All tissues of the oral cavity, both teeth and gums, are interconnected and naturally have a complex structure. Gums, just like teeth, require careful and thorough care. Periodontology is a separate science in dentistry that deals with the study of gum disease. Inflammation from the teeth can spread to periodontal tissue, and vice versa. Therefore, it is so important to maintain careful hygiene of the entire oral cavity and promptly treat any dental diseases.
Gum structure
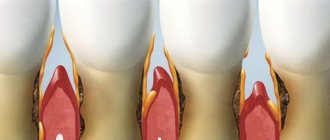
The periodontium consists of a complex of tissues that form the entire periodontal space.
- Periodontium is a complex of fibers that hold the dental unit in the socket. The periodontium is located between the cementum and the alveolar wall. Nerve fibers, lymphatic vessels, veins and arteries are also located here, which together are responsible for the proper metabolism of the tooth.
- The gums are the outer part of the entire complex. The gums are the first to bear the brunt of harmful microorganisms that enter the oral cavity.
- The alveolar process is a bone plate that has a spongy structure and serves as a bed for the dental unit.
- Cement is the outer covering and protection of the tooth root.
- Enamel covers the crown of the tooth and is the hardest element of the entire complex.
- The pulp is the main source of metabolism in the tooth. Consists of blood vessels and nerve endings.
- Dentin is a substance located around the pulp and consisting mainly of mineral components.
The structure of the periodontium: anatomy and histology of periodontal tissues
The periodontium (paro (perio) = around, odontos = tooth) includes the following tissues: (1) gingiva (G), (2) periodontal ligament (PL), (3) root cementum (RC) and (4) alveolar bone proper ( ABP) (Figure below). ABP lines the alveolus of the tooth and is inextricably linked to the alveolar bone; On an x-ray, it may appear as a lamina of dura mater. The alveolar process, which extends from the basal bone of the maxilla and mandible, consists of the alveolar bone and the alveolar bone itself. The main function of the periodontium is to attach the tooth to the bone tissue of the jaws and maintain the integrity of the surface of the chewing mucous membrane of the oral cavity. The periodontium, also called the “supporting apparatus” or “supporting tissues of the teeth,” is a developing, biological and functional unit that undergoes certain changes with age and, in addition, undergoes morphological changes associated with functional changes and changes in the oral environment. The development of periodontal tissue occurs during the development and formation of teeth. This process begins early in the embryonic phase when cells from the neural crest (from the neural tube of the embryo) migrate into the primary branching arch. In this position, the neural crest cells form a band of ectomesenchyme under the epithelium of the stomatodeum (primitive oral cavity). Once the uncommitted neural crest cells have reached their location in the jaw space, the stomatodeum epithelium releases factors that initiate epithelial-ectomesenchymal interactions. Once these interactions have occurred, the ectomesenchyme assumes a dominant role in further development. After the formation of the dental plate, a series of processes begin (bud stage, cap stage, bell stage with root development) that lead to the formation of the tooth and surrounding periodontal tissues, including the alveolar bone itself. During the cap stage, ectomesenchymal cells condense against the dental epithelium (dental organ [DO]), forming the dental papilla (DP), which gives rise to dentin and pulp, and the dental follicle (DF), which gives rise to periodontal supporting tissues (Fig. . below). The crucial role played by ectomesenchyme in this process is further established by the fact that the tissue of the dental papilla also appears to determine the shape and appearance of the tooth. If the bell-stage tooth germ is dissected and transplanted to an ectopic site (for example, connective tissue or anterior chamber of the eye), the process of tooth formation continues. A crown and root are formed, as well as supporting structures (cementum, periodontal ligament and a thin plate of the alveolar bone itself). Such experiments confirm that all the information necessary for the formation of a tooth and its attachment apparatus is located in the tissues of the dental organ and the surrounding ectomesenchyme. The dental organ is the formative organ of the enamel, the dental papilla is the formative organ of the dentin-pulp complex, and the dental follicle is the formative organ of the attachment apparatus (cementum, periodontal ligament and the alveolar bone itself). The development of the root and supporting periodontal tissues follows the development of the crown. Epithelial cells of the outer and inner dental epithelium (dental organ) proliferate in an apical direction, forming a double layer of cells called Hertwig's root epithelial sheath (RS). Odontoblasts (OBs) that form root dentin differentiate from ectomesenchymal cells in the dental papilla under the inductive influence of internal epithelial cells (Fig. below). Dentin (D) continues to form in the apical direction, producing the root framework. During root formation, periodontal supporting tissues, including acellular cementum, develop. Some data in cementogenesis still remain unclear, but the following concept is gradually emerging. Early in dentin formation, the inner epithelial cells of the Hertwig root synthesize and secrete enamel-associated proteins, probably belonging to the amelogenin family. At the end of this entire period, the epithelial root sheath becomes fenestrated and ectomesenchymal cells from the dental follicle penetrate these fenestrations and contact the root surface. Ectomesenchymal cells in contact with enamel-associated proteins differentiate into cementoblasts and begin to form cementoid. This cementoid is an organic cement matrix and consists of crushed matter and collagen fibers that are mixed with collagen fibers in the not yet fully mineralized outer layer of dentin. It is assumed that the cementum becomes firmly attached to the dentin through these fiber interactions. The formation of cellular cementum, which often covers the apical third of dental roots, differs from the formation of acellular cementum in that some of the cement blasts are embedded in the cementum. The remaining parts of the periodontium are formed by ectomesenchymal cells from the dental follicle lateral to the cementum. Some of them differentiate into periodontal fibroblasts and form periodontal ligament fibers, while others become osteoblasts and form the alveolar bone itself, in which the periodontal fibers are anchored. In other words, the primary alveolar wall is also an ectomesenchymal product. It is likely, but still irrefutably proven, that ectomesenchymal cells remain in the mature periodontium and take part in the life activity of this tissue.
Periodontal functions
In a healthy state, the periodontium performs a number of functions assigned to it:
- Support. The main function is due to which the tooth is held between bone plates.
- Shock-absorbing function. Correctly distributes pressure over the entire dentition.
- Trophic. A function responsible for nutrition and ensuring metabolism of the tissue complex.
- A protective function that helps create a barrier against the effects of bacteria.
- Reflex – affects the correct distribution of the chewing load.
- The plastic function is responsible for the elasticity of periodontal tissues.
Periodontium, histology
What is periodontium at the microscopic level? Histology is a science that can find out this. Considering the periodontium, histology identifies the following main tissues in its anatomical composition - bone (alveolar process), connective (gingiva, pulp, periodontium), epithelial (covers the gum from above).
Among the cellular elements one can find fibroblasts, osteoblasts, cementoblasts, and epithelial cells. Histology also identifies amino acids, polysaccharides and proteins in the components of periodontal tissue.
Periodontal diseases
Reasons why gum disease occurs:
- soft and hard plaque on teeth;
- anomalies in the location of dental units;
- poor-quality prosthetics or treatment;
- genetic predisposition;
- reduced immunity;
- diseases of internal organs;
- hormonal imbalances in the body;
- constant stress;
- various bad habits;
- Irregular oral care.
In contrast to the large number of causes influencing the development of periodontal diseases, there are not so many diseases themselves:
- Gingivitis is the initial stage of gum inflammation.
- Periodontitis is an inflammatory process in the gums, gradually spreading to the alveolar processes of the jaw.
- Periodontal disease is a fairly severe form of the disease, characterized by exposure of the roots of the teeth.
- Periodontoma is the formation of tumors in soft tissues.
How to treat?
The treatment method will depend on the nature of the disease itself. For catarrhal form, rinsing with antiseptic and anti-inflammatory solutions and herbal decoctions is sufficient. Chamomile, sage or calendula work best. For best results, it is recommended to rinse the area under the hood.
Treatment of the purulent form is more complex. Antibiotics, angihistamines and anti-inflammatory drugs are prescribed. Surgical treatment has 2 options:
- Removal of a tooth;
- Excision of the mucous hood.
The first option is more drastic, but it allows you to completely get rid of the cause. Excision of the hood is used for correct but difficult tooth eruption. An incision is made under local anesthesia, the cavity is washed and drainage is installed. After surgery, the patient is prescribed antiseptic rinses.
Chronic pericoronitis is treated only by tooth extraction.
The use of a laser provides a good therapeutic effect. The affected area is exposed to infrared radiation, which penetrates deep into the tissue. To completely eliminate all signs, it is recommended to carry out 7-10 daily procedures. The result of treatment will be a reduction in inflammation and swelling.
Of course, treatment can begin at home. Rinsing will relieve acute symptoms, but will not get rid of the main cause of the condition - the tooth. Self-administration of antibiotics will also alleviate the condition, but only a doctor can prescribe the correct dose and regimen.
Treatment
Treatment of major periodontal diseases is as follows:
- removing all plaque and then polishing the teeth;
- treatment of existing carious formations;
- carrying out high-quality prosthetics, if necessary;
- splinting of the dentition (also carried out if necessary);
- treatment of existing common diseases;
- taking vitamins or medications;
- Regular cleaning of the oral cavity not only at home, but also in the dental office.
In the most difficult situations, in addition to the listed treatment, surgical intervention may be necessary.
The structure of the periodontium under a microscope –
In Figure 8 below you can see collagen fibers penetrating the root cementum. Please note that the terminal sections of the fibers (located in the cement of the root or in the bone wall of the alveoli) are called Sharpey's fibers. Next, Fig. 8 shows a histological preparation of the periodontium of a tooth, where 1 – bundles of collagen fibers, 2 – the main amorphous substance, 3 – periodontal vessels.
Electron microscopy data made it possible to find out that periodontal fibers penetrate into the cement of the tooth root to a depth of only 3 to 5 μ.t, and into the bone wall of the alveoli - no more than 20 μ.t. It also became known that although periodontal fibers consist predominantly of mature type 1 collagen, it also contains some immature elastic fibers (oxytalan). These fibers are only 2-3 mm long, and they are not located perpendicularly like all steel fibers, but parallel to the surface of the tooth root. Oxytalan fibers cross the dento-alveolar fibers at right angles, and their role is to redistribute blood flow in the periodontium under conditions of chewing load.
Collagen fibers occupy only 40% of the periodontal volume, and the remaining 60% is nothing more than the main amorphous substance (which, in turn, consists of as much as 70% water). In addition to water, there is also a large number of different cellular elements present here - first of all, we are interested in fibroblasts, which are located along the collagen fibers. Fibroblasts can also differentiate into fibrocytes or myofibroblasts during the cell cycle.
Another group of cellular elements includes cementocytes and cementoblasts. The latter are located on the surface of the cementum of the tooth root, and their function is to build replacement cement. There is also a small group of cellular elements, which include osteoblasts, osteoclasts, and odontoclasts. The following are also found in small quantities in the periodontium: lymphocytes, plasma cells, mast cells, eosinophils and neutrophilic leukocytes.
Periodontal histology: video
Below in video 1 you can see the histology of tooth tissue in stunning resolution. Video 2 is the best lecture on periodontal histology you can ever hear. The video is in English, but if you wish, you can turn on subtitles, and then select translation from English into Russian in the settings.