Causes of crooked teeth
In the 1980s, the term crowding of teeth syndrome (CTS) was coined to refer to an abnormality that defines crowding of the anterior teeth that interferes with satisfactory oral hygiene.
STIs affect 70% of the world's adult population. The anomaly occupies a prominent place in the structure of all dental pathologies. The syndrome can occur both during the development of baby teeth and during the eruption of permanent teeth. In the first case, the prevalence is 34%, and in the second - 68%.
As a person grows, the degree of crowding of teeth may increase, as changes occur in the periodontal tissues: the ligamentous apparatus of the tooth becomes less stable. According to research, the older the age group of patients, the higher the percentage of people requiring orthodontic medical interventions. Thus, we can talk about the pattern of distribution of the anomaly by age and the absence of a pattern of distribution by gender.
The main reasons for the development of crooked teeth include:
- Quick replacement of temporary teeth with molars (up to 6-7 years). The jaw bones do not have time to develop, so there is not enough space for teeth. However, there is no data on why some children change their teeth earlier. This is an individual feature caused by abnormalities in the growth and formation of teeth.
- Bad childhood habits such as thumb sucking or pacifier use. As a result, the risk of malocclusion and abnormal tooth growth increases.
- Congenital malocclusion. Changing the size of the jaw (less often the shape) negatively affects the position of the molars, premolars, canines and incisors.
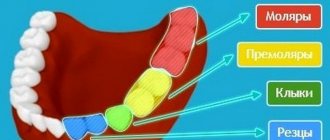
- Location and name of teeth
- Incomplete development of the alveolar process and the basal part of the upper jaw.
- Macrodentia, which means an excessive increase in the size of one or all teeth.
- Narrowing of dental arches due to soft tissue dysfunction. Dysfunction can be caused by hormonal imbalances, injuries, metabolic disorders, heredity and predisposition, and malocclusion.
- Appearance of third molars - “wisdom teeth”. This reason is typical for people of mature age, when the teeth are already formed and there is no room for the “eight”.
- Extra teeth - having extra teeth.
Congenital factors of diseases include: dysfunction of lip closure, anomaly of the frenulum of the tongue, infant swallowing, mouth breathing. Prolonged mouth breathing in childhood leads to deformation of the facial skeleton:
- the lateral parts of the upper jaw come closer together, as a result of which the upper jaw develops incorrectly;
- the hard palate becomes higher and narrower.
As a result, the upper row of teeth becomes much narrower. Subsequently, similar changes occur in the lower jaw. All this leads to torsion.
If you notice similar symptoms, consult your doctor. Do not self-medicate - it is dangerous to your health!
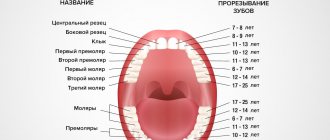
Timing of teething in children
Teething is physiological and serves as an indirect indicator of the correct or impaired development of the child. As a physiological act, teething is not a painful phenomenon and cannot cause any diseases. It is in direct connection with the general health of the child - timely growth of teeth in a certain sequence indicates the normal development of his body. A delay in teething may be a consequence of rickets, an infectious disease, prolonged dysfunction of the intestines and changes in metabolism. Earlier teething - endocrine disorders. A discrepancy in the time of the beginning of the eruption of the central incisors by 1-2 months from the conditional period cannot be considered as the effect of any pathology.
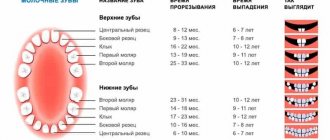
The newborn does not have a single tooth, although in rare cases their intrauterine development is observed. Between 6 and 8 months of life, the central incisors of the lower jaw begin to appear, and then the upper. By 8-12 months, the lateral incisors are formed first on the lower jaw and then on the upper jaw. By 12-16 months, the first molars erupt, by 16-20 months - the canines, and by 20-30 months - the second molars, which complete the formation of the primary bite.
The eruption of baby teeth often affects the child’s well-being. In weakened children, this physiological process is accompanied by general malaise, poor sleep, restless behavior, crying, and moodiness. Sometimes the temperature rises to 37.50C, the nature of bowel movements changes, short-term rashes on the body and redness of the facial skin are possible. The child's weight gain is temporarily suspended and immune defense is reduced. To establish the true cause of the malaise, a consultation with a pediatrician is necessary.
At the 7th year of life, the replacement of baby teeth with permanent ones occurs, the time of eruption of which, as a rule, coincides with the resorption of the roots of baby teeth and their loss. In contrast, the formation of a permanent bite begins with the appearance of the first molars of the lower jaw and normally ends by 15-18 years. The central incisors (8-9 years), first premolars (9-10 years), canines (10-11 years), second premolars (11-12 years), second molars (12-13 years) sequentially erupt. The third molars of the lower jaw, or as they are sometimes called “wisdom” teeth, grow later, often after the age of 20-25 years.
A correctly and timely formed bite plays a big role in the normal development of the child’s body. Violation of the timing of teething (early or late), the order, as well as the absence of one or another tooth require the attention of a pediatrician and dentist, since they are evidence of pathology not only of a local, but often of a general nature (the result of diseases suffered by the mother during pregnancy, or any anomalies in the child’s health).
For various reasons, a number of deviations can occur in the structure of teeth, their location and development: the absence of a rudiment of a tooth, an incorrect position of the tooth axis (horizontal or oblique), which is why it erupts outside the arch of the dentition or remains in the thickness of the jaw bone. In addition, the incorrect formation of the tooth itself - size, shape, position, color, lack of enamel coating, etc. Such changes should be analyzed by a specialist.
Timing of teeth eruption, formation of rudiments and roots, maturation of enamel
Baby teeth
| Teeth | Period of eruption, months. | Timing of root formation | Beginning of root resorption | Root resorption time |
| I | 6 — 8 | +2 years | from 5th year | in current 2 years |
| II | 8 — 12 | +2 years | from 6th year | in current 2 years |
| III | 16 — 20 | +3 years | from 8th year | in current 3 years |
| II | 8 — 12 | +2 years | from 6th year | in current 2 years |
| V | 20 — 30 | +3 years | from 7th year | in current 3 years |
Permanent teeth
| Teeth | Timing of eruption | Timing of root formation | Final “enamel maturation” | Bookmark of follicles |
| 6 | 5 — 6 | at 10 | at 1 - 3 years | at 5 months intrauterine development |
| 1 | 6 — 8 | at 10 | at 4 -5 years old | at 8 months high-quality development |
| 2 | 8 — 9 | at 10 | at 4 -5 years old | at 8 months high-quality development |
| 4 | 9 — 10 | at 12 years old | at 5-6 years old | at 2 years old |
| 3 | 10 — 11 | at 13 years old | at 6 -7 years old | at 8 months high-quality development |
| 5 | 11 — 12 | at 12 years old | at 6 -7 years old | at 3 years old |
| 7 | 12 — 13 | at the age of 15 | at 7-8 years old | at 3 years old |
For infants, the number of teeth that have erupted is one of the objective criteria by which the baby’s health status is assessed. The timing of teething and the order of their appearance can vary significantly. So, the first tooth can appear as early as 1 month or 1 year, but most often this happens at 6-8 months of life. To calculate the number of baby teeth (N), depending on age, use the formula: N = n-4, where n is the number of months of a child’s life. So, at the age of 12 months, the baby should have 8 teeth.
Signs of physiological teething
- Teething at certain average times
- Eruption pairing
- Teething in a specific order
Causes of delayed teething:
- rickets and other disorders of calcium-phosphorus metabolism;
- decreased activity of the endocrine glands (hypothyroidism);
- disturbances in the digestion and absorption of nutrients;
- severe eating disorders;
- chronic infections;
- hereditary disorders of mineral metabolism and diseases of osteochondral tissue;
Difficult teething with increased body temperature, catarrhal symptoms, and indigestion is most often caused by an infectious disease. Therefore, the appearance of such symptoms in a baby during teething requires a mandatory medical examination and observation!
Possible features of teeth in children at the teething stage:
- Expansion of spaces between teeth. It may reflect increased jaw growth and during the transition period from baby teeth to permanent teeth is regarded as a normal condition. A wide gap between the front incisors on the upper jaw is usually associated with a deep-lying maxillary frenulum. The tactics for monitoring and treating wide gaps between teeth are determined by an orthodontist.
- A blackish edging on the neck of the tooth can be due to the use of soluble iron preparations or a chronic inflammatory process (precipitation of bacteria of the leptotrichium group);
- Yellowish-brown staining of teeth is most often associated with the use of antibiotics by the mother in the second half of pregnancy or by the child during the period of teeth formation.
- A yellowish-greenish color develops in severe disorders of bilirubin metabolism and hemolytic (destruction of red blood cells) conditions;
- Reddish staining of tooth enamel is characteristic of a congenital disorder of pigment metabolism - porphyrin. This disease is called porphyria;
- Malocclusions occur due to uneven growth of the jaws, due to prolonged sucking of the nipple;
- Anomalies in the location of teeth occur for constitutional reasons (small jaw size), due to trauma, congenital disorders of connective tissue metabolism, and tumors of the alveolar process of the jaw.
The absence of teeth before 1 year of age is extremely rarely associated with edentia - the absence of their rudiments. You can check the presence of tooth germs using a special radiovisiography method prescribed by a pediatric dentist.
Stages and symptoms of the disease
A predisposition to the development of anomalies can be identified already in early childhood by consulting an orthodontist. During the examination, the specialist will find that there is no space between the baby’s teeth. This sign indicates that, with a high degree of probability, there will be no room left in the permanent dentition for tooth eruption. As they appear, the problem will only get worse. Timely identification of negative factors in children will help normalize the situation even at the stage of taking a bite of milk. However, very often specialists are faced with the fact that even with congenital prerequisites, patients turn to a specialist only during the period when the permanent dentition is fully formed and there are clinical signs.
The anomaly is characterized by varying degrees of severity, which causes clinical symptoms and possible complications. The degree of development of pathological signs also affects treatment tactics, as well as prognosis. Depending on the symptoms of dental crowding, there are 3 degrees of damage.
- A mild degree of anomaly is characterized by minimal changes in the position of 1-2 teeth in the dentition. In order for them to take the correct position, only 2-3 mm is missing. The problem does not extend to the remaining teeth; they occupy a clearly defined place;
- With a moderate degree of anomaly, the problem affects only individual teeth. They rotate around their axis, are offset relative to the teeth and can tilt. Their displacement corresponds to 5-6 mm;
- In the case of severe anomalies, its manifestations are clearly visible to others. The aesthetics of a smile is disrupted due to deformation of the dentition; some teeth are pushed out of the dentition. The arch shape has been changed.
The main disadvantage of the anomaly is that crowding of teeth leads to deterioration in the aesthetics of the dentition. This is especially noticeable with severe injuries. However, this is not the only problem.
With this position of the teeth, the chances of quality cleaning are significantly reduced. The prerequisites will be created for the formation of dental plaque, which will affect the change in the shade of the enamel, manifest as tartar deposits, and the presence of bad breath. Lack of proper hygiene will lead to the development of other dental diseases and the appearance of additional symptoms. Also, incorrect position of the teeth can lead to injuries to the mucous membrane. Symptoms will be supplemented by manifestations such as bleeding, inflammatory or erosive process.
Talking teeth
Anastasia Lyubalina
Administrator of the dental clinic "Ekostom"
Even in early childhood, we master all speech patterns, including speech motor standards for each specific sound. Impulses from the brain enter the speech organs, as a result we can pronounce sounds, and therefore speak. This skill is brought to automaticity in most healthy people in childhood and is not lost throughout life.
With age, in the course of life, people may experience various changes in the structure of the dental system, for example, tooth loss. The reasons for this may be: a change from a primary dentition to a permanent one (if the timing of this process is extended), genetic diseases, decreased immune processes, diabetes mellitus, trauma, insufficient oral hygiene at home or untimely visit to the dental clinic, as well as non-compliance with measures prevention and dentist recommendations and much more. Of course, these changes will entail characteristic secondary disturbances in the aesthetics of the face, the digestive process, and, of course, speech activity, in particular sound pronunciation.
Despite the high compensatory capabilities (as we know, the dental system is capable of self-regulation in terms of adaptation to changing external conditions), the older a person is, the more already honed skills suffer. Let us consider in more detail the mechanism of violations.
When teeth are lost, the organs of the dental system (mostly the tongue) tend to “fill” the resulting empty space. In this case, the tongue takes an inadequate position for itself both at rest and in the process of sound formation. The lips and cheeks seem to “sink” in the place where teeth are missing. In this regard, all speech-motor structures are disrupted, therefore, sound pronunciation is disrupted according to the type of distortion.
Depending on which segment is missing a tooth or several teeth at once, the pronunciation of different groups of sounds is correspondingly impaired. The violations are most clearly manifested in complete edentia, when all teeth are missing in the oral cavity. In this case, the pronunciation of all speech sounds is impaired.
Let's look at examples.
Depending on the location of the lost teeth, the pronunciation of the following groups of sounds is impaired:
1. labiodental sounds [V], [F] and their soft variants, if there are no lower incisors. The lower lip and upper incisors are involved in the process of pronouncing these sounds. The teeth seem to rest on the lower lip, and the air stream passes through an obstacle in the form of a “fence” of the teeth. In the absence of upper incisors, the air stream does not overcome the barrier created by the organs of articulation, which means the pronunciation is distorted.
2. Dental sounds [D], [T], [N], [L], their soft variants and the sound [C]. In the process of pronouncing these sounds, the tongue seems to be pushed away from the back wall of the upper incisors. In the absence of front teeth in the upper jaw, the tongue “falls” into an empty space in the dentition, preventing the organs of articulation from making the necessary movements. The pronunciation of sound becomes impaired.
3. Palatodental sounds [Ш], [Ш], [ж] In the process of pronouncing these sounds, the lateral edges of the tongue rest against the back wall of the chewing teeth, and in their absence, it occupies empty space, changing the speech motor structure of the pronounced sound, making it difficult to pronounce .
Specific to people with incomplete teeth is the so-called “lisp.” This change in pronunciation is associated with the incorrect position of the organs of articulation in the oral cavity, with a violation of the algorithm of movement of these organs. Depending on the specific reasons, a person may have a lisp in different ways. In some cases, a speech defect may be barely noticeable, and sometimes lead to a pronounced disruption of communication between people. This issue is especially acute for people in “speech professions” (speakers, teachers, etc.). It is typical for patients to switch to whispered speech, because this masks the lack of pronunciation.
The most modern and effective way to get rid of the disease is to restore the dentition through implantation and prosthetics. When installing orthopedic structures, the anatomical and physiological integrity of the dentofacial apparatus is returned to the patient. As a result, the speech organs return to their normal and familiar state at rest, and also take the correct position in the process of speech formation.
The sooner a patient addresses this problem to specialists of the appropriate profile, the more likely it is that the sound-pronunciation side of speech will be fully restored in a short time.
Expert opinion
Vitaly Zotkin
Doctor - orthopedic dentist at the Ecostom clinic
Changes in the speech of patients associated with tooth loss are always obvious and immediately reveal the problem. An experienced specialist can determine the location of a lost tooth by ear, down to the segment and serial number, already at the stage of the initial consultation.
For many patients, especially those whose profession is related to speech communication, in addition to other advantages of prosthetics and implantation, the effective rate of restoration of correct speech is very important. Oddly enough, this point is one of the most important in orthopedic dentistry. It is necessary to understand that in order to achieve the desired result, you need to select the working methods and, of course, the materials of the future design as accurately as possible. Using high-precision equipment and computer technology, orthopedic dentists, together with dental technicians, restore the complete anatomy of lost teeth, taking into account all the individual characteristics of the dental system of each individual patient.
During the treatment process, the specialist is obliged to warn the patient that after installation of the structure, speech function will not be restored immediately. This is due to the fact that the organs of the oral cavity responsible for speech formation “existed” for some time in the absence of teeth and managed to get used to them. There must be an adaptation period. Getting used to the prosthesis can take a long time, and the product may need to be adjusted. To shorten the adaptation period, training exercises are used, for example, reading poetry out loud, pronouncing tongue twisters, and articulation gymnastics.
As a rule, in all cases, after installation of the orthopedic structure, pronunciation is completely normalized, which is especially valuable for patients.
Why is it important to fix the problem in time?
Any orthodontic irregularities are potential dental problems in the future.
Improper closure leads to abrasion of the enamel on the cutting edge of the teeth (all or only on one side if the bite is asymmetrical).
When teeth are crowded, it is more difficult to remove plaque - this causes caries, and with insufficient care - gum disease.
If prosthetics are required in the future, placing an implant may not be possible or there may even be restrictions on placing a bridge. So first you will need to correct the position of the remaining teeth.
With severe crowding of teeth and a noticeable narrowing of the jaw, aesthetic problems are added: teeth look unsightly, asymmetry of the lower part of the face may occur.
Treatment by an orthodontist is not an aesthetic procedure. A beautiful smile is what you get as a bonus; the main acquisition is a correct bite and maintaining dental health in the future.
Wisdom teeth and crooked teeth
Wisdom teeth are one of the causes of crowding. Previously, wisdom teeth were needed: at the age of 20-30, other molars were worn down due to rough food, and the growing eight teeth were used for chewing food. In modern people, the chewing load is less, and the jaw is also lower, and the figure eight has not yet atrophied, so there is often no room for them.
The 8's are still trying to cut, but due to lack of space, they either grow at an angle or squeeze and move the other teeth, causing crowding as a result.
You can examine the rudiments of teeth on x-rays as early as 12 years of age. This way you can see if they are growing correctly or at an angle. If the jaw is small, wisdom teeth can be removed before the rash appears so that they do not cause any problems. But it is not at all necessary to simply remove them, since when they break out, they will make chewing easier and can serve as a support for dentures.
Teething
The emergence of permanent teeth from the place of origin and development into the oral cavity, provided that the child develops correctly, coincides with the period of loss of milk teeth. As a rule, replacement occurs in the same sequence as eruption during the formation of a temporary bite.
The first permanent teeth appear between 5 and 6 years of age. These are the first permanent molars that have no temporary predecessors. They are the first to undergo the process of calcification of hard tissues after the birth of a child. After this, premolars, second molars, central and lateral incisors, and canines appear.
If there are problems with resorption of temporary roots and other difficulties that prevent normal eruption, a baby tooth is removed and other dental care is provided. This takes into account the fact of genetic predisposition and other features of the child’s development.
According to WHO, the standard terms of development and eruption are:
- Central incisors. Mineralizes at 4-5 years of life. They appear in the mouth at 6-8 years of age, while root formation is completed only by 10 years of age.
- Lateral incisors . They erupt at the age of 8-9 years. Complete mineralization of the enamel occurs at 4-5 years of a child’s life, and the root system continues to develop up to 10 years;
- Fangs . Enamel mineralizes at 6-7 years of age. They emerge in place of temporary ones at 10-11 years of age and complete full formation at 13 years of age.
- First premolars. They undergo complete mineralization at the age of 5-6 years and appear in the mouth at 9-10 years. The root system of these teeth is formed by the age of 12.
- Second premolars . Mineralizes by 6-7 years. They usually erupt at the age of 11 years and complete development by 12 years.
- First molars . They are the very first permanent teeth. They mineralize at 2-3 years, erupt at 5-6 years and are fully formed by 10 years.
- Second molars . They appear in children at the age of 12-13 and complete development by the age of 15. Moreover, their intramaxillary growth and mineralization takes place in the period of 7-8 years.
The last permanent teeth to appear between the ages of 18 and 25 are the third molars. Their final development can last up to 30 years.
Diagnosis of torsion
Diagnosis of pathology consists of a clinical examination and additional research methods. At the first stage, a physical examination is carried out: the specialist determines the position of the teeth, the degree of displacement, the current inclination and / or inversion.
The second stage is radiological research methods: radiographs are prescribed to identify the causes of crowding and identify possible rudiments of extra teeth. The method is also effective for determining the current location of wisdom tooth buds and the extent of their presence.
To obtain the most accurate results, the results of computed tomography, teleroentgenogram and orthopantomogram are examined.
Teleradiogram is a panoramic radiography of the skull in frontal or lateral projection. The study allows you to study the profile, jaw and craniometric dimensions (parameters of the profile, joints and ratio of the skull bones), which are necessary for choosing therapy.
Orthopantomography (a circular panoramic image of the teeth) allows you to get an idea of the location and number of germs in the teeth, estimate the free space for teeth that have not yet erupted, and study the number of crowns, their angles, shape and size.
The curve or sagittal compensation curve must be measured. This is a line drawn along the cutting edges of the front teeth and the buccal cusps (cracks) of the chewing teeth. With crowded teeth syndrome, the severity of the curve of Spee increases and exceeds 2 mm.
In addition, biometric methods are used to assess dental shrinkage:
- The Pont method evaluates the degree of compression of molars and premolars. This method allows you to identify the cause of crowded teeth, as well as choose the optimal treatment method, taking into account the individual characteristics of a particular patient. The Pon method consists of comparing the transverse dimensions of the molar crowns of a particular patient with the average size.
- The Corkhouse method establishes the relationship between the length of the anterior region and the width of the incisors. The method consists of determining the length of the anterior part of the maxillary arch, which is then compared with the calculated individual norm. As a result, we can conclude that the dentition is lengthening or shortening. The length is measured along the middle jaw from the point between the central incisors to the intersection of the jaw with a line passing through the Pont measurement points.
- The Snagin method allows you to identify the causes of the syndrome and choose the optimal treatment method. It is based on measuring the width of the dental crowns, the arch along the premolar line and the parameters of the apical base (a conventional line running along the apex of the roots of the upper and lower jaw). If the lack of free space for teeth is associated with underdevelopment of the maxillary bones, a discrepancy occurs between the width of the apical base and the size of the mesiodistal teeth.
Polyodontia (supernumerary teeth) - symptoms and treatment
For a successful prognosis in treatment, high-quality and timely diagnosis of patients is very important. The dentist-therapist must know the basic clinical manifestations and principles of diagnosing hyperdentia. This is especially important in the work of a pediatric specialist during periods of medical examination and planned sanitation of the oral cavity in children. This makes it possible to identify the presence of this anomaly at an early age and carry out appropriate treatment in the early stages.
Most often, “extra” teeth are located in the anterior part of the upper jaw. The question of the exact location of supernumerary teeth is very important, since the surgical stage of treatment depends on this. The more accurately the position of various anatomical formations is determined, the less surgical trauma (damage to the growth zones of complete teeth, the formation of large defects in the bone of the alveolar process) will result from the surgical stage of treatment. The volume and time of the procedure will be reduced, which is very important when it comes to treating children. The position of the causative tooth can be determined using instrumental examination methods:
- CT scan;
- orthopantomography;
- intraoral radiography;
- visiography;
- Magnetic resonance imaging.
Computed tomography allows you to obtain a cross-sectional, layer-by-layer image of any area of the human body, including the skull. Dental (dental) X-ray computed tomography allows you to make 4 types of images in different planes in one and a half minutes. The radiation dose with this examination method is less than other types of CT. The procedure is easily tolerated by patients and does not require special training, which is convenient when working with children. In addition, it is as informative as possible for the doctor.
Orthopantomography is a method of x-ray examination in which you can obtain an image of all the patient’s teeth, upper and lower jaws, adjacent tissues and areas of the facial skeleton. Conducted for children from 3-4 years old. This is a quick, simple, highly effective method that helps identify oral diseases in the early stages. It has virtually no clinical contraindications and is actively used by dentists.
Intraoral radiography is the simplest, most common diagnostic method in therapeutic dentistry. The picture shows from one to 3-4 teeth and adjacent formations. For the pathology under consideration, the method is not informative enough, but can be used if the above types of diagnostics are unavailable.
Visiography is a system for obtaining X-ray images without the use of film. In this type of research, instead of film, a special sensor is used, from which the image is transferred to a computer, after which it is processed and then saved. Advantages of this technique:
- The radiation exposure to the patient is tens of times lower compared to the most advanced film X-ray, which is extremely important for both the patient and the radiologist.
- Scalability and the possibility of mathematical image processing (measuring the size, density of objects, etc.).
- It is possible to store the received information and create your own database for each patient.
- There is the possibility of instant transfer of diagnostic data directly from the treatment room to the computer monitor of the attending doctor, wherever he is. This is very convenient if you need to consult doctors from different clinics or from different cities.
But, as with intraoral radiography, the image produces a low-informative planar image of the area under study, limited to 1-4 teeth.
Magnetic resonance imaging is a radiation diagnostic method that can be used to obtain an image of the layers of the human body in any plane. The method is simple and does not have any harmful effects on the body of the subject. A contraindication for MRI is the presence of metal foreign bodies (dentures, braces, surgical pins, etc.) in the patient’s body.
Sometimes, to determine the level of location of problem teeth, Yu.I.’s technique Zhigurta (1994). It consists of studying an orthopantomogram of the jaws and marking on it the four levels of occurrence of unerupted incisors and canines. However, this method is imperfect and does not allow an accurate assessment of where the supernumerary tooth is located. It is more advisable to use modern diagnostic methods described above.
To more accurately determine the relationship of the additional tooth with the roots and rudiments of the complete teeth, contact intraoral radiographs are taken in the preoperative period and 1, 3, 6 and 12 months after the operation. They are used to determine the degree of change in the position of the impacted tooth, the condition of the root of the complete tooth and the morphological structure of the bone of the alveolar process in the studied area [1][7][8].
Treatment methods for crooked teeth
Modern orthodontic designs can successfully treat crowding. Based on the characteristics of the clinical picture of the pathology, one or another correction procedure may be indicated.
Braces
Most often, such treatment is justified if the pathology is not too serious. The course of correcting the defect will take several months; if you follow all the specialist’s recommendations, the effect of treatment is noticeable and lasting. For each patient, the time for using the systems is selected individually - it depends on the age group, the quality of the periodontal tissues and the presence of concomitant diagnoses. Various models of such structures allow you to align the jaw row due to the formation of an oval of the correct shape formed by an arch. Thus, abnormally overgrown organs end up in the right place.
Removal of a tooth
If there is insufficient free space in the row of the lower jaw, especially in the stage of a developed type of crowding, the patient has no choice but to resort to the removal of part of the organs. First, the outermost lateral teeth, also called wisdom teeth, are amputated. If the clinical situation is too advanced, sometimes even such a radical measure is not enough and the premolars must be removed. This mainly affects the lower jaw, since it is much more susceptible to deformation and mechanical stress than the upper jaw. Due to this, its natural size becomes a little smaller over time, and with such a diagnosis this is quite an aggravating factor. Depending on the severity of the disease, the course of treatment can range from 2-3 weeks to 1.5-2 months. After removal of all necessary organs, the installation of orthodontic structures is indicated. The cost of the removal procedure is standard and depends on the region, clinic and the cost of pain medication.
Extension
Such treatment will be effective only if the pathology is not very pronounced. It is carried out by lightly smoothing the enamel surface (mechanical separation principle) or installing spacers (physiological separation option). The first case is the opportunity to free up to 0.5 cm of the interdental space. It should be noted that many experts consider separation to be a fairly worthy alternative to amputation of jaw fragments. The procedure is carried out quickly, sometimes 2-3 visits to the dentist are enough.
Leveling devices are used for initial and moderate severity of anomalies.
- Aligners.
With the help of aligners, treatment proceeds much slower (within 1 year), but this procedure is much more comfortable for the person. The cost of structures is several times more expensive than braces, but the effectiveness of such treatment is much higher.
The principle of crowding relief is to apply light but constant pressure to the row of jaws. With the help of the habituation reflex, organ fragments are transferred to the correct position. There is a psychological “memorization” of the teeth in the desired position, which develops during the treatment process and is gradually corrected with each subsequent removable aligner. They are transparent and thin in appearance and are not difficult to wear. The course of treatment is about a year. Their cost is determined by the complexity of the correction and the number of aligners performed.
- Expansion of the dentition using plates.
Such manipulations are allowed only after a thorough study of the qualitative condition of periodontal tissues. The doctor records the presence of the amount of hard bone required for the procedure. The manipulation itself is carried out in several ways, but plates are often used. The effect is achieved due to the systematic pressure of the expansion plate on a number of jaws and gradually giving its fragments the correct position. Products are made individually. The best results in this case are observed in children and adolescents, whose bones are not yet fully formed and are more susceptible to changes in position than adults. Standard design: metal plate, mounting screws and spring. The devices are secured with clips. The course of treatment depends on the situation. Typically this is a period of 6 to 12 months.
Stages of dental development
There are four conventional stages of dental development in humans . The division into such periods is fair if we are talking about both milk and permanent teeth. MORE· The first stage is the laying of the beginnings of teeth. The formation of the dental rudiments of primary teeth occurs in the embryo in the sixth to eighth weeks of intrauterine development. First, an epithelial plate is formed, then enamel caps. The formation of the beginnings of permanent teeth occurs in the fifth month of intrauterine development of the fetus. The first to be laid are the incisors, then the small molars and canines. The last to be laid are the rudiments of the large molars (in the sixth month of the child’s life) and wisdom teeth – “eights” (only in the fourth or fifth year of the child’s life). · The second stage is differentiation. Differentiation of dental buds usually occurs at the twelfth (maximum fourteenth) week of fetal development inside the womb. During this period, cells are formed - builders of the surface tissue of the tooth (enamel) and cells - builders of dentin (the layer of the tooth located under the enamel). In medical science, such building cells are called adamantine blasts and odontoblasts, respectively. · The third stage is histogenesis. The next stage of dental development is histogenesis. This is the formation of hard dental tissues. The process of histogenesis begins in the fourth month of the baby’s intrauterine development. First, dentin is formed, and then the outer and most durable tissue of the tooth and the entire human body - enamel. · The fourth stage is the development of tooth roots . The development of the roots of both baby and permanent teeth begins after the baby is born. Typically, tooth root development begins shortly before tooth eruption begins. The development of tooth roots ends with the formation of the root apex - this occurs two years after the start of eruption.
Recommendations for using braces
Although braces can correct even severe crowding, it will take time and repeated visits to a specialist. In addition, the patient needs to change eating habits and pay more attention to oral hygiene.
- Brush your teeth under the orthodontic product. Orthodontists have developed a number of recommendations, compliance with which will make using the device more comfortable:
- Brushing your teeth after every meal is mandatory. The optimal solution would be to purchase a professional toothbrush, in addition to using dental floss and an interdental brush.
- Avoiding seeds and nuts while wearing braces. Particulate matter can damage the structure, resulting in the need for replacement. Care should be taken when handling any solid food: raw vegetables, fruits, meat fibers. It is not recommended to chew them - it is better to cut them into small pieces and chew them thoroughly.
- Excluding viscous products from the menu (caramel, nougat, chewing gum). They clog the grooves in the shoulder straps and are almost impossible to clean.
- Reasonable consumption of hot and cold drinks. A sharp change in temperature leads to thermal expansion of the metal elements, as a result of which the braces can peel off from the enamel.
- Regular visits to a specialist and immediate contact with him in the event of damage to the structure.
Additionally, caution should be exercised when consuming coloring foods and beverages while treating crowding. Coffee, strong tea, and soda can stain the transparent elements of the braces system and make it more noticeable.
After fixing the device, the patient may experience discomfort and pain in the jaw area during the first two weeks. Such manifestations are natural and should not cause concern. Over time, the discomfort disappears, and the bandage becomes familiar.
Modern designs are made from the most delicate materials, but soft tissue injuries may occur during installation. In order not to damage the gums, it is necessary to use plastic wax, provided in time by a specialist. If the mucous membrane is still red and swollen, it is recommended to use anti-inflammatory drugs until the wound is completely healed.
Forecast. Prevention
When treating crowded teeth syndrome, the prognosis is favorable in most cases. Thanks to the use of modern therapeutic methods, it is possible to restore the aesthetic appearance and functionality of the maxillofacial apparatus. The prognosis for restoration of the gums and maxillofacial area directly depends on the degree of development of crowding and the timeliness of contacting a specialist.
Depending on the degree of development of the patient’s pathology, the duration of full treatment ranges from 1.5 to 3 years.
If left untreated, plaque and tartar appear, and gingivitis, caries, and various periodontal diseases may develop. This leads to premature tooth loss.
The best method of prevention is a systematic visit to the dentist. The doctor at the appointment will help to timely identify negative factors, predisposition to anomalies and take measures to reduce negative consequences.