All people have a unique appearance and unique facial features. Some of us sometimes experience gaps between our teeth. Sometimes this defect may be subtle. But in other cases, such imperfection leads to serious physical as well as psychological consequences, and the issue of correcting this disorder is very relevant for a person.
Classification of dental gaps
Diastemas
– these are gaps of any size between the front central incisors. Tremae are spaces between any other teeth in the upper or lower jaw. Gaps between the lower front incisors are uncommon, but gaps between the upper central teeth can be seen several times more often. In many cases, the presence of a diastema of this kind provokes serious psychological discomfort, interfering with the harmonious socialization of patients.
Depending on what type of teeth are – baby or permanent – a distinction is made between false and true gaps between them. False dental gaps are observed in children - such defects go away on their own along with the change of teeth. True gaps form between permanent teeth and can only be removed with specialized help from a dentist. Doctors advise starting to correct such defects immediately after they occur, since then it will require much less time and effort.
What is atraumatic tooth extraction?
The essence of atraumatic tooth extraction is to saw the crown under local anesthesia into a certain number of parts (this depends on the number of roots in the tooth) and carefully remove each part along with its root. With this method, the interradicular bone septa are preserved and the walls of the socket are not damaged, which is extremely important for good healing and further prosthetics.
One of the stages of atraumatic tooth extraction is the infusion of platelet mass into the socket, which promotes tissue regeneration and accelerates healing. Thus, a basis is formed for further prosthetics using dental implants.
After atraumatic tooth extraction, the wound heals quite quickly and without problems such as swelling, bruising and other troubles familiar to many. It goes without saying that the patient must strictly follow all the recommendations of the attending physician for several days.
Gap between teeth: what should be done?
If you have a very small diastema, then a visit to the dental clinic can wait. However, even a small gap should be regularly monitored by a doctor, since tooth gaps tend to grow over time. However, if the diastema is significant, it is better to visit the dentist as soon as possible. This defect can contribute to the development of caries, malocclusion, gum disease, etc. Various methods have been developed for correcting diastemas. Typically, the doctor carries out treatment on an individual basis and selects a method that will be most effective for a particular patient. The technique is chosen based on the reasons for the appearance of a gap between the teeth, the size and degree of development of the dental gap, and the wishes of the person himself.
Possible complications after tooth extraction
23.09.2012 18:12- Simple tooth extraction “all inclusive” - 2500 rub.
- Removal of a tooth with periodontal disease - 1500 rub
- Removal of a permanent tooth (complicated) - resorcinol formalin / bur separation machine / wisdom tooth - 4000 rub
- Removal of impacted (dystopic) wisdom tooth - 5500 rub
- Removal of an impacted (dystopic) wisdom tooth using an ultrasonic device - 7500 rub
Tooth extraction is a full-fledged operation, after which certain unpleasant consequences may arise, caused both by the behavior of the patient himself and by factors beyond his control. Complications can also arise during the operation, since the removal of some teeth can be very difficult: due to the large size of the root or strong bone tissue, it is necessary to make incisions, which, after a successful operation, are stitched. In any case, there is no need to worry, since unprotected tissues in the postoperative period are under maximum influence of microbes, which can result in inflammation.
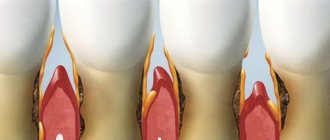
Alveolitis
Very often, after tooth extraction, a complication such as alveolitis occurs. This problem occurs when a blood clot necessary for healing has not formed at the site of the extracted tooth. In this case, the hole becomes defenseless against external influences, as a result of which an inflammatory process often develops in it .
The key symptom of this complication is pain after tooth extraction (of varying degrees of severity). Pain may occur after 2-3 days. At the same time, the mucous membrane of the gum swells, the edges of the socket become inflamed, there is no blood clot in the tooth socket and the socket is possibly filled with food debris. The patient may have a fever, and sometimes there is pain when swallowing. The hole itself becomes covered with a dirty gray coating that emits an unpleasant odor. Along with these symptoms, the patient often feels general malaise, enlarged lymph nodes, slight swelling, fever, and pain in the area of the extracted tooth.
The main causes of alveolitis
Alveolitis is a disease that is not associated with the introduction of infection into the tooth socket as a result of working with an unsterile instrument. The disease develops with the participation of those microbes that are normally found in the oral cavity of every person.
So, teeth are usually removed due to the fact that chronic foci of inflammation are localized in the area of their roots that cannot be eliminated by conservative methods.
Therefore, the socket of the extracted tooth is primarily infected, and the concentration of microorganisms in it is quite high. If a person is healthy and all immune systems function normally, then the microflora is suppressed and the hole heals without complications. In the event that there are any local or general malfunctions in the mechanisms of the body's reactivity, the likelihood of developing inflammatory complications in the socket increases significantly.
Thus, the following local and general causes may contribute to the development of alveolitis:
- long-term existence of chronic inflammatory foci with frequent exacerbations, as well as exacerbation of the chronic inflammatory process;
- traumatic removal, when conditions arise for the destruction of the created barrier and the penetration of microflora deep into the tissues;
- absence of a blood clot in the socket of the extracted tooth (the clot did not form, or the patient did not follow the doctor’s instructions and the clot was removed; this usually happens when the patient is inattentive to the doctor’s recommendations and diligently rinses the tooth socket);
- general changes in the body due to stress, recent colds (infectious or viral) diseases, the presence of chronic diseases (mainly endocrine), especially in the stage of decompensation, general physical exhaustion, etc.
Treatment of this complication after tooth extraction
Treatment consists of relieving inflammation with local and general means. Sometimes it is sufficient to simply thoroughly rinse the hole with antiseptic solutions and then treat it with a special aseptic ointment or paste. Then, with the help of antibiotics and vitamins, general anti-inflammatory therapy is carried out. But sometimes treatment is delayed up to 1.5 - 2 weeks. In some cases, for this complication, physiotherapy or laser therapy may be prescribed.
Socket bleeding
One of the most common complications after tooth extraction is alveolar bleeding, which can occur immediately after surgery, within the next hour, day, and sometimes more than a day after tooth extraction.
Main causes of bleeding
- Early alveolar bleeding can be caused by the use of adrenaline: when it stops its action, a short dilation of the blood vessels occurs, which causes bleeding.
- Late socket bleeding may occur due to violation of the doctor’s recommendations in the postoperative period - mainly as a result of external disturbance of the socket of the extracted tooth.
- Local causes of socket bleeding include various physical injuries in the area of the socket of an extracted tooth: damage to the gums, fracture of part of the alveolus or interradicular septum, development of inflammation in the area of the extracted tooth, damage to blood vessels in the palate and under the tongue.
- The general causes of the appearance of alveolar bleeding are most often associated with various concomitant diseases of the patient (leukemia, scarlet fever, jaundice, sepsis, hypertension, etc.).
Treatment of this complication after tooth extraction
The effectiveness of stopping alveolar bleeding depends on how correctly the causes and source of bleeding were identified.
- If blood comes from the soft tissue of the gums, then sutures are placed on the edges of the wound.
- If blood comes from a vessel in the wall of the tooth socket, then first apply local cold in the form of an ice pack, then tightly squeeze the bleeding vessel and place a tampon soaked in a special hemostatic agent into the socket, which is removed no earlier than 5 days.
- If local measures do not help, dentists turn to general hemostatic agents that increase blood clotting.
Paresthesia
Much less often, after tooth extraction, a complication such as paresthesia may occur, which is caused by nerve damage during the process of tooth extraction. The main symptom of paresthesia is numbness in the tongue, chin, cheeks and lips. Paresthesia, as a rule, is a temporary phenomenon, disappearing within 1-2 days to several weeks.
Treatment of paresthesia is carried out through therapy with vitamins B and C, as well as injections of dibazole and galantamine.
Changing the position of adjacent teeth after tooth extraction
After tooth extraction, defects can often form in the jaw, and neighboring teeth begin to tilt towards the formed defect, and the antagonist tooth from the opposite jaw begins to move towards the defect, which leads to disruption of the chewing process. At the same time, the chewing load sharply increases, the usual state of the jaws is disrupted and bite deformation develops, which can greatly affect the general condition of the teeth. In this case, it is recommended to replace the extracted tooth with an artificial one using bridges, implants, or removable partial dentures.
All kinds of injuries that occurred during tooth extraction
Often, when removing the second premolar and molars of the upper jaw, perforation of the bottom of the maxillary sinus , resulting in communication between the oral cavity and the nasal cavity through the sinus.
The reasons are as follows:
(subject to the correct and careful actions of the doctor)
- anatomical features: the roots of the above teeth are close to the bottom of the sinus, and in some cases the bony septum is completely absent;
- the presence of a chronic inflammatory focus at the apex of the tooth, which destroys the already thinned bone plate.
If, after the removal of premolars or molars of the upper jaw, a message still appears, the doctor must use one of the known methods to eliminate it during the same visit.
There is only one contraindication:
The presence of a purulent inflammatory process in the sinus (acute purulent maxillary sinusitis). If the message is not diagnosed and eliminated in time, the patient feels liquid and liquid food entering the nose. In this case, you should consult a doctor as soon as possible. If you delay visiting a doctor, a chronic inflammatory process will inevitably develop in the sinus, which will require more serious and technically complex treatment.
Potential complications during the tooth extraction procedure include:
- Damage to adjacent teeth. Adjacent teeth or dentures (eg, crowns, bridges, implants) next to the extracted tooth can sometimes be damaged during the procedure. Adjacent teeth may become broken, split into pieces, or weakened during the extraction of the tooth or teeth, sometimes requiring more time from the dentist.
- Tooth fracture . The tooth may break during the extraction process, making the procedure more difficult and requiring more time and effort to complete the extraction. You may have to remove the tooth in parts. By the way, the process of removing a tooth in parts can cause complications after tooth extraction.
- Incomplete tooth extraction. A small portion of the tooth root may be left in the jawbone. Although this may increase the risk of infection, sometimes the dentist will choose not to try to extract it because removal may be too dangerous, for example if it is very close to a nerve.
- Jaw fracture. Patients with weak jaw bone structure (such as older women with osteoporosis) may be at risk for a jaw fracture. Even if the actual tooth extraction procedure is completed smoothly without any problems, there are cases of complications during the recovery period. Most often, a fracture of the jaw (in the lower jaw) occurs during the removal of “wisdom teeth” and in the upper jaw – a separation of the tubercle of the upper jaw.
- Removal of part of the alveolar ridge - occurs when a tooth is removed incorrectly, when forceps are placed directly on the bone surrounding the tooth and the tooth is removed along with it. In this case, an extensive bone and cosmetic defect occurs (especially in the anterior-frontal area). This problem can only be solved with the help of plastic surgery using artificial bone tissue and special protective membranes.
- Removal of a baby tooth and the germ of a permanent tooth - Occurs due to the carelessness or lack of professionalism of the doctor. When a baby tooth is removed (very often the roots of the tooth are missing, since they dissolve before changing teeth), the doctor begins to look for them in the tooth socket and perceives the germ of a permanent tooth as the roots of a baby tooth.
Remember the main thing: you should trust your doctor and actively participate in the treatment yourself, i.e. unquestioningly and carefully follow all recommendations. And if you suspect the development of complications, do not delay and do not hesitate to consult a doctor again.
Use of artistic restoration
Some patients are advised to undergo aesthetic artistic dental restoration to eliminate diastema. This is a therapeutic intervention during which composite microprostheses (veneers) are installed on the two central incisors, between which there is a gap. The doctor uses a filling material that matches the patient’s natural enamel shade and builds up additional volume of hard tissue on the two central front teeth. To undergo this procedure, you only need to visit the clinic once.
When restoring a tooth, the doctor restores its shape and function. The presence of colored deposits and cracks in the enamel, and other signs of destruction of dental tissue does not play any role, since most of the visible dental tissue is removed. Then its natural shape, color and functional properties are formed using composite materials (build-up method). If the root of a tooth is damaged, it is treated first, and restoration is carried out only at the next stage. If no pathologies associated with the tooth root are detected, then in 5-6 hours a qualified doctor is able to restore at least 4-5 teeth. However, if the dentist first works with the root of the tooth, then further manipulations are carried out after at least two days.
An important advantage of artistic restoration is its complete painlessness. Another important advantage of this method is its safety, therefore it has a minimal list of contraindications. Dental restoration can be performed on women even during pregnancy.
Advantages of atraumatic tooth extraction
Compared to traditional methods, atraumatic tooth extraction has a number of advantages:
- The procedure does not cause any discomfort in the patient. Instead of ordinary forceps, dentists use special periotome knives, which allow them to cut the ligaments and carefully pull the root out.
- Thanks to the use of special preparations during atraumatic tooth extraction, bone tissue atrophy is prevented and the process of restoration and healing of the hole is accelerated. This is facilitated by the preservation of the interroot septum.
- Since bone tissue is not destroyed during atraumatic tooth extraction, the specialist has the opportunity to immediately perform one-step implantation.
Surgical plastic surgery
For many patients, the determining factor in choosing a method for eliminating diastema is the cost of therapy. Be sure to consider your financial resources when you and your doctor select a method for correcting a dental gap. Choose the method that suits you best, but do not skimp on your health, as otherwise you may not achieve what you want and spend even more money on eliminating the negative consequences of unsuccessful treatment.
A tooth gap can also be removed using surgical plastic surgery. This technique involves installing dental crowns. Dentists correct the defect by placing ceramic veneers or crowns on the front teeth. This intervention allows you to achieve an excellent aesthetic effect that lasts for many years. Some disadvantage of this technique is its rather high price.
If for one reason or another you cannot use this technique, the doctor can fill the front teeth for corrective purposes, as a result of which the gap will be eliminated. Pay attention to the above method if the diastema occurs a second time or the installation of staples does not bring the desired result.
Application of radiological methods in the diagnosis of periodontal diseases
Author: Sotirios Tetradis
Radiographs are valuable for diagnosing periodontal disease, assessing severity, determining prognosis, and assessing treatment results. However, radiographs are only an addition to clinical examination, and not a replacement for it.
Radiographs demonstrate changes in calcified tissue; they do not reveal current cellular activity, but rather reflect past cellular activity on bone and roots.
Normal interdental septum
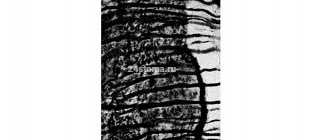
The assessment of bone changes in periodontal disease is based primarily on visualization of the interdental septum, since the relatively dense root structure obscures the vestibular and lingual bone plates. The interdental septum is usually described by a thin radiopaque line adjacent to the periodontal ligament and on the alveolar ridge called the fascicle (Fig. 31-1).
Figure 31-1. The ridge of the interdental septum is usually parallel to a line drawn between the cemento-enamel junction of adjacent teeth (arrow). Note also the radiopaque layer of fascicle bone around the roots and interdental septum.
Because the fascicle is the cortical bone lining the dental socket, the shape and position of the root and changes in the angle of the x-ray beam produce significant changes in its appearance.
The width and shape of the interdental septum and ridge angle usually vary depending on the convexity of the proximal tooth surfaces and the level of the cemento-enamel junction (CEJ) of the contacting teeth. The vestibulo-oral diameter of the bone is related to the width of the proximal root surface. The angle of inclination of the ridge of the interdental septum is usually parallel to the line between the CEJs of the contacting teeth (see Fig. 31-1). When there is a difference in the level of the CEJ, the interdental bone ridge appears tilted rather than horizontal.
X-ray research methods
In conventional radiographs, periapical and bitewing views offer the most accurate diagnostic information and are most often used in the evaluation of periodontal disease. To correctly and accurately determine the periodontal status of the bone, it is necessary to adhere to the correct exposure and development techniques. The level of bone, the pattern of bone destruction, the width of the periodontal ligament, as well as the radiodensity, trabecular pattern and marginal contour of the interdental septum, vary depending on the exposure and time of examination, the type of film and the direction of x-ray radiation. To obtain high-quality images both before and after treatment, a standardized research methodology is required.
Prichard established the following four criteria to determine adequate angulation of periapical radiographs:
- The radiograph should show the cusps of the molars, and some visualization of the occlusal surface is also possible.
- The boundaries of the tooth and pulp chambers must be distinguishable.
- The interdental space must be open.
- Proximal contacts should not overlap unless the teeth follow anatomical lines.
For periapical radiographs, the parallel long-cone radiograph method most accurately projects the level of the alveolar bone (Fig. 31-2).
Figure 31-2. Comparison of long-cone radiographs and radiographs obtained by the angle bisector method. A, Shot for
Orthodontic correction methods
Orthodontic methods for correcting diastemas are rightfully considered the safest, most effective and gentle (they allow you to preserve a maximum of healthy dental tissues). However, their main drawback is the long duration of treatment. Malocclusions are eliminated step by step - for this, braces are used. Orthopedic treatment is primarily indicated for children and adolescents whose permanent teeth have recently replaced their deciduous predecessors. Braces are special orthodontic structures that are attached to the teeth from the inside (invisibility braces) or the outside. How long do you need to wear braces? This is determined by the doctor individually, but usually treatment continues until the bite is completely corrected (from 6 to 24 months). It is best to install braces when the jaw is actively growing.
Your dentist may also recommend mouth guards, which are small transparent covers for your teeth. Aligners contain information about the normal shape and size of teeth. These devices are made in such a way that they move individual teeth in the required direction, restoring their correct position. The result of this is that the teeth move closer to each other and the diastema is eliminated. Aligners have a transparent base, so they are even less noticeable on the surface of the teeth than braces.
The advantage of mouth guards is that they can be removed while eating. Moreover, since they are filled inside with a whitening compound, using this method, you will not only eliminate the gap between the front incisors, but also lighten the tooth enamel. This will also add beauty to your smile and eliminate the need for additional whitening procedures.
Orthodontists are indispensable if a person, in addition to diastema, is diagnosed with any other malocclusion. Metal braces are considered affordable and reliable for most patients.
All problems can be solved
An even dentition, white teeth of regular shape adorn any person and serve as an integral part of an ideal smile. Thanks to this, everyone can feel attractive, because in the modern world almost any dental defect can be successfully corrected. Thanks to this, many patients are able to return to normal life. Therefore, if you are concerned about the presence of a diastema, this imperfection can be corrected quite quickly and painlessly in dentistry near the Krasnye Vorota, Baumanskaya, Novokuznetskaya and Tretyakovskaya metro stations. Do not be indifferent to your health and psychological state, and confidently contact dental specialists to solve your problems.