Formation of permanent teeth
Molars are formed from the epithelial dental plate. The appearance of their rudiments occurs only closer to the 5th month of fetal development inside the mother’s womb.
There are two groups of molars:
- Substitutes. This includes canines, incisors and premolars, which have temporary analogues.
- Additional. This group includes molars that do not have milk predecessors.
The growth of the primordial teeth of the replacement type occurs in the same alveolus as the temporary teeth; they are located behind the lingual surface of the primary teeth. Only after some time does the volume of bone tissue increase, ensuring their insulation.
Additional teeth are formed only after a year, since for this the jaw must reach the appropriate size.
Setting up teeth in children
The formation of the most important systems of the child’s body occurs in the early stages of pregnancy, when the woman does not even suspect she is pregnant. The unfavorable factors of this period, one way or another, leave their mark on the development of the baby, including teeth. Due to the increasing number of cases of dental diseases that develop even before teeth erupt, the intrauterine formation and development of a baby’s teeth is of great interest. Laying and formation of dental germs In the development of a child’s teeth, three stages, periods, which may be different from each other, can be distinguished. The first period is the actual formation and formation of tooth germs. The second stage is the differentiation of tooth germs; at this stage, a “distribution of roles” occurs between the tissues of the child’s teeth. The third , longest period is the formation of dental tissues and their complete “maturation”, i.e. mineralization. This period is the most crucial, since if the mother’s condition is unfavorable, or pregnancy complications occur, the child develops various dental diseases of the teeth, and not only. It's no secret that before erupting, teeth develop in the thickness of the jaw from the corresponding rudiments. Already at 6-7 weeks of pregnancy, when a woman has just learned about her pregnancy and begins to get used to her new status, the embryo already has a thickening of epithelial cells in the oral cavity, which gradually grows, it is in this thickening that flask-shaped growths appear - the enamel organ . As the name implies, these are the future baby teeth; there are 5 of them on each child’s jaw, for a total of 20. Don’t be surprised, in fact, when a child is born, there are 4 jaws in the mouth – 2 upper and 2 lower . Only after a period of time do the two processes of the jaw fuse with each other, and a single jaw bone is formed. At approximately 10 weeks of intrauterine development of the fetus, the enamel organ begins to change; cells of other tissue begin to grow into the cells of the enamel organ, due to which the outlines of the future crown of the baby tooth appear. With aggressive influence, the process of laying and formation of the rudiments of milk teeth may be disrupted, which may result in the absence of one of the teeth, or even a group of teeth. Differentiation of tooth germs This is a very important period, since changes occur both in the germs themselves and in the surrounding tissues. The fetal body is not a constant substance in terms of growth; throughout intrauterine development, active growth and differentiation of new cells, tissues and organs occur. At the same time, the period is quite short. Perhaps the most important stage in this period is the separation of the tooth germs from the connection with the epithelial plate. Thus, the tooth germs become isolated and begin to mineralize and develop. If this gap is disrupted, the connection or attachment of tissues to each other is maintained, tumor processes can subsequently form. During this period, which ends by the 16th week of pregnancy, the fetus may develop defects and anomalies in the development of the maxillofacial area, which, as a rule, can be diagnosed already in the first three months of pregnancy. Most often, intrauterine anomalies are represented by cleft lip and palate. Which are formed precisely as a result of non-fusion of the jaw bones. By the end of the second month of pregnancy, the embryo is practically formed, and the resulting defects and anomalies are less significant and are mainly a consequence of insufficient growth and development. Maturation of dental tissues This period begins by the 4th month of intrauterine development of the embryo; it is during this period that tooth tissues appear - enamel, underlying dentin and dental pulp. Initially, dentin is formed - this is the tissue that lies under the enamel. Dentin is an acellular tissue that has the shape of microscopic tubes filled with liquid. As dentin forms, enamel begins to form at the top - the hardest, and at the same time the most fragile tissue of the human body. Development begins with a small area at the site of the future cutting edge or tubercle of the tooth, since it is in this place that the enamel will be much thicker, and gradually the enamel covers the entire crown of the future baby tooth. The main feature of baby teeth is a thin layer of enamel compared to permanent teeth. This feature is due to intrauterine development. Already at the 5th month of pregnancy, the crowns of the anterior group of teeth are fully formed, and at the 7th month of pregnancy the crowns of the chewing group of teeth are formed. Until the moment of birth and teething, enamel and dentin continue to develop, accumulating in their composition the necessary microelements that are obtained from the mother’s body. The formation of permanent teeth occurs in the 5th month of pregnancy; it is this period of pregnancy that is considered indicative of the dental health of the unborn baby. Negative influences on the baby can affect the condition of not only milk, but also permanent ones. This effect can be expressed in the absence of one of the tooth buds, underdevelopment of tooth enamel, or its intrauterine damage. It is for these reasons that every pregnant woman needs to take care of her condition and regularly visit the doctor and follow all recommendations, especially in critical cases. Timing of mineralization of teeth Knowing the timing of mineralization of teeth, and comparing them with the negative effects during pregnancy, you can predict in advance certain dental diseases of the child, and take timely measures to treat and eliminate them. Recently, almost every 4 children in the oral cavity have teeth with underdeveloped enamel (enamel hypoplasia); it is difficult for parents to diagnose the disease, since the disease is quickly complicated by caries, which leads to early tooth loss. But, if you take the necessary measures in time, your baby’s teeth can be saved. The beginning of mineralization of baby teeth, namely the anterior group, occurs at 17–20 weeks of pregnancy, and in the presence of provoking factors, one can even assume a group of teeth that will be subject to changes. Fangs and chewing teeth begin to mineralize from approximately 7 to 7.5 months of intrauterine development and continues throughout the first year of the baby’s life. Mineralization of permanent teeth begins later, the anterior group of teeth begins its mineralization in the first six months of a child’s life, and the development of permanent teeth will no longer be influenced by the state of the mother’s health, but by the state of health, including the nutrition, of the baby himself. Mineralization of permanent chewing teeth begins from the age of 1.5 years and continues almost until the very moment of teething. Aggressive factors The formation and mineralization of primary teeth can be influenced by various factors, but most importantly, at different periods of development. Negative effects in the prenatal period, in the early stages of pregnancy, provoke the formation of congenital defects and developmental anomalies. Negative factors in the prenatal period include maternal gynecological pathology in the form of early toxicosis, chronic inflammatory diseases of the appendages, anemia of pregnant women, due to which the baby does not receive enough nutrients, vitamins and minerals, etc. Infectious diseases also have an impact, especially in the early stages of pregnancy - up to 12 weeks. Recently, vegetarianism has become fashionable, which is very harmful for the body of a pregnant woman and for the development of the child. A pregnant woman's diet should be complete and balanced! Don’t forget about the mother’s bad habits during pregnancy – alcohol and smoking. The influence on permanent teeth is most often exerted by factors that acted after the birth of the baby. This group includes malnutrition of a child - a lack of certain minerals, vitamins, etc. Mineralization of teeth begins from the cutting edge or tubercle of the tooth, and by the location of the affected enamel it is possible to diagnose at what period the pathological effect on the tooth tissue occurred, and vice versa. The condition of permanent teeth can be influenced by diseases of the endocrine system, disorders of phosphorus-calcium metabolism, such as rickets. A deficiency or, conversely, an excess of certain minerals also has an effect.
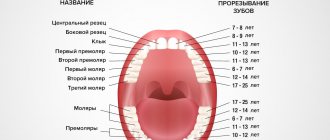
At what age do they appear?
Statistics show that the beginning and completion of the change from temporary teeth to molars in most children occurs at approximately the same time. There are minimal differences only among children in different regions. The warmer the climate, the sooner the child will have permanent teeth.
The table shows age parameters that can be used to determine the approximate beginning of the eruption of molars according to several well-known authors.
| Set of teeth | Period of eruption of permanent teeth in children (in years) | ||
| according to Vinogradova | according to Lukomsky | according to Novak | |
| Central incisors | 5-6 | 6-9 | 6-9 |
| Lateral incisors | 7-9 | 7-10 | 7-10 |
| Fangs | 12-13 | 9-14 | 9-14 |
| First premolars | 9-11 | 9-13 | 9-13 |
| Second premolars | 9-11 | 9-15 | 10-14 |
| First molars | 4,5-7 | 7-8 | 5-8 |
| Second molars | 12-13 | 10-15 | 10-14 |
| Third molars | 18-25 | 15-24 | 18-20 |
The differences in the age at which permanent teeth appear depending on the author are due to the fact that they present the results of studies in different regions that were carried out with a serious difference in time (several decades).
Timing and basic patterns of eruption of primary teeth.
MINISTRY OF HEALTH OF UKRAINE
Kharkov State Medical University
Characteristics of temporary, replacement and permanent dentition. Physiological types of bites.
Methodological recommendations for students of the Faculty of Dentistry and interns
Approved
Academic Council of Kharkov State Medical University.
Protocol No. ________
Kharkov, 2005
Characteristics of temporary replacement and permanent dentition. Physiological types of occlusions: Method. decree. for students / Comp. IN AND. Kutsevlyak, A.V. Samsonov, S.V. Altunina, Yu.V. Tkachenko. – Kharkov: KhSMU, 2005.- p./
| Compiled by: | IN AND. Kutsevlyak, |
| A.V. Samsonov | |
| S.V. Altunina, | |
| Yu.V. Tkachenko |
Over the course of a person's life, temporary and then permanent teeth emerge successively in the oral cavity. Knowledge of the anatomical structure, timing of teething, characteristics of growth and development of the jaws at different stages of the formation of the maxillofacial system, physiological occlusions is important for doctors of all specialties. This general morphological direction is basic and determines the patterns of development of the dentofacial system and reveals individual characteristics.
Timing and basic patterns of eruption of primary teeth.
A newborn child's jaws contain the rudiments of 20 temporary and 16 permanent teeth of various stages of development. The lower jaw is located behind the upper jaw, and between the alveolar processes in the anterior section there is a sagittal gap of up to 10 - 14 mm.
During the thoracic period, the intramaxillary formation and mineralization of temporary teeth continues, and from the 6th month the process of teething begins and a temporary bite is formed. At the same time, mineralization of permanent teeth begins.
The average age of teething is the age at which the tooth erupts in 50% of children.
It has been established that in a zone with a high fluoride content in drinking water, the eruption of lateral incisors, canines, and second molars begins 2-3 months later compared to a zone with a low fluoride content in drinking water.
The sequence of eruption of temporary teeth on each jaw occurs in the following order: I – II – IV – III – V, and in general in the occlusion as follows: Iн – Iв – Iв – Iн – Ivн – Ivв – IIIв – IIIн – Vн – Vв. The presented order of eruption is the most typical, however, options are also possible when the child’s lateral incisors erupt first, and soon after them the central ones.
Teeth usually erupt sequentially, in pairs, symmetrically. Violation of paired eruption is observed with malformations of teeth and jaws. It is considered normal when, by the end of the 1st year of a child’s life, 8 incisors have erupted, then the first molars, canines and second molars (Table 1).
Table 1
Timing of mineralization, eruption and formation of teeth
| Tooth formula | Temporary | ||||
| I | II | III | IV | V | |
| Bookmarking teeth | From 7 to 20 weeks of embryonic development | ||||
| Beginning of mineralization | 4,5 | 4,5 | 7,5 | 7,5 | 7,5 |
| In months of embryonic development | |||||
| Timing of eruption | 6 — 8 | 8-12 | 16 — 20 | 12 — 16 | 20 — 30 |
| In months of life | |||||
| Timing of root formation | Ko 2 | Ko 2 | K 5 | K 4 | K 4 |
| years | |||||
| Time frame for root resorption (beginning) | 4 — 5 | 4 — 5 | 8 — 9 | 6- 7 | 7 — 8 |
| years | |||||
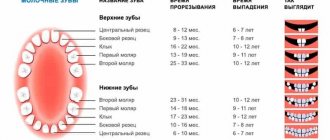
However, recently, due to acceleration processes, many children begin to erupt at an earlier time - 4 or 5 months of life, so some authors propose average periods of eruption, which were determined by them as a result of their own clinical studies (Table 2).
Table 2.
Average time for eruption of primary teeth
| Tooth | Child's age in months | |||||
| according to I.O. Novik | according to I.G. Lukomsky | according to AA Kolesov | according to A.I. Evdokimov and T.I. Albanian | according to N.I. Agapov | According to Eidmann cited. according to Kamnnek, 1968 | |
| I | 6-9 | 6-9 | 6-8 | 6-8 | 6-8 | 6-8 |
| II | 8-10 | 7-10 | 8-12 | 8-12 . | 8-12 | 8-10 |
| III | 16-22 | 15-20 | 16-20 | 16-20 | 16-22 | 16-20 |
| IV | 12-20 | 12-17 | 12-16 | 12-16 | 12-16 | 12-16 |
| V | 20-32 | 20-30 | 20-30 | 20-30 | by 30 | 20-30 |
Anatomy of primary teeth.
Temporary teeth differ from permanent teeth in size, shape, and color (Table 3).
Table 3.
Comparative characteristics of temporary and permanent teeth
| № | Sign | Temporary bite | Permanent bite |
| 1 | Number of teeth | 20 | 28 — 32 |
| 2 | Group affiliation | Incisors, canines, molars | Incisors, canines, premolars, molars |
| 3 | Crown size | Less | More |
| 4 | Height to width ratio | Width prevails | Height predominates |
| 5 | Color | White-blue | White-yellow |
| 6 | Transition of crown to neck | Sharp due to enamel roller | Smooth |
| 7 | The widest part of the crown | Cervical | Equatorial |
| 8 | Retention points | The fissures are shallow, there are no pits | Fissures and pits are deep |
| 9 | Expressiveness of tubercles in the crown | After 4 years they are normally erased | Children do not wash it off |
| 10 | Location of teeth in the dentition | Appearance of trema and diastema after 3 years | Normally there are no three or diastemas |
| 11 | Tooth mobility | Increases during the period of physiological resorption | No |
| 12 | Root location | In single-rooted plants there is a pronounced vestibular bend, in multi-rooted ones they diverge widely | Pronounced sign of root angle |
| 13 | Tooth Cavity Size | Relatively large, wide root canals | With age, the tooth cavity becomes smaller and the root canals become narrower. |
| 14 | Hard tissue thickness | Less | More |
| 15 | Degree of mineralization | Less | More |
| 16 | Presence of “immune zones” of enamel | No | Yes (lumps, cutting edges) |
| 17 | Structure of dentinal canals | Short, wide | Long, narrow, with anastomoses |
Among the temporary teeth there are: incisors – 8; fangs – 4; molars – 8. The teeth are not homogeneous in their structure. This depends on the group affiliation of the tooth, on the described surface of the tooth. For convenience of description, surfaces are distinguished: vestibular, lingual, medial, distal, occlusal.
The group of temporary incisors are single-rooted teeth. There are 4 incisors on each jaw: 2 medial (central) and 2 lateral (lateral), left and right, respectively. What is common in the structure of the incisors is the shape of the crown, flattened in the vestibular-lingual direction near the cutting edge. The root has a cone shape.
The group of temporary canines are single-rooted teeth. There are 2 fangs on each jaw: right and left. What is common in the anatomy of these teeth is the presence of a crown that is pointed on all surfaces and the longest cone-shaped root.
Group of temporary molars. These are teeth with a multi-tubercular chewing surface and several roots. Primary molars are the largest teeth in the primary dentition. The child has 8 molars: 4 molars of the upper jaw - first and second (right and left); and 4 molars of the lower jaw - first and second (right and left).
There are several systems for recording the dental formula of primary teeth.
| Anatomical dental formula of temporary teeth | I2C1M2, where I are incisors, C are canines, M are molars. | |
| Clinical formula according to Zigmondy | V IV III II I | I II III IV V |
| V IV III II I | I II III IV V | |
| Clinical formula according to WHO | 55 54 53 52 51 | 61 62 63 64 65 |
| 85 84 83 82 81 | 71 72 73 74 75 | |
There are three main periods in the temporary dentition: 1st period (from birth to 2.5 - 3 years) - formation of the temporary dentition; 2nd period (from 3 to 4 years) – formed temporary bite; 3rd period (from 4.5 to 5 – 6 years) – reduction (abrasion, wear) of the temporary occlusion.
The period of formation of temporary occlusion. With normal development of teeth and jaws, the process of eruption of temporary teeth begins at 6–8 months (Fig. 3), lasting up to 2.5–3 years. As teeth erupt and chewing function develops, involution of those organs that previously provided the act of sucking is observed. With the eruption of the second primary molars, the first rise in the height of the bite occurs. During this period, the alveolar process actively develops, the basal part of the lower jaw thickens, its branches grow, the outlines of the mandibular canal change, the size of the mandibular angle decreases, and the relief and architecture of the lower jaw become more complex.
By the age of 2.5 - 3 years, the temporary bite is considered formed . This period lasts up to 4 years and is a stable state of the dental system.
Violations in the primary occlusion can lead to various complications, both local and general. They affect the growth and development of the jaws, the eruption of permanent teeth, reduce chewing ability, and lead to
changes in the shape of the hard palate.
The period of formed temporary occlusion has the following dental characteristics: 1. There are 20 temporary teeth, they have a pronounced anatomical shape, 2. The teeth within the dentition have tight contact. The contact point is point-like, but with an increase in physiological mobility, by the end of the period of formed temporary occlusion, the contact point becomes planar. 3. the upper and lower rows of teeth have the shape of a semicircle and their midpoints coincide with each other; 4. The teeth of the upper jaw in the frontal region overlap the teeth of the lower jaw. This is explained by the greater width of the upper dental arch compared to the lower one; 5. each tooth of the upper jaw articulates with two lower ones, with the exception of the second molar, which articulates only with its antagonist - the second lower molar; 6. The distal approximal surfaces of the second temporary molars are in the same vertical plane.
By the end of the eruption of primary teeth, the first stage of physiological raising of the height of the bite , which begins with the establishment of contact between the first temporary molars and ends with complete eruption and correct articulatory relationships of the second temporary molars.
The next period of formation of the dental system is the period of reduction of temporary occlusion , lasting from 4.5 to 6 years. A fully formed temporary bite during this period is unstable and undergoes a number of changes. It is also called the period preceding the change in the temporary bite, or the period of “wear and tear” of the temporary bite. As a result of the growth of the jaw bones in preparation for the replacement of temporary teeth with permanent (larger ones), this period is characterized by the formation of physiological gaps between the teeth (diastemas - between the central incisors and three - between the remaining teeth). The abrasion of the cusps of the chewing teeth and the cutting edges of the frontal teeth gradually increases. The physiological mobility of individual teeth to be replaced increases. The dentition lengthens. Due to the abrasion of the chewing surfaces of the lateral teeth, a medial (towards the midline) shift of the lower jaw occurs and a “direct sliding bite” is formed. In this case, the incisors contact their cutting edges, and a medial step appears in the lateral area, formed by the distal surfaces of the second temporary molars (Tsilinsky’s symptom).
This relationship of teeth ensures the subsequent correct position and relationship of the first permanent molars. The spaces of primates (diastema and trema) are a reserve site for the medial displacement of the lower dentition and the subsequent unimpeded placement of permanent teeth. Wearing of teeth leads to a decrease in the height of the crowns, and a straight “sliding” bite is formed. The differentiation of the elements of the temporomandibular joints is completed, the formation of third molars, the development and mineralization of premolars and second molars continues. Towards the end of the period of “wear and tear” of the temporary dentition, the eruption of the first permanent molars begins.
Teething sequence
Almost all parents believe that the first molars should be incisors, which replace temporary elements of the dentition. But this opinion is wrong. Even before baby teeth fall out, at the age of 5-6 years, children receive their first molars, which are not on the list of primary teeth.
After this, the sequence of formation of a permanent bite is almost no different from the order of eruption of primary teeth:
- the lower and upper central incisors grow;
- lateral incisors appear on both jaws;
- lower and upper first premolars;
- fangs;
- upper and lower second premolars;
- second and third molars (you must understand that the so-called “wisdom teeth” sometimes do not penetrate the surface of the gums at all).
Teeth cutting in this order does not happen just like that, because it ideally corresponds to the speed of development and formation of the maxillofacial system. If the optimal sequence is followed, correct bite development occurs.
Duration of growth
Typically, children say goodbye to their last temporary teeth at about 12-13 years of age, although the roots of baby teeth dissolve even earlier. By that time, the oral cavity already has molars that are actively growing, and their roots are at different stages of formation.
It is necessary to understand the approximate timing of growth and root formation in case of deviations. It is these indicators that are taken into account when choosing a treatment method.
Experts distinguish two main stages of development of the roots of permanent teeth:
- Stage of unformed apex.
- Unclosed apex stage.
At the first stage, the length of the root becomes maximum, but its walls are parallel to each other. The channel is of sufficient width; it ends in the area of the future apex with a bell. The periodontal gap can be seen only on the sides of the tooth root.
At the next stage, there is a gradual formation of the upper part of the root, the convergence of the root walls and the release of the periodontal fissure, the apical region of which is slightly enlarged.
Root canal treatment in children
The roots of children's baby teeth are filled with a special paste. It has the ability to dissolve in parallel with the process of resorption of hard tissues. This is the only way to ensure that the order of changing teeth is not disrupted and that there are no obstacles to the resorption of milk roots.
Once the root canals are treated, they are closed with a filling. Sometimes the doctor decides to use temporary filling material. This measure is justified if the likelihood of complications is high and you need to make sure that the inflammation has subsided. Only when the dentist is sure that everything is in order will he install a permanent filling.
The completion of tooth root formation occurs at approximately this age:
| Teeth | Upper jaw, age | Lower jaw, age |
| Central incisors | 9-13 | 7-11 |
| Lateral incisors | 9-12 | 8-11 |
| Fangs | 9-12 | 9-12 |
| First premolars | 11-13 | 11-13 |
| Second premolars | 11-13 | 11-13 |
| First molars | 9-12 | 9-12 |
| Second molars | 14-15 | 14-15 |
Since the eruption of third molars does not occur at a specific time, it is impossible to establish a clear age at which their roots are formed.
X-ray results confirm the completion of the process of tooth root formation. The key signs are the absence of an opening at the apex, as well as a pronounced periodontal contour.
Thus, completion of dental growth, including full maturation, usually occurs only between the ages of 15 and 18 years. It is at this time that the maxillofacial apparatus already has the same dimensions as in adults.