ending groove.
Rice. 23. The mouth is located close to the mouth of the MV canal.
The increase will help to overcome almost all problems that arise at the time of treatment. Teach yourself to sit correctly, also teach your assistant to sit correctly, create ergonomic conditions around you, etc. But this is the topic of another article.