The process of building and erupting baby teeth in children is quite painful and, as a rule, these features cause inconvenience not only to the baby, but also to his parents. Symptoms include redness and swelling of the gums, as well as crying and problems with appetite. Prepare for sleepless nights if you also notice short-term redness and a rash on your child's lower lip and chin. Unfortunately, a more severe process is also possible, accompanied by an increase in temperature. How are baby teeth structured, how long does it take for them to appear, and what should parents do during this difficult time? We will discuss this in this article.
The structure of the tooth.
A tooth is a bone located in the alveolar process of the jaw and consisting of various hard tissues (enamel, dentin, cement) and soft tissues (dental pulp). Anatomically, the following parts of the tooth can be distinguished:
- crown of the tooth (the part of the tooth protruding above the gum);
- tooth root (part of the tooth located in the jaw);
- neck of the tooth (a conventionally distinguished part of the tooth, which is a transitional area from the crown of the tooth to the root, covered with a thin layer of enamel)
The crown of the tooth is covered with enamel, the hardest tissue in the body, consisting of hydroxyapatite crystals. Beneath the enamel is a softer, more porous tissue called dentin. On the crown of the chewing tooth there are tubercles and fissures. Fissures are natural depressions on the chewing surface of the teeth between the cusps. Deep fissures are often the cause of the development of the carious process, because... a lot of plaque remains in them.
Inside the tooth there is a cavity containing pulp. The pulp of a tooth, in common parlance, the “nerve” of a tooth, is a neurovascular bundle consisting of blood vessels and a nerve. The neurovascular bundle provides nutritional function and replenishment of the composition of tooth tissue.
Each group of teeth differs in their structure, shape and function:
- incisors - involved in biting off food;
- fangs - provide “tearing off” and holding food;
- molars and premolars - are involved in grinding food to create an optimal digestive bolus.
Why do baby teeth sometimes have to be removed?
As was written above, most often such teeth can be removed without resorting to professional help. However, sometimes there is still a need to visit the dental office. Before we look at the reasons why you have to seek help from dentists, let's talk about the location of the dental nerve. It is located quite deep in the tissues. The enamel provides it with reliable protection from external influences.
Why does the body need to protect the dental nerves? This can be explained quite simply:
- nerve endings that are located in the pulp must always be sterile. After all, they have a connection with the general blood flow;
- Temperature changes, acids, alkalis negatively affect dental nerves. If they are exposed, the person begins to feel unbearable pain. Therefore, to relieve a person from pain, it is necessary to protect the nerves well;
- a tooth can perform its assigned functions only if the pulp is not affected by external factors.
From the above we can conclude that any violation of the integrity of dentin can lead to the removal of nerves. But is it possible to remove the nerve in a baby tooth? Will this have negative consequences? Removing the nerve is a safe and sometimes necessary procedure. The most common reasons for removing nerves from teeth are:
- pulpitis – is an inflammatory process that occurs in the pulp tissues;
- caries (deep) – thin enamel is not able to fully protect the tooth from the negative effects of harmful microorganisms. This is why the carious process quickly affects the tooth and spreads almost instantly;
- periodontitis - quite often children, afraid of a visit to the hospital, hide from their parents that the tooth hurts. Gradually, such neglect turns into a disease. Periodontitis develops, which occurs at the junction of the tooth and gum;
- Tooth trauma – trauma can cause damage to the enamel. In the future, this becomes the reason for removing the nerve.
Teething in children.
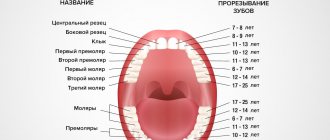
Diagram and table of timing of eruption, location and loss of baby teeth in children
In humans, like almost all mammals, teeth erupt twice during life. The first teeth that appear in a child at the age of 6 - 9 months are called “milk” because of their color, as they have a soft white (milky) color.
Before appearing in the oral cavity, the tooth stretches the mucous membrane (the tooth can be easily felt with a finger), after which it breaks through it and appears in the oral cavity. In some children, a small bluish “bump” with transparent contents forms in the place where the baby tooth is about to erupt. This is an eruption cyst that forms over the future tooth. Despite the menacing name, in most cases, this goes away WITHOUT intervention from a doctor. The cyst breaks through and the long-awaited tooth appears. The cutting of a child’s first teeth is always a special and joyful event for parents, but it is often accompanied by unpleasant sensations and itching of the gums: therefore, the child is capricious and whiny, may sleep poorly, and puts everything in his mouth to “scratch” the gums and speed up the teething process. There may even be a slight increase in body temperature in a child due to teething. To represent the sequence of teeth erupting in a baby’s mouth, a diagram of the eruption of baby teeth in children is given. You can learn more about the sequence of eruption and replacement of baby teeth by reading the article “Teeth in children from 0 to 3 years old. When do children’s first teeth appear and cut?”
At the age of five years, the gradual replacement of milk teeth with permanent ones begins: under the “pressure” of new permanent teeth, the roots of the milk teeth dissolve and the milk tooth falls out (more precisely, the crown of the tooth falls out, since the root has dissolved). This is why, after a baby tooth falls out, it has no roots—hence the popular belief that baby teeth have no roots. At five years of age, the first permanent chewing tooth behind all the baby teeth is often the first to erupt. Parents often perceive this tooth as a milk tooth, since its eruption is not accompanied by the loss of any milk teeth: it seems that the child has 24 milk teeth.
The replacement of baby teeth with permanent ones is completed at the age of 13 years. By this age, a child usually has 24 teeth in his mouth, 6 teeth on each side of the jaw: central and lateral incisors, canine, first and second premolars and a molar. Next, the teenager’s second and third molars erupt. The latter is often called the “wisdom” tooth and it does not erupt until the age of 17–18 years. In some people, wisdom teeth do not erupt at all, as they are rudimentary.
Difference between baby teeth and permanent teeth.
PHOTO: Caries of primary front teeth. The enamel of baby teeth is thinner and less mineralized, which makes it less resistant to caries.
Unlike permanent teeth, the “lifespan” of primary teeth is much shorter. Resorption of tooth roots begins 2-3 years after their eruption in the oral cavity and continues until they fall out.
Contrary to popular belief, baby teeth, just like permanent teeth, have roots and a nerve (pulp). The roots hold the tooth in the bone. Under the milk tooth is the germ of a permanent tooth. As the permanent tooth erupts, it stimulates the resorption of the roots of the baby tooth, and by the time the baby tooth falls out, only the crown remains.
Since baby teeth (like permanent teeth) have a nerve (pulp), they can hurt if an infection from a carious cavity enters the tooth cavity, causing the development of pulpitis (inflammation of the nerve of the tooth).
392measures and structure.
- Primary teeth are smaller than permanent teeth and have less massive roots;
- Baby teeth have a more complex anatomical structure of root canals, which leads to a more labor-intensive treatment process than in permanent teeth;
- The hard tissues of primary teeth are less mineralized and less resistant to abrasion and the development of caries.
- the hard tissues of baby teeth are much thinner than those of permanent teeth: the inflammatory process quickly reaches the nerve of the tooth;
How does caries work in a child?
The most acute form of caries. Please note that there is no usual dark coloring. Fabrics simply fall apart faster than they can accumulate pigment.
The course of caries in children is radically different from that in adults. They have weakly mineralized enamel and very loose, permeable dentin. Bacteria that synthesize organic acids consume the tissue of baby teeth at an incredible speed, if only they have managed to gain a foothold. Classic chronic caries almost never occurs in children. Chronic caries is when it develops so slowly that it manages to be stained by tea, coffee, cigarettes and borscht. The result is the classic, familiar black dots on the teeth. If you probe them, they give in, but are still quite dense. But children have uncolored caries. Can not get in time. When probing, it resembles rotten wood, which crumbles into layers under the instrument. As a result, it can take a little more than a month from the beginning to the complete fracture of the crown.
Because of its tenderness, children's enamel is especially vulnerable to the malicious microflora of the oral cavity of adults. The worst scenario is when a grandmother or grandfather with a mouth full of carious teeth tries to see if the child’s food is hot with his own spoon. As if there is no other way to measure temperature. It would be better to even dip your finger. Therefore, make sure that the child has his own separate spoon, which no one but him uses.
Very often, when caries is identified, the question arises about the advisability of treatment. “Let’s get through it, it’s still milky! I had all my teeth pulled out when I was a child, there’s no point in treating it anyway.” You look at your mother, and there is an impressive malocclusion and defects in the development of the jaws. In fact, there is no point in removing a carious tooth without any additional action if it is about to change anyway. In other cases, there are two options: we either treat fully, or we remove a completely hopeless tooth, but come up with a temporary structure to close the defect. Baby teeth take longer to work than they think. The same fangs change at 12–14 years of age! And without them, the bite will simply move away and become asymmetrical. There will be inevitable deformities and joint problems.
It is also impossible not to treat. This is simply dangerous. The infection will go deeper and can destroy the germ of the permanent tooth under the diseased milk tooth. In a very severe case, the infection can result in phlegmon, mediastinitis and sepsis. There are very wide spaces for its distribution throughout the fatty tissue.
So, given the speed of spread, there cannot be any options of “let’s continue like this for a couple more months.” Moreover, there is already excellent anesthesia, and masks with nitrous oxide, and sevoflurane, if the case is advanced and more than 10 teeth have to be treated at a time. Fortunately, a well-working team can carry out such a large-scale treatment in just a couple of hours. If you are interested, you can look at one of the previous posts, a colleague there spoke in detail about nitrous oxide and anesthesia.
Why are baby teeth needed?
Milk teeth are involved in the development of functions in the child such as chewing and pronunciation of sounds. Without them, chewing hard food would be impossible. The aesthetic component plays an important role.
Also, baby teeth hold space in the dentition for permanent teeth. The eruption of primary teeth stimulates the primary growth of the jaws. The second wave of jaw growth begins during the period of replacement of baby teeth with permanent ones. Early removal of primary chewing teeth leads to the displacement of neighboring teeth into the area of the missing one and the formation of crowding of teeth in the future!
Features of the structure of the roots of permanent teeth
Patients over 7-10 years of age usually have a fully formed root canal system. However, for a child with permanent teeth whose parents have made an appointment with a pediatric dentist, the formation process may not be complete. In this case, the canals will have some features that are important to take into account when carrying out endodontic treatment. Common features for permanent teeth are the location of the root orifices under the tops of the crown tubercles. Another characteristic feature is the increased cut diameter in the bucco-oral direction compared to the mesiodistal one. Physiological narrowing is usually located at a distance of 0.5-1 mm from the anatomical opening. Also, permanent teeth have a system of lateral canals, which are located at different levels from the main ones.
In cases where the process of root formation has not yet been completed, the patient exhibits the following features:
- absence of replacement and secondary dentin;
- large volume of pulp and intradental cavity;
- smooth transition from the crown to a wide canal in single-rooted teeth;
- low degree of mineralization and small thickness of the canal walls;
- a significant amount of predentin, easily susceptible to deep infection;
- absence of apical constriction: the funnel-shaped part smoothly passes into the growth zone;
- short root length;
- oval cross-sectional shape of the canal in the apical region.
When starting any manipulations with root canals, the pediatric dentist must first determine their anatomical structure and individual characteristics, using radiography and other modern research methods.
Tooth development.
The formation of the rudiments of baby teeth in the fetus begins at 4–5 months of intrauterine development. That is why the mother’s illnesses during this period lead to disruption of various stages of dental development, for example, a violation of the mineralization of the tooth occurs. As a result, the enamel can become weak and brittle. Taking certain medications during this period can also affect the development of teeth. For example, if the mother was treated with tetracycline antibiotics, the child’s teeth will be dark yellow or even brown (so-called tetracycline teeth).
Enamel mineralization begins in the prenatal period and continues for 6 months after birth. Mineralization of the crown part of the teeth has time to take place in utero, while mineralization of the cervical region of the incisors, canines and molars continues after birth, in completely new and not always favorable conditions. The mineralization process can be negatively affected by the nature and diet, social living conditions and various diseases of the child (acute respiratory infections, intestinal infections and functional diseases). That is why the cervical area is the most vulnerable and typical place for the occurrence of “bottle” caries of primary teeth.