Composition of tooth enamel
Dental enamel is the most durable, wear-resistant and hard component in the human body. It represents the outer or surface layer of the teeth, completely covers its coronal and partially cervical part, and also performs protective functions. The main characteristics of enamel include:
- The color of tooth enamel varies from white to yellowish, and it can change shade (color) depending on a person’s dietary habits or bad habits.
- The thickest areas of enamel cover the chewing molars in the area of their anatomical tubercles; their thickness varies between 2.3-3.5 mm;
- The thinnest areas of tooth enamel are localized in paroxysmal areas (places of contact in their lateral projection), here the thickness of the protective layer reaches approximately 1.3 mm;
- The enamel that covers all the teeth in the human oral cavity is not capable of regeneration, because there are no living cellular structures in the tissues of this protective layer;
- Depending on the characteristics of each person’s body, up to 95% of the chemical composition of tooth enamel is presented in the form of mineral compounds. The remaining percentage is divided between water and organic matter in approximately a 2:1 ratio, respectively. In addition, depending on the percentage of mineral content of tooth enamel, it can be more or less transparent (the higher the percentage of minerals, the more transparent the enamel becomes).
Other components in the enamel
In addition to the already mentioned main components of the enamel layer of the tooth, its chemical composition also contains a set of other components:
- Neonatal line - present exclusively on baby teeth, it looks like a dark-colored stripe (almost black). This line is located in the area of contact between two types of enamel, the first of which was formed before the baby was born, and the second after.
- Bundles and plates of dental enamel are special enamel formations containing prisms of a hypomineralized type, between which the interprismatic substance consists of the same material. It is noteworthy that the molecular structure of this material involves a large number of protein compounds. Many dentists are of the opinion that through the mentioned bundles and plates, various microorganisms penetrate into the enamel from the oral cavity, making their way to deeper dental tissues, causing caries, etc.
- Gunter-Schräger stripes are lines that stand out on the tooth enamel in a darker or lighter shade, the width of which does not exceed 100 microns. They are located perpendicular to the surface of the enamel layer and are formed as a result of opening its prisms.
- Retzius lines - in shape they resemble arches offset from the central one, located symmetrically in relation to each other. When cut across a tooth , these formations resemble rings inside a tree trunk. The formation of Retzius lines corresponds to different periods of mineralization of the enamel layer.
Tooth root cement: structure
Cement is close in chemical composition and strength to coarse-fiber bone tissue. Inorganic components in the composition of cement make up approximately 65% - mainly calcium phosphate (in the form of hydroxyapatite crystals or amorphous calcium phosphates) and calcium carbonate. Organic components make up about 23%, and they are almost entirely represented by collagen; plus about 12% water.
Cementum is divided into 2 forms - primary (acellular) and secondary (cellular). A layer of primary cement lines the dentin of the entire surface of the tooth root, and in turn, a layer of secondary cement will be located on top of it. However, this so-called secondary “cellular cement” will no longer cover the entire surface of the root, but only its apical third + in multi-rooted teeth, also the area of bifurcation/trifurcation of the roots (Fig. 4).
Cement layers (electron microscopy) –
Cellular and acellular cementum (histology) –
1) Primary (acellular) cement –
Primary cement covers the entire tooth root. It does not contain cells, and consists only of calcified intercellular substance, which includes collagen fibers and the main amorphous “gluing” substance. The collagen fibers of this cement layer are characterized by uniform mineralization, and some of them have a longitudinal direction - in relation to the root surface, and some - a perpendicular (radial) direction. The latter are called "Sharpey's fibers", and they are very important for fixing the tooth in the alveolus.
2) Secondary (cellular) cement –
Secondary cement is formed after tooth eruption, and it no longer covers the entire surface of the root, but only its apical third + the area of furcations of multi-rooted teeth. It can be placed either on top of the primary cementum or directly adjacent to the root dentin. Secondary cement consists mainly of cells (cementocytes and cementoblasts), as well as intercellular substance, which in turn consists of the main amorphous substance and randomly directed collagen fibers.
- Cementocytes (Fig. 5-6) - lie on the surface of the cement in special lacunae (cavities) and in their structure they are very similar to cementocytes of bone tissue. Cementocytes have long processes, and where the cellular cement is directly adjacent to the surface of dentin, the processes of cementocytes can directly contact the dentinal tubules. When new layers of cement are formed, the cementocytes of the inner layers gradually die, forming empty lacunae in the cement.
- Cementoblasts - these cells are “cement builders”, i.e. ensure the deposition of more and more of its layers. The deposition of cement by cementoblasts occurs throughout a person’s life, and therefore the thickness of cement in the area of the root apices increases several times towards the end of life.
Cementocytes in secondary cementum (histology) –
Fig. 6 (designations), where 1 – cementocyte, 2 – dentinal tubules, 3 – contacts of cementocyte processes with dentinal tubules.
3) Collagen fibers –
The most important part of the collagen fibers of cement are the so-called “Sharpey fibers”. They are the terminal sections of the fibers of the periodontal attachment of the tooth on the cementum side. In Fig. 7 you can see a histological specimen, which shows that the radial collagen fibers of the periodontal fissure and cementum of the tooth root are “a single whole.”
Connection of periodontium and cementum of the tooth root –
Previously, it was believed that the radial fibers of the periodontium (which on one side are fixed to the compact lamina of the alveoli, and on the other to the root cement) were a single whole. But modern research shows that this is not entirely true. The terminal sections of the dento-alveolar fibers of the periodontium begin to form separately from each other: one part - from the side of the cement of the tooth root, and the other part - from the side of the alveolar bone plate.
And when both parts of the fibers reach the middle of the periodontal fissure, they are connected through immature collagen fibers (procollagen fibers) into a single network. The plexus of immature collagen fibers in the center of the periodontal fissure is called the “Siecher plexus” (24stoma.ru).
Summary:
| Acellular (primary) | Cellular (secondary) | |
| localization | – adjacent to dentin, – covers the root. | – covers acellular cement in the area of the apical third of the root and the furcation area of multi-rooted teeth. |
| structure | – collagen fibers (longitudinal and radial arrangement), – amorphous substance, – growth lines are located close to each other. | – cementocytes in lacunae (their processes anastomose with each other), – collagen fibers (chaotic direction), – amorphous substance, – growth lines are located relatively far from each other. |
Dental cement: histology
Below in video 1 you can see the histology of tooth tissue in stunning resolution. Video 2 is the best lecture on cement histology you can hear. The video is in English, but if you wish, you can turn on subtitles, and then select translation from English into Russian in the settings.
Features of the structure of the enamel of baby teeth
The main distinguishing feature of the enamel layer of children's teeth is that it is less durable and also much thinner than the enamel of permanent teeth. This is explained by the lower content of mineral compounds in teeth in relation to water and organic substances. Considering these features, if you examine baby teeth and their enamel layer under a microscope, you will notice the following differences:
- Due to the fact that the service life, as well as periods of mineralization and the tendency towards this process are shorter, the Retzius lines are much less pronounced in the structure of primary dental units.
- If in permanent teeth enamel prisms are located apically, then in milk teeth their direction is completely different, they are located horizontally.
- In children's primary teeth, the final enamel layer is much less pronounced; prisms are clearly visible on its surface, while its structure is much more porous, with microscopic cracks present.
Under the influence of each of these features, tooth enamel in children is more susceptible to wear and damage. For this reason, children develop caries much more often and it progresses faster, which is why it is important to visit the dentist regularly and have their teeth treated in a timely manner.
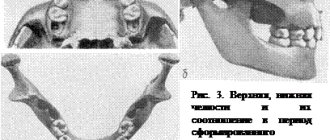
Intramaxillary development
The first stage of formation of temporary teeth begins at 6-8 weeks of embryogenesis and lasts until the middle of the first year of a child’s life. It includes the following processes:
- the formation of a dental plate from multilayered squamous epithelium located in the oral fossa of the embryo with the further formation of a ridge and the growth of tooth buds in the form of flask-shaped buds;
- the formation of epithelial (enamel) organs due to the ingrowth of mesenchyme into the kidneys with the subsequent formation of dental papillae and sacs;
- histogenesis of dental tissues (formation of dentin, formation and mineralization of enamel, development of pulp from the mesenchyme of the dental papilla with the formation of nerve fibers and blood vessels).
Each newborn has inside both jaws the rudiments of all 20 temporary and 16 permanent teeth, which have varying degrees of development and mineralization.
Types of damage to tooth enamel
Over the course of life, even if you provide your teeth with proper care and follow the rules of oral hygiene prescribed by dentists, the enamel layer gradually wears out and is destroyed. This contributes to the occurrence of various diseases of the oral cavity; it is influenced by the food a person eats, etc.
Among the main causes of damage and destruction of tooth enamel, dentists identify:
- Erosion is damage to the enamel layer, and then dentin, which is not associated with carious lesions of the teeth . The essence of this pathological process lies in disorders of mineral metabolism. As a result, disturbances occur in the crystalline structure of the enamel, which is manifested by its focal thinning and destruction. Externally, erosions look like local darkening on a round or oval tooth. The occurrence of erosions is provoked by the consumption of foods with high acidity levels, pathologies of the gastrointestinal tract, the use of certain medications, and the use of aggressive tooth powder or paste.
- Excessive sensitivity of tooth enamel - this disorder is especially pronounced in the form of painful sensations when the teeth cold or hot food, drinks, and even as a result of contact with cool air. The sensitivity of tooth enamel develops due to its thinning under the influence of the factors already described above. A thinned enamel layer puts teeth at increased risk of caries and other dental pathologies.
- Necrosis - this term characterizes multiple lesions of the hard tissues of the tooth, especially the enamel layer and dentin. The pathological process is initially expressed in the appearance of small light spots on the surface of the tooth , which subsequently darken and deepen. The progression of pathology threatens tooth destruction and is accompanied by a number of other oral diseases. The main reasons for the development of necrosis include gastrointestinal diseases, hormonal imbalances, metabolic disorders in the body, and work in hazardous industries.
- Caries is a carious lesion that threatens teeth , primarily affecting the enamel layer of the structure , gradually destroying it and spreading to deeper tissues. There are many reasons for the development of caries, from non-compliance with the rules of oral hygiene and irregular tooth brushing, to pathologies of the structures of the oral cavity, diseases of the gastrointestinal tract and metabolic disorders. If you start caries treatment at the stage when the lesions have affected only the enamel layer, you can only get by installing a filling or even restoring the enamel. But progressive caries is dangerous for teeth due to destruction, which may lead to the need for its complete removal.
- Mechanical damage - due to the fact that the main function of the enamel layer is to provide protection to the teeth , it primarily suffers from the effects of external adverse factors. Mechanical damage to the enamel includes cracks and other violations of its integrity due to blows, bruises, eating too hard food, etc. If the enamel of at least one tooth has been subjected to aggressive mechanical action, you should consult a doctor for an examination and, if necessary, subsequent treatment.
- Wedge-shaped defect – this term characterizes the pathological process in which the area of the dental neck is exposed. In such cases, the thinnest and most vulnerable areas of the enamel layer, located at the base of the teeth, are negatively affected. In addition to visible receding gums, damage to the enamel is indicated by a change in its color, as well as an acute reaction to hot and cold.
Tooth for tooth
People made their first attempts at dental treatment a long time ago. During excavations in Egypt, archaeologists discovered an artificial tooth carved from a mollusk shell in the jaw of a man who lived five and a half thousand years ago (Fig. 1) [2].
Figure 1. View of the vestibular surface of a tooth cut from a shell. The interval of marks along the edges is 1 mm.
[2]
In addition to the “seafood tooth,” they found reimplanted teeth in the jaw of a young woman, and all of them were out of place: instead of the upper central incisor, the alveolus contained a fang. These teeth had all the signs of integration, that is, fusion with living tissue [3]. Thus, it turns out that already at this time the first steps were taken in dentistry, but, more surprisingly, also in the field of tissue engineering.
But, you ask, how can dentistry and tissue engineering be related, apart from the fact that several thousand years ago an Egyptian valued his smile so much that he replaced a lost tooth with someone else's? They very well may, because at the moment there is no panacea for treating a patient who has been diagnosed with partial or complete adentia , that is, lack of teeth. In addition, the loss of even one tooth leads to changes not only in aesthetic parameters, but, more importantly, to disruption of primary food processing and deterioration of speech. We should also not forget that when teeth are lost - whether as a result of injury or caries and its complications - the condition of the dental system as a whole changes, which worsens the prognosis and complicates further treatment.
In order to compensate for the functions of a lost tooth, orthopedic structures and implants are now used (Fig. 2). Still, these are “artificial” substitutes: they lack blood vessels, nerve endings, and receptors. Also one of the most important aspects is the absence of the periodontal ligament in the implant, which until recently was considered the gold standard of treatment for missing teeth.
Figure 2. Structure of the tooth and implant. Natural tooth - tooth. Artificial crown - artificial crown. Gingiva - gums. Implant - implant. Osteointegration - osseointegration. Periodontal ligament - periodontal ligament.
website www.neoclinique.ro
The periodontium is a highly specialized fibrous connective tissue composed of cells and extracellular matrix. It is located between the cement that covers the root of the tooth and the bone tissue that forms the wall of the socket. In humans, the periodontal ligament helps strengthen the tooth in the alveolus, provides mechanical resistance to the effects of chewing forces on the tooth, distributing the applied pressure: the force of all masticatory muscles is no less than 390 kg [4].
What's wrong with the implant?
Firstly, as already described above, there is the absence of the periodontal ligament. The implant is retained due to osseointegration, that is, through an anatomical connection with bone tissue. Unlike a tooth, which has little physiological mobility, an implant is immobile. If a semblance of connective tissue appears around the implant, then this means only one thing - peri-implantitis , that is, an inflammatory process in the bone tissue surrounding the implant. In most cases of this scenario, the implant must be removed [5].
Secondly, the implant cannot be connected into a common structure with the patient’s remaining teeth due to the lack of ligamentous apparatus and the inability to adequately distribute pressure. The principle works here: whoever is stronger is in the dentition. Either the implant will not allow the tooth to move, which will lead to atrophy of periodontal tissue and tooth loss, or the implant will be lost.
Thirdly, each patient has its own anatomical features, and the volume of bone tissue for placing an implant is not always sufficient.
And fourthly, it is important to remember that for the longevity of the implant it is necessary to maintain ideal oral hygiene, which, to put it mildly, is not possible for everyone. Here we return to the previously mentioned problem of peri-implantitis [5]. It turns out to be a kind of vicious circle.
All these disadvantages lead to the search for alternative treatment methods.
One of them could be tissue engineering. In this article, I will try to summarize the recent progress, prospects and main directions of development of dental bioengineering, that is, briefly talk about what it takes to create a tooth.
Strengthening tooth enamel
Today in dental practice there are many effective ways to strengthen the enamel, which allows you to maintain its integrity and prevent destruction and diseases of the dentition. At the same time, methods of strengthening and protecting the enamel layer are divided into two groups, the first are intended for adults, the second for children.
Strengthening baby teeth enamel
As was said earlier in relation to baby teeth, their enamel is more vulnerable. To protect it, saving the child from premature loss of dental units and problems in the future, doctors perform the following actions to provide temporary protection:
- Fluoridation involves treating teeth with special fluoride-based compounds; it is recommended to repeat this procedure 2-3 times a year.
- Fissure sealing - the dentist performs the procedure of filling the recesses and grooves of chewing teeth with temporary filling material, protecting the dental structures from the negative effects of harmful microorganisms and other unfavorable factors.
- Application gels and preventive mouth guards for teeth - the method is based on enriching the enamel layer with useful components (fluorine, calcium, vitamins) through the use of special products.
Periodontal and root formation
This stage of development of temporary teeth precedes their eruption and continues 1-.5-2.5 years after the completion of this process. The crowns are usually already fully formed by this time. The place of root origin is Hertwig's epithelial sheath, consisting of external and internal cells of the enamel organ.
The process of development of the root system and periodontium includes the following stages:
- ingrowth of epithelial cells into the underlying mesenchyme;
- separation and formation of a channel of a certain shape;
- formation of root dentin with the participation of odontoblasts;
- development of cement on the surface of dental dentin;
- formation of dense periodontal tissues by fibroblasts;
- fixation of the root with collagen fibers to the alveolar bone;
- formation of secondary cement on the basis of primary cement after eruption.
Strengthening the enamel of molars
There are more methods to preserve molars and maintain the condition of their enamel layer. Firstly, this is due to fewer contraindications for adults. Secondly, molars require long-term strengthening.
The main methods of strengthening the enamel of permanent teeth include:
- Drug therapy is based on the use of vitamin complexes containing vitamins of groups B6, B12, D. In addition, the patient is selected drugs that promote better absorption of calcium and fluoride by the body.
- Special gels and oral hygiene products – this technique uses specialized toothpastes and gels containing components necessary for teeth to strengthen and maintain the condition of the enamel layer. Also, teeth are subjected to unimaginative cleaning in a dental office.
- Mineralization and preventive cleaning – mineralization is performed using special means to increase the strength of the enamel and reduce its susceptibility to a number of negative factors. As for cleaning, such procedures are performed by dentists in the clinic using special equipment. During cleaning, plaque and tartar are eliminated , pathogenic bacteria and microorganisms that can harm the enamel layer are removed.
- Home prevention - to maintain healthy teeth and enamel, patients are advised to perform a light massage of the gums, enrich the diet with fresh vegetables and fruits rich in vitamins.
Author: Zhukov M.A.