Periodontal disease is a set of pathological processes that spread to the tissues surrounding the teeth and holding them in the alveoli. According to statistics, pathologies belonging to this group are diagnosed in 90% of the adult population. Moreover, most often diseases of this type are detected in men and women aged 37-45 years.
In the absence of timely and competent treatment, periodontal diseases can cause loosening and premature tooth loss, the appearance of foci of chronic infection in the oral cavity, deterioration of the body’s immune status and the development of other complications. That is why modern dentists pay increased attention to the development of methods and means for treating pathologies belonging to this group.
Structure and functions of periodontium
Periodontium is usually called a complex of tissues that includes:
- alveolar processes (areas of the jaw that bear the dentition);
- gums (mucous membranes covering the alveolar processes);
- periodontium (tissues consisting of protein fibers and located in the space between the alveolar plate and the cement of the tooth root);
- cement (special bone tissue covering the roots and necks of teeth).
In the human body, the periodontium performs the following functions:
- shock-absorbing (evenly distributes the load on the jaws);
- supporting-retaining (provides strong fixation of the tooth in the alveolar socket);
- trophic (contains an extensive network of lymphatic and blood vessels, a huge number of nerve receptors);
- barrier (protective) and others.
Preserving periodontal tissue in a healthy state is the key to long-term and proper functioning of the masticatory apparatus.
The relationship between periodontal diseases and occlusion pathology
E. V. Bykova assistant at the department of orthodontics of North-Western State Medical University named after. I. I. Mechnikova
P. P. Zhdanov Associate Professor of the Department of Orthodontics of Northwestern State Medical University named after. I. I. Mechnikova
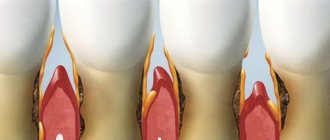
The relationship between periodontal diseases and occlusion pathology is currently beyond doubt. The pathology of occlusion is accompanied by incorrect positioning of the teeth, their inclination and rotation, in which the axis of application of occlusal forces does not coincide with the axis of the tooth, and the physiological forces associated with chewing become excessive. Such forces applied to the teeth, with intact periodontal tissues, cause primary occlusal trauma.
With healthy periodontium, occlusal trauma leads to increased tooth mobility without destruction of the periodontal ligament. With damaged periodontal tissue, excessive occlusal load promotes the spread of inflammation into deeper periodontal structures, increasing the severity of periodontal processes (Klinberg I. et al., 2006; Kalamkarov H. A. et al., 1972; Goldman HM, 1956; Jin LJ et al. ., 1992).
At the same time, Geiger AM (2001) refutes the long-existing theory about the pathology of occlusion as an etiological factor in periodontal diseases. However, according to his data, pronounced jaw discrepancies and traumatic occlusion contribute to the aggravation of the pathological process in the periodontium. As dental crowding increases, the risk of developing periodontitis increases in patients over 35 years of age (Pugaca J. et al., 2007).
Physiological occlusion and correctly positioned teeth are anatomically and physiologically necessary to maintain periodontal health and prevent the development of periodontitis (Loginova N.K. et al., 1993; Popov S.A., 1999). Ramfjord SP et al. (1973) argue that with the loss of supporting teeth as a result of the formation of a deep incisal overlap, the resulting overload of this area leads to the development of periodontal diseases.
Thus, the opinions of scientists regarding the relationship between the pathology of occlusion and periodontal diseases are contradictory.
Purpose of the study: to assess the relationship between dental deformations and pathological changes in periodontal tissues.
Material and research methods
126 people (102 women and 24 men) aged 20-54 years were examined. The condition of periodontal tissues was assessed as: healthy periodontium, generalized periodontitis of mild and moderate severity. The comprehensive examination included: clinical, laboratory, morphometric, and radiological research methods.
Research results
The indicators of the recession index and the degree of gum retraction indicate (Table 1) that in patients with dentition deformations, with an increase in inflammatory manifestations in the periodontium, the prevalence and volume of recessions significantly increase. Of the total number of patients examined, 54 (42.9%) were patients with distal occlusion, 44 (34.9%) were patients with neutral occlusion, and 28 (22.2%) were patients with mesial occlusion (Table 2).
Table No. 1. Recession index (RI) and degree of retraction index (DR) of the gums in patients at the diagnostic stage (n=126)
| Sign | Intact periodontium (n=38) | HP of mild severity (n=42) | GP of moderate severity (n=46) |
| IR (%) | 0 | 13,38±5,18 | 59,75±7,05 1 |
| CP (mm) | 0 | 0,13±0,06 | 0,75±0,15 2 |
Note: 1 - t=5.22; p<0.001; 2 - t=3.71; p<0.001 (compared to the group of patients with mild periodontitis).
Table No. 2. Distribution of patients according to occlusion pathology and clinical examination data (n=126)
| Sign | Intact periodontium (n=39) | Mild GP (n=42) | Moderate GP (n=45) | Total (n=126) |
| Neutral occlusion | 15 (39,5 %) | 17 (40,5 %) | 11 (26,1 %) | 43 (34,9 %) |
| Distal occlusion | 17 (43,6 %) | 16 (38,1 %) | 22 (47,8 %) | 55 (42,9 %) |
| Mesial occlusion | 7 (16,9 %) | 9 (21,4 %) | 12 (26,1 %) | 28 (22,2 %) |
| P.I. | 0,26±0,04 | 0,38±0,07 ** | 0,38±0,05 ** | − |
| PBI | 0,49±0,09 | 0,99±0,10 ** | 1,64±0,12 *, ** | − |
| Tooth mobility | 0 | 0,36±0,08 | 0,75±0,12 * | − |
| ZDK depth | 2,14±0,14 | 2,67±0,14 * | 3,51±0,24 ** | − |
Note: 1) there is no relationship between the condition of periodontal tissues and the nature of occlusion (χ2=2.73; p>0.10); * — p<0.01 (compared to mild HP); ** — p<0.001 (compared to intact periodontium).
At the same time, distal occlusion in 47.8% of cases is combined with generalized periodontitis of moderate severity. Mild generalized periodontitis was diagnosed in 42 people (33.3% of cases), and in 17 patients it was combined with neutral occlusion, and in 16 people (38.1% of cases) it was found in combination with distal occlusion. Mesial occlusion in a greater percentage of cases is combined with generalized periodontitis of moderate severity and is observed in 26.1% of cases.
To analyze the relationship of the jaws and options for dentoalveolar compensation of occlusion, the inclination angles of the incisors of the upper and lower jaw, teleradiography of the skull was performed in a lateral projection
The diagnosis of occlusion pathology, made according to a clinical examination, does not fully reflect the discrepancy in jaw size, since dentoalveolar compensation can significantly reduce this discrepancy. It represents a change in the inclination and height of the dentoalveolar complex to achieve optimal or satisfactory occlusion and is implemented in three planes. It manifests itself most significantly in the area of the anterior teeth in the sagittal plane (Slavichek R., 2008; Sadao S., 2008). Dental alveolar compensation leads to changes in the inclination of teeth and the development of periodontal diseases.
For a more accurate analysis of the relationship of the jaws and options for dentoalveolar compensation of occlusion, the inclination angles of the incisors of the upper and lower jaw, we performed teleradiography of the skull in a lateral projection.
The relationship between the apical bases of the upper and lower jaw was determined on a teleradiogram using WITS and A-Po analysis. Of the entire group of patients examined, 64 (50.8%) patients had Engle class I, 36 (28.6%) had Engle class II, 26 (20.6%) had Engle class III. The relationship between Angle class and periodontal pathology is presented in Figure 1.
Rice. 1. Correlation between Angle class and periodontal pathology (n=126)
As can be seen from Figure 1, with intact periodontium, Engle class I occurs in 35.9% of cases, Engle class II - in 33.3%, Engle class III - only in 11.5% of cases. Generalized periodontitis of moderate severity is combined with Engle class III in 42.3% of cases.
The assessment of the inclination of the incisors of the upper and lower jaws was carried out on a teleroentgenogram in the lateral projection according to the angles: internal angle I-NL - the angle of inclination of the upper incisors to the plane of the base of the upper jaw, IMPA - the angle of inclination of the lower incisors to the plane of the base of the lower jaw. The results obtained were compared with the norm presented in the works of Proffitt U.R. (2008), Alexander R.G. (2008). A relationship has been identified between the angle of inclination of the incisors and the condition of periodontal tissues, which is presented in Table No. 3. From Table No. 3 it follows that with normal inclination, intact periodontium occurs in 48.5% of cases, protrusion of incisors in 47.8% of cases is combined with generalized periodontitis mild severity and in 34.3% - with generalized periodontitis of moderate severity.
Table No. 3. Dependence of periodontal pathology on the inclination of the maxillary incisors
| Periodontal condition | Total research | Norm | Protrusion of incisors | Retrusion of incisors |
| Intact periodontium | 38 | 16 (48,5 %) | 12 (17,9 %) | 10 (38,5 %) |
| mild GP | 42 | 9 (27,3 %) | 32 (47,8 %) | 9 (34,6 %) |
| Moderate GP | 46 | 8 (24,3 %) | 23 (34,3 %) | 7 (26,9 %) |
| Total | 126 | 33 (100 %) | 67 (100 %) | 26 (100 %) |
Note: there is a relationship between the condition of periodontal tissues and the inclination of the maxillary incisors (χ2=11.01; p=0.026).
By assessing the position of the incisors of the upper and lower jaw, we established the relationship between the inclination of the teeth and the relationship of the jaws. Thus, in Engle class I, incisor protrusion occurred in 29 (45.3%), normal position - in 21 patients (32.8%). With less frequency, normal inclination of the incisors occurred in patients with distal occlusion (22.2% of cases) and mesial occlusion (15.4% of cases) (Fig. 2).
Rice. 2. Correlation between teeth inclination (normal and protrusion) and Angle class (n=126).
An analysis was carried out of the dependence of the condition of periodontal tissues on the relationship of the jaws in the vertical and transversal planes, the position of individual teeth and groups of teeth. No dependence was found on the degree of periodontitis: on the depth of incisal overlap (?2=7.74; p>0.10), the presence of cross-occlusion (?2=1.15; p>0.10), three and crowding of teeth (?2 =5.02;p>0.10). A relationship has been found between the inclination of teeth and the degree of periodontitis.
Conclusion
As the analysis of clinical data shows, distal occlusion (47.8%) and mesial occlusion (42.9%) in a greater number of cases are combined with generalized periodontitis of moderate severity. Neutral occlusion occurs with almost the same frequency in patients with intact periodontium and generalized periodontitis of mild severity, and only in 26.1% of cases is combined with generalized periodontitis of moderate severity.
Analysis of the recession index shows the predominance of maximum prevalence values for mesial occlusion
When assessing the prevalence of periodontal diseases depending on the pathology of occlusion, it was found that the highest prevalence of generalized periodontitis of moderate severity is observed in patients with distal occlusion and occurs in 47.8% of cases. Generalized periodontitis of mild severity was combined with neutral occlusion in 40.5% of cases and with distal occlusion in 38.1% of cases.
There was no dependence of the degree of periodontitis on the depth of incisal overlap (?2=7.74; p>0.10), the presence of cross-occlusion (?2=1.15; p>0.10), three and crowding of teeth (?2= 5.02; p>0.10). Analysis of the recession index shows the predominance of maximum prevalence values with mesial occlusion. A relationship between the prevalence and degree of gum retraction and the pathology of occlusion was revealed. The recession index values are higher with mesial occlusion. The degree of gum retraction is more pronounced with distal occlusion.
- Kalamkarov Kh. A., Gantsev G. A., Ershov V. N. Relationship between dentofacial deformations and periodontopathies in children // Dentistry. - 1972. - No. 5. - P. 47-50.
- Klinberg I., Jaeger R. Occlusion and clinical practice. - M.: Medpress-inform, 2006. - 200 p.
- Loginova N.K. Functional prerequisites for the development of a mechanical theory of the etiology and pathogenesis of periodontal diseases // New in dentistry. - 1993. - No. 1. - P. 2-7.
- Popov S.A. Diagnosis and treatment of incorrect position of individual teeth in children using modern orthodontic technology: Abstract of thesis. dis. ...cand. honey. Sci. - St. Petersburg, 1999. - 22 p.
- Sato S., Akimoto S., Matsumoto A., Shirasu A., Yoshida Y. Guidelines for the clinical application of the IVD technique. — M.: Azbuka, 2008.—158 p.
A complete list of references is in the editorial office
Causes of periodontal disease development
Factors that increase the likelihood of developing periodontal disease are:
- heredity;
- hypovitaminosis;
- failure to comply with hygiene requirements;
- presence of dental plaque;
- dental anomalies (bite disorders and others);
- somatic diseases (malfunctions of the nervous system, gastrointestinal diseases, diabetes mellitus, cardiac and endocrine disorders);
- smoking;
- weakened immune system;
- non-compliance with drinking regime;
- habit of breathing through the mouth;
- the presence in the oral cavity of low-quality fillings, orthodontic or orthopedic structures incorrectly installed in dentistry.
In addition, the risk of disease directly depends on the place of residence, lifestyle, characteristics of professional activity and dietary habits of patients.
Gum structure
The periodontium consists of a complex of tissues that form the entire periodontal space.
- Periodontium is a complex of fibers that hold the dental unit in the socket. The periodontium is located between the cementum and the alveolar wall. Nerve fibers, lymphatic vessels, veins and arteries are also located here, which together are responsible for the proper metabolism of the tooth.
- The gums are the outer part of the entire complex. The gums are the first to bear the brunt of harmful microorganisms that enter the oral cavity.
- The alveolar process is a bone plate that has a spongy structure and serves as a bed for the dental unit.
- Cement is the outer covering and protection of the tooth root.
- Enamel covers the crown of the tooth and is the hardest element of the entire complex.
- The pulp is the main source of metabolism in the tooth. Consists of blood vessels and nerve endings.
- Dentin is a substance located around the pulp and consisting mainly of mineral components.
Symptoms of periodontal disease
The first symptoms indicating the occurrence of periodontal disease are:
- tingling, itching, numbness in the gums;
- bleeding of gum tissue;
- swelling of the interdental papillae;
- thickening of the gingival margin;
- detachment of gums from dental crowns.
In the future, the clinical picture may be supplemented by:
- gradual exposure of the necks of the teeth;
- redness, hyperemia of the gums;
- formation of pathological gum pockets;
- increase in interdental spaces;
- gradual loosening of teeth.
Symptoms of tissue diseases also include increased sensitivity of dental tissues to irritants, as well as aching pain in the affected area.
Classification and symptoms
Pathological damage to the tissues surrounding the dentition, in most cases, occurs as a result of an imbalance between bacterial symbiosis and oral tissues. There are 5 main categories:
- Gingivitis is an inflammation of the marginal part of the gum mucosa adjacent to the teeth, occurring without disturbing the position and mobility of the teeth. Accompanied by swelling, redness, pain and bleeding. The main cause is periodontal pathogens: Porphyromonas gingivalis, Aggregatibacter actinomycetemcomitans and other gram-negative anaerobic coccobacilli. Under the influence of their toxins, a change in the structure of the tissues of the dental epithelial junction occurs, which serves as a barrier that prevents the penetration of infectious agents towards the tooth root. There are several forms: catarrhal (occurs in 97% of cases), hypertrophic, ulcerative-necrotic. The outcome of gingivitis can be complete restoration of periodontal tissue. Without adequate treatment, it turns into periodontitis and threatens adentia.
- Periodontitis is an inflammation of periodontal tissues, accompanied by progressive destruction of soft tissues and atrophy of the jaw bone. The causes are usually poor hygiene, mechanical injuries and hypersensitivity to certain medications. Risk factors include hormonal and general metabolic disorders, immunodeficiency states, malocclusions, hypertonicity of the masticatory muscles, etc. The disease develops gradually, and at the initial stage does not cause noticeable discomfort. Early manifestations may include bleeding, soreness and changes in the shape and color of the gums, and the appearance of bad breath. As the process progresses, periodontal pockets deepen, alveolar processes are destroyed, which leads to loosening and tooth loss. In severe cases of the disease, pus may be released from the periodontal pocket and an increase in body temperature may be noted.
- Periodontal disease is a dystrophic lesion of the periodontium, accompanied by gradual resorption of bone tissue. Periodontal disease is less common and, as a rule, is one of the symptoms of hypertension, atherosclerotic changes in blood vessels, neurogenic or endocrine pathologies. The difference between periodontitis and periodontal disease is that with periodontitis there is always an inflammatory process, while with periodontal disease it is absent. With periodontal disease, gum pockets do not form, there is no purulent discharge, and tooth displacement occurs only in severe forms of the disease when the root is more than half exposed. At the initial stage of the disease, there is usually no discomfort. Patients with moderate severity of periodontal disease experience burning, itching, and hyperesthesia. In severe cases of periodontal disease, due to loss of bone tissue, interdental spaces – trema – are formed between the teeth. A fan-shaped divergence of the crowns is observed.
- Idiopathic lesions. These include a number of general somatic diseases, one of the clinical manifestations of which is the progressive lysis of periodontal tissue (Papillon-Lefebvre, Hand-Schueller-Christian syndrome, neutropenia, immunodeficiency states, acatalasia, etc.). The causes of idiopathic periodontal pathologies are not completely clear. The leading role is played by genetic predisposition. Patients develop deep periodontal pockets with the release of exudate, displacement and loosening of dental units. Characterized by rapidly progressing resorption of bone tissue with the formation of oval-shaped cavities.
- Periodontomas are benign tumor and tumor-like pathologies of the periodontium: gingival fibromatosis, epulis, periodontal cyst, etc. They usually develop as a result of chronic irritation of soft tissues by destroyed tooth walls, sharp edges of deep-set crowns, and incorrectly modeled clasps of a removable denture.
Treatment of periodontal diseases
The general treatment program for periodontal diseases includes:
- removal of microbial plaque and mineralized deposits from the surface of teeth;
- caries therapy;
- preventing functional overload of certain areas of the dentition;
- rejection of bad habits;
- carrying out orthodontic treatment (if indicated);
- anti-inflammatory therapy;
- combating systemic diseases;
- the use of drugs that enhance immunity, stimulate osteogenesis and activate the adaptive and protective functions of the body;
- carrying out general hygiene measures (monitoring the regime of work, nutrition, rest, hygiene).
The treatment regimen for periodontal diseases is drawn up taking into account all manifestations of the disease and the results of a comprehensive examination of the patient. Timely seeking of professional help by a patient significantly improves the prognosis of the disease, shortens the duration of treatment and avoids the development of complications.
Treatment
Treatment of major periodontal diseases is as follows:
- removing all plaque and then polishing the teeth;
- treatment of existing carious formations;
- carrying out high-quality prosthetics, if necessary;
- splinting of the dentition (also carried out if necessary);
- treatment of existing common diseases;
- taking vitamins or medications;
- Regular cleaning of the oral cavity not only at home, but also in the dental office.
In the most difficult situations, in addition to the listed treatment, surgical intervention may be necessary.
Gingivitis
Gingivitis is an inflammatory disease of the marginal gums, while the supporting structures of the tooth are not affected.
There are several types of gingivitis:
- Catarrhal. It manifests itself as mild bleeding and swelling of the gums, itching.
- Hypertrophic. Characterized by bad breath and severe bleeding.
- Ulcerative-necrotic. Ulcers appear on the gums, and a gray coating appears on the teeth. This pathology is characterized by severe pain and putrid odor from the mouth.
Gingivitis can be acute or chronic, affecting the entire gum or the area of 1 to 3 teeth.
The causes of the disease may be:
- Poor dental hygiene, accumulation of soft plaque, which promotes the growth of bacteria.
- Injury from too hard foods or a hard toothbrush.
- Poorly installed crown or filling.
- Disturbances in the functioning of the heart.
- Hormonal disbalance.
- Diseases of the gastrointestinal tract.
- Avitaminosis.
- Decreased immunity.
- Chronic poisoning with iodine, lead, mercury, aluminum.
- Blood diseases.
For gingivitis, the dentist removes dental deposits, treats the gums with an antiseptic, applies applications with medications, prescribes anti-inflammatory drugs, a vitamin complex, selects a toothpaste, brush, and mouthwash.
Periodontitis
Periodontitis is an inflammation of the periodontal tissue and ligaments, often a consequence of untreated gingivitis. In severe cases, it affects bone tissue.
Symptoms of periodontitis include:
- the formation of hard tartar, they can secrete pus;
- severe pain;
- tooth displacement;
- exposed dental necks;
- pain when pressing on mobile teeth;
- holes between teeth and gums;
- the occurrence of flux when an infection gets into an inflamed tooth pocket.
The development of periodontitis is promoted by hypertonicity of the masticatory muscles, crowded teeth, high frenulum attachment, traumatic bite, blood diseases, diabetes mellitus, chronic pathologies of internal organs, and immunodeficiency.
There are three forms of periodontitis according to the severity of inflammation:
- Easy. There is hyperemia of the edge of the gums - overcrowding of blood vessels, pain, bleeding, slight loss of bone, shallow depth of the bone pocket.
- Average. Bleeding gums can be spontaneous, teeth become loose. Brushing with a toothbrush and eating food are difficult, the pocket increases to 5 mm.
- Heavy. Teeth fall out, severe bleeding, deep bone pockets.
The approach to the treatment of periodontitis is complex and is divided into several stages:
Remove tartar every six months, as it grows quickly.
Oral hygiene. The doctor will select cleansers and rinses. Be sure to use dental floss and brushes if there are large gaps between the teeth. It is recommended to purchase an irrigator for rinsing pockets with water.
Antiseptic treatment using special gels and rinses. In advanced cases, drugs with a long-term disinfecting effect are used. These are gelatin flakes that the dentist places in the periodontal pocket. They swell and prevent bacteria from entering it. At the same time, an antiseptic is released from the scales.
Anti-inflammatory therapy: application of bandages and ointments, physiotherapy.
Prescription of vitamins, antibiotics, immunostimulants.
Surgery may be required. The dentist makes an incision in the gum and, using special instruments, removes tartar and damaged areas, and adds artificial bone tissue.
Periodontal disease
Periodontal disease is a rare pathology in which the periodontal tissue and ligaments are damaged. Teeth begin to loosen and fall out.
The occurrence of this disease is provoked by the following factors:
- alcohol abuse, smoking;
- hereditary predisposition;
- deficiency of vitamins in the body;
- vascular atherosclerosis;
- hormonal disbalance;
- diseases of internal organs;
- abnormal position of teeth, malocclusion;
- diabetes;
- elderly age.
With periodontal disease, the necks of the teeth are exposed, the mucous membranes become whitish and decrease in volume. A wedge-shaped defect may develop and increased sensitivity occurs. There is no bleeding or swelling of the gums. The teeth are well fixed in the socket; their mobility develops only with significant destruction of bone tissue.
Treatment of periodontal disease depends on the degree of development of the disease and may include:
- Professional oral hygiene.
- Elimination of malocclusion, alignment of incorrectly positioned teeth.
- Prosthetics in case of tooth loss.
- Surgical treatment aimed at restoring bone tissue.
- Periodontal massage and physiotherapy to improve blood circulation.
- The use of antibacterial agents and vitamin complexes.
Highly qualified specialists of the Formula of Health clinic will carry out all the necessary procedures to quickly rid the patient of periodontal diseases.
Treatment necessarily includes an x-ray using the latest generation Finnish digital device “Planmeca” to identify possible destruction of bone tissue.
Teeth cleaning is carried out using an Air Flow sandblasting machine, which painlessly removes plaque and tartar.
If the patient has an incorrect bite or misaligned teeth, it is recommended to wear the Damon braces system, which allows you to get good results within several months.
If a tooth is lost, it can be restored using crowns and veneers made of durable and high-quality materials in a variety of shades, ideally matching the color of the patient’s enamel.
In advanced stages of periodontal disease, surgical intervention may be necessary. Our specialists will perform an operation that allows you to completely get rid of the pathology and save your teeth.