The drug is used in radiation and combination therapy and has a non-hormonal, analgesic, and reparative spectrum of action. The unique composition allows it to be used for therapeutic and prophylactic purposes, for the treatment of wounds, trophic ulcers and anal fissures. The Russian medicine accelerates the restoration of the epidermis and mucous membrane after radiation exposure.
Features of the composition
The active ingredient of the drug is lidocaine hydrochloride, which is necessary for pain relief. Additional gel ingredients are presented:
- purified water;
- chlorhexidine hydrochloride;
- hydroxyethylcellulose.
Annotation from the manufacturer indicates that the drug has a nonspecific stimulating and antiradical spectrum of action. It helps to normalize the functioning of the immune system, accelerate recovery processes at the cellular level, stabilize the formation, development and maturation of blood cells.
The product applied to the skin inhibits nerve conduction by blocking endings and fibers. Lidocaine is superior in effectiveness to its closest analogue, procaine. During the treatment of oncological pathologies, the drug provides radioprotective effectiveness, reducing the susceptibility of healthy cellular structures and tissues to radiation therapy and its destructive properties.
Therapeutic manipulations make it possible to increase the volume of radiation dosages and reduce the intervals between sessions prescribed to patients with cancer.
Introduction
Laser methods for correcting age-related changes and treating various skin pathologies (vascular and pigment abnormalities, hypertrichosis, scar deformities, etc.) are in great demand and allow expanding the range of services in dermatology and cosmetology. Contrary to popular belief, most laser procedures involve pain. The increasing demand for effective and painless laser procedures has stimulated the search for the ideal anesthesia method. Patients expect quick but impressive results from procedures. To meet these needs, dermatologists are constantly searching for anesthetics that are effective, pose the least risk to the patient, and have minimal unwanted side effects.
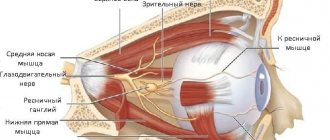
Innervation and sensory function of the skin. Skin pain. Brief information
Sensory receptors in the skin convert certain forms of energy into action potentials in sensory neurons. Cutaneous mechanoreceptors respond to touch and pressure. Thermoreceptors are involved in the sensation of heat and cold. Nociceptors are multimodal receptors and respond to stimuli such as pain (bite, pinch, cut, prick), extreme heat (burn) and cold, mediators of inflammation (Table 1).
Table 1. Basic sensory modalities of the skin Source: Kim E. Barrett, Susan M. Barman, Heddwen L. Brooks, Jason X.-J. Yuan. Ganong`s Review of Medical Physiology. 26th ed. McGraw-Hill Education; 2022.
Sensory axons originate in sensory ganglia and define areas of the skin called dermatomes. They are myelinated in the dermis but not in the epidermis. From a plexus in the deep dermis, nerve fibers rise to the surface of the skin and form a superficial nerve plexus at the junction of the reticular and papillary dermis. Nerve endings can be free, dilated or corpuscular. Impulses from nociceptors are transmitted through myelinated Aδ fibers (2-5 µm in diameter) at a speed of 12-35 m/s and unmyelinated C-fibers (0.4-1.2 µm in diameter), conducting impulses at a lower speed - 0.5- 2 m/s. Activation of Aδ fibers is responsible for the primary, so-called fast, pain, which is an immediate response to a stimulus and determines the site of action and the intensity of the painful stimulus. Activation of C-fibers is responsible for secondary pain (delayed or slow pain), which is characterized by vague, dull, diffuse, aching painful sensations [1].
Skin pain, mostly acute, occurs due to physical, chemical or thermal injury, but can also be chronic. Pain is not so common with skin diseases (mainly with ulcerative skin lesions, Lyell's syndrome), but nevertheless accompanies neurological or neurocutaneous diseases. External painful stimuli, as well as numerous chemicals such as bradykinin, histamine, serotonin, prostaglandins, interleukin-1, etc., are capable of modifying or inducing nociceptor activation. Substance P is the best known and most important pain mediator. Other pain mediators have also been described: CGRP, somatostatin, glutamate, etc. [2].
The main “nociceptive triggers” in cosmetology are all injection techniques (mesotherapy, contouring, biorevitalization, PRP therapy, thread technologies, etc.), laser and IPL procedures, RF microneedling lifting, dermabrasion, chemical peels. In fact, any of the listed procedures has a pronounced stimulating effect on all types of nociceptors - chemical, mechanical and thermal [3].
High-energy laser effects on the skin can cause acute pain. The somatosensory system reacts instantly to the transduction of a nociceptive signal due to intense, transcendental stimulation of multimodal nociceptors, primarily thermal nociceptors.
Pharmacology of local anesthetics
Local anesthetics are divided into 2 groups: those containing an ester linkage (for example, procaine (procaine), tetracaine, cocaine) and those containing an amide linkage (for example, lidocaine and prilocaine) (Fig. 1).
Rice. 1. Scheme of the structure of ether and amide anesthetics. (J. Morgan. Clinical anesthesiology. Book 1. M., St. Petersburg: Binom; 2001).
Ester local anesthetics are metabolized by plasma cholinesterase and other nonspecific esterases, while amide anesthetics are primarily metabolized in the liver via microsomal enzymes. It is known that ester anesthetics can cause allergic reactions upon contact with the skin, while this is rare with amide anesthetics. Para-aminobenzoic acid is a metabolite of ester hydrolysis and is associated with allergic reactions. The solubility of local anesthetics in fats correlates with their strength and duration of action (Table 2)
Table 2. Structure and properties of local anesthetics1 Note. Adapted from Strichartz GR, et al. Fundamental properties of local anesthetics. II. Measured octanol: buffer partition coefficients and pKa values of clinically used drugs. Anesth Anal. Aug 1990;71(2):158−170. [4].
Mechanism of action of local anesthetics
Local anesthetics reversibly block nerve conduction near their injection site by acting on free nerve endings in the dermis or mucosa, resulting in temporary loss of sensation in a localized area. Conduction of nerve impulses is blocked by a decrease in the permeability of nerve cell membranes to sodium ions, possibly due to competition with calcium-binding sites that control permeability to sodium ions (Fig. 2).
Rice. 2. Mechanism of action of local anesthetics (adapted from K. Whalen, C. Feild, R. Radhakrishnan. Lippincott Illustrated Reviews: Pharmacology. 7th ed. Wolters Kluwer; 2019).
Rice. 3. Recommendations for the use of topical anesthesia during laser ablation procedures.
Rice. 4. Recommendations for the use of topical anesthesia during non-ablative laser procedures without violating the integrity of the skin.
Complete inhibition of conduction is achieved by increasing the concentration of anesthetic.
Clinical and pharmacological properties of a combined local anesthetic cream containing 2.5% lidocaine and 2.5% prilocaine (eutectic mixture)
Eutectic mixtures
are compounds that melt at lower temperatures than any of their components, allowing the use of higher concentrations of anesthetics. It is a 5% oil-in-water emulsion with a melting point of 18°C, consisting of 25 mg/ml lidocaine, 25 mg/ml prilocaine, thickener, emulsifier and distilled water adjusted to pH 9.4. Since the eutectic mixture is a liquid, anesthetics do not need to be dissolved in oil before being introduced into the aqueous phase of the formulation; this increases the concentration of the active substance in the emulsion droplets and allows more of the anesthetic to penetrate the nerve endings in the deeper layers of the skin. Lidocaine/prilocaine cream is applied in a thick layer (1-2 g per 10 cm2, maximum dose - 60 g per 600 cm2) to intact skin under an occlusive film (cling film can be used) to facilitate the penetration of local anesthetics through the stratum corneum. The depth of anesthesia depends on the time of contact with the cream. It has been shown that the anesthetic effect reaches a depth of 3 mm after 60 minutes, 4 mm after 90 minutes, and 5 mm after 120 minutes of use [5]. Cutaneous analgesia increases within 3 hours with an occlusive dressing and persists for 1-2 hours after removal of the cream. After application of lidocaine/prilocaine cream to the skin, a biphasic response occurs with initial vasoconstriction and blanching of the skin (peaking after 90 minutes of application). After 2-3 hours of application, vasodilation occurs, which leads to skin erythema. It should not be confused with other adverse skin reactions such as urticaria or allergic contact dermatitis. The amount of systemic absorption of the cream is directly related to the duration and area of application. Blood flow and skin thickness, the presence of a particular skin pathology affect the absorption, onset of action, effectiveness and duration of action of lidocaine/prilocaine cream.
The stratum corneum of the epidermis is the main barrier to the delivery of local anesthetic deep into the skin. There are 3 ways of penetration through the stratum corneum: intercellular (through the intercellular spaces of keratinized keratinocytes), para- or transcellular (through keratinized cells), through the infundibulum (follicular part) of the hair follicle and the ducts of the sweat glands. Local anesthetics penetrate more easily through the mucous membrane of the oral cavity, genitals and conjunctiva due to the absence of the stratum corneum [6].
Factors influencing the delivery of local anesthetics to the skin:
1) dosage form - free bases are lipophilic and can independently penetrate the stratum corneum, while salt forms require special delivery systems for this;
2) melting point and eutectic mixtures - the lower the melting point, the better the penetration. Eutectic mixtures have a lower melting point, thus providing better penetration than the individual component;
3) the concentration of the drug in the vehicle - the higher it is, the faster the penetration rate.
Despite the low risk of systemic toxicity, clinicians should be wary of potential side effects. Using lidocaine/prilocaine cream on broken or inflamed skin or over a large area (greater than 600 cm2) may increase the risk of systemic side effects. Prilocaine as part of a combination cream may cause methemoglobinemia due to its ability to oxidize iron in red blood cells to a ferric state, impairing oxygen transport. Lidocaine/Prilocaine Cream should not be used in patients with congenital or idiopathic methemoglobinemia or in children younger than 12 months who are taking medications known to cause methemoglobinemia such as sulfonamides, dapsone, acetaminophen, nitrates, nitrites, and phenobarbital.
Lidocaine/Prilocaine Cream is classified as Pregnancy Category B, but caution should be exercised when used in nursing mothers as lidocaine and possibly prilocaine are excreted in breast milk in small amounts. The risk of side effects in infants is considered minimal.
Danger of using ether and highly concentrated anesthetics
The US Food and Drug Administration (FDA) has issued an advisory regarding the risk of dangerous side effects associated with the use of local anesthetics for cosmetic procedures. It states that local anesthetics are sometimes used in unapproved ways and in doses that may pose a serious risk to the health and life of the patient. There have been 2 reported deaths associated with the application of topical anesthetics to the legs for pain relief during laser hair removal. Patients, at the direction of specialists, wrapped their legs in cellophane to enhance anesthesia. Both patients experienced convulsions, coma, and subsequent death due to the toxic effects of anesthetics. As it turned out, in these cases, creams with a high concentration and excessive amounts of lidocaine and tetracaine were used (gel 10% lidocaine + 10% prilocaine in the first case and gel 6% lidocaine + 6% tetracaine in the other) [7].
Therefore, in 2006, the FDA issued an official warning about the potential for side effects caused by drugs containing a mixture of ester and amide local anesthetics. Active ingredients of products not recommended by the FDA as topical anesthetics: benzocaine 20% + tetracaine 4% + lidocaine 6%; lidocaine 10% + tetracaine 10%; lidocaine 30% + prilocaine 2% + tetracaine 4%; lidocaine 15% + prilocaine 5%; lidocaine + prilocaine + tetracaine.
Use of lidocaine/prilocaine cream during laser procedures in dermatology
The use of lidocaine/prilocaine cream significantly expands the possibilities of outpatient dermatological procedures. Topical anesthesia significantly reduces pain discomfort during skin biopsy (shave and punch biopsy), curettage, laser and electrosurgical removal of molluscum contagiosum and warts, laser treatment of port-wine stains and removal of blood vessels on the legs, laser sanitation of trophic ulcers, etc. [7-11 ]. Topical anesthesia is also used on the genital mucosa in adults for painless removal of local lesions, such as genital warts [12].
The main indications for laser procedures in dermatology and the application time of lidocaine/prilocaine cream are shown in table. 3.
Table 3. Indications and times of application of lidocaine/prilocaine cream for common laser procedures in dermatology
Use of lidocaine/prilocaine cream during laser aesthetic procedures
All types of laser interventions in dermatology can be divided into 2 types:
1) procedures during which ablation (layer-by-layer removal) of the affected skin area is performed;
2) procedures aimed at selective removal of pathological structures without compromising the integrity of the skin (the principle of selective photothermolysis).
In the first case, lasers operating in the mid- and far-infrared spectrum are used for ablation: Er: YAG (2940 nm) and CO2 (10,600 nm). The chromophore is water. Various modes of exposure to the skin are used - incision and excision, continuous and fractional ablation. The level of pain during ablative procedures depends on the energy parameters of the impact, which determine the depth of the impact, the percentage of coverage (the greater the distance between the microthermal ablation areas, the more comfortable the procedure), the area of treatment (the most sensitive: the periorbital region, nasolabial triangle, centrofacial region). Before the advent of topical anesthetics, ablative laser procedures required the use of intravenous sedation. With the introduction of more superficial single-pass and fractional techniques, it is possible to provide adequate anesthesia using topical anesthetics [13]. The market leader in topical anesthesia is the eutectic mixture of lidocaine and prilocaine. For almost all ablative procedures, the recommended minimum application time for lidocaine/prilocaine cream is 60 minutes. This time is sufficient to treat the skin to the level of the basement membrane, when it is necessary to carry out continuous or fractional superficial ablation without removing the laser-induced eschar. In cases where it is necessary to remove the scab with subsequent repeated passage in this area, the anesthesia time should be increased to 90-120 minutes, and the possibility of conduction anesthesia should also be provided.
A prerequisite before starting the procedure is to completely remove the cream and dry the skin so that the laser light can interact unhindered with the tissues.
To carry out deep laser multi-pass resurfacing, additional methods of pain relief are required - intravenous sedation, conduction anesthesia, anesthesia. Although there are many options for local anesthesia for laser resurfacing, unfortunately, there is no standard guidance to ensure optimal safety when using local anesthetics. When deciding which one to use, several factors must be considered: the anatomical site, the amount of anesthetic used, the duration required for the desired depth of anesthesia, the safety profile of the individual local anesthetic and how it interacts with the patient's comorbidities [14].
Type 2 laser procedures do not violate the integrity of the epidermis, but may also be accompanied by significant discomfort associated with painful sensations.
Laser fractional photothermolysis is used for non-ablative rejuvenation of mild to moderate skin photodamage, wrinkles and dyspigmentation. The popularity of this procedure is due to its high clinical effectiveness and moderate side effects - transient erythema and edema. However, deep penetration of laser light in the near-infrared spectrum creates the effect of volumetric thermal heating in the deep layers of the skin, producing a pronounced pain effect due to the high density of polymodal nociceptors and thermoreceptors in the dermis. To increase the comfort of the procedure, a combination of topical anesthesia with lidocaine/prilocaine cream (application 45-60 minutes) and cooling of the treatment area with a forced stream of cold air is recommended [15-17].
Laser hair removal is the most common procedure that uses topical anesthetics, especially in sensitive areas such as the upper lip and groin area. For effective pain relief in these areas, the application time of lidocaine/prilocaine cream under the occlusive film should be at least 30 minutes if the skin is prepared for hair removal (hair shaving) immediately before the procedure. Due to the deep penetration of laser light (up to 4 mm for epilation with a neodymium laser), the time of application of the cream on skin prepared in advance for the procedure (hair shaving 1 day before) should be 45-60 minutes. To prevent delayed side effects after laser hair removal (thermal injury, paradoxical hypertrichosis), it is recommended to apply a cooling pack to the laser-treated skin area for 30 s during the procedure [18, 19].
Treatment of vascular pathology of the skin in most cases does not require anesthesia. Especially when it comes to the removal of single telangiectasias or small vascular malformations (cherry and spider angioma, pyogenic granuloma, venous lake, etc.). However, during laser removal of port-wine stains in the facial area, especially in children and adolescents, severe pain is observed that requires adequate anesthesia. Lidocaine/prilocaine cream with an exposure of 20-40 minutes is effective as an anesthetic, depending on the area of the port-wine stain and its location - the closer to the center of the face, the more painful the procedure [10]. Although the skin may appear pale due to the vasoconstrictor effect of the local anesthetics contained in the cream, treatments using a pulsed dye laser or IPL device provide satisfactory treatment results for port-wine stains. Restoring blood flow to pale areas can be achieved by rubbing or blowing a stream of warm air onto the skin surface (hair dryer). At the same time, the effectiveness of anesthesia is not reduced. Additionally, to improve the comfort of the procedure, it is recommended to apply cooling packs to the treated area.
Anesthesia for laser treatment of pigmented skin pathology and tattoo removal is carried out according to the same scheme.
Before the laser procedure, in each case of using local topical anesthesia, it is strongly recommended to carefully remove the cream using an antiseptic water-based solution and dry the skin. This will facilitate unhindered interaction of laser light with the surface of the skin. It should be remembered that the anesthetic cream is an oil-in-water emulsion containing excipients that practically do not penetrate the skin - polyethylene glycol-54, hydrogenated castor oil. As a result, a film may remain on the surface of the skin after the absorption of anesthetics, which, when interacting with laser light, absorbs a certain part of the energy, thereby causing a burn to the epidermis and/or reducing the effectiveness of laser exposure.
Indications and contraindications
The drug is prescribed after radiation therapy in order to accelerate the regeneration of damaged cells. Coletex gel can also be used for other injuries:
- for abrasions, wounds, scratches;
- diabetic and trophic ulcers;
- vaginal injuries;
- anal fissures;
- punctures in the sinuses;
- suturing – after treatment of epidermal abscesses that have arisen;
- eruption of baby teeth;
- insertion of a probe through the nasal passages or oral cavity;
- performing rectoscopy manipulations.
The medication is suitable for performing resection of polyps located in the nasal cavity and simple operations related to the treatment of the organs of vision.
The main contraindications to the use of the gel include individual intolerance to individual components. In addition to hypersensitivity to the ingredients, special caution is required when using the medicine in people with persistently low blood pressure (hypotension) or sinoatrial block (impaired conduction of impulses to the ventricles and atria).
Constant medical monitoring of therapy is required for patients with a slow heartbeat, chronic and acute heart failure, and intraventricular conduction abnormalities.
How to make teething easier for children.
December 15, 2022
2370
5
2
Content
- Symptoms of teething in children
- Top 7 pain-relieving gels for teething
- Kamistad Baby
- Dentinale
- Holisal
- Baby Doctor First teeth
- Kalgel
- Pansoral
- Dentinox
A baby’s first teeth are always a great joy for parents, but often this is accompanied by a deterioration in the child’s well-being, fever, moodiness and bad mood. Only 30% of young children do not have any negative symptoms when teething. In pharmacies you can buy various drugs to improve the condition of a child during teething: both drugs for oral administration and for external use. Today we’ll talk about gels for gums.
Many parents buy such products on the advice of friends or based on reviews from moms on forums. But it is better to consult a pediatrician before purchasing a painkiller, because only a doctor can take into account all the individual characteristics of your baby’s body and choose a truly effective and safe remedy.
Read also Top 10 best hypoallergenic formulas for children 10 best infant formulas for children with allergies.
Features of application
The gel is evenly applied to the affected areas - mucous membrane or skin in small quantities. The drug can be administered into the vaginal and rectal areas; if indicated, the drug can be used as a basis for therapeutic dressings.
The dosage is determined by the attending physician based on the results of a laboratory diagnostic examination, after determining the stage and severity of the disease. Over the course of 24 hours, manipulations are repeated no more than 4 times.
The drug is not recommended for use by pregnant and lactating women and, for minors under 18 years of age, the drug is prescribed with extreme caution and regular checks of general condition.
Pharmacokinetics
Absorption: When applied topically to mucous membranes, lidocaine is absorbed to varying degrees, depending on the dose and site of application. The rate of perfusion in the mucosa influences absorption.
Distribution: lidocaine is distributed in well-perfused organs, incl. in the kidneys, lungs, liver, heart, and also penetrates into adipose tissue. Penetrates the placenta by passive diffusion. Distribution in the placenta may be sufficient to penetrate the fetus and reach toxic levels. Lidocaine quickly crosses the placenta, appearing in the fetal bloodstream within a few minutes of maternal use.
The binding of lidocaine to plasma proteins is largely dependent on the concentration of the drug and alpha-1-acid glycoprotein (AAG) in plasma. There are reports of lidocaine binding to proteins by 60-80%. This indicates that plasma protein binding is increased in uremic patients and renal transplant recipients and is enhanced after acute myocardial infarction. The latter is also characterized by an increase in the level of AAG. Increased protein binding may reduce the effect of free lidocaine or even cause an overall increase in drug plasma concentrations.
Metabolism: lidocaine is metabolized with the participation of microsomal liver enzymes, a decrease in alkalinity due to oxidation occurs within a few minutes. Metabolic rate is limited by hepatic blood flow and, as a result, may be impaired in patients following myocardial infarction and/or with congestive heart failure. As a result of the biotransformation of lidocaine, metabolites are formed - monoethylglycine exilidide (MEGCS) and glycine exilidide, which have significantly less pronounced antiarrhythmic activity.
Excretion: about 90% is excreted in the form of metabolites and 10% unchanged by the kidneys. Excretion of unchanged drug in urine depends in part on urine pH. Acidic urine has been reported to increase the proportion excreted in urine. The half-life (T1/2) of lidocaine is longer in patients with liver disease.
Indications for use
Lidocaine, 5% ointment is used for local anesthesia of the skin and mucous membranes of the oral cavity and perianal area
Directions for use and doses
The dose depends on the indications, the area of the anesthetized surface, the vascularity of the tissue and the individual tolerance of the patient. Use the minimum dose to achieve the desired effect. Do not use the drug for a long time
Adults and children over 12 years of age
To relieve pain - apply 1-2 g as needed
Children (up to 12 years old)
In children under 12 years of age, 100% bioavailability should be taken into account after application to mucous membranes and damaged skin, and therefore the maximum amount of Lidocaine, 5% ointment prescribed to children should not exceed 0.1 g of ointment/kg body weight (corresponding to 5 mg lidocaine/ kg body weight). The minimum interval between doses in children should be 8 hours.
Side effect
Hypersensitivity reaction in the form of skin irritation (the drug contains propylene glycol), urticaria, swelling, and in severe cases anaphylactic shock may develop.
Systemic toxicity from local anesthetics mainly includes CNS and cardiovascular side effects.
From the side of the central nervous system - restlessness, anxiety, agitation, nervousness, disorientation, confusion, paresthesia, dizziness, tinnitus, miosis, blurred vision, nausea and vomiting, convulsive contractions and muscle tremors. Insensitivity of the tongue and in the area around the mouth, absent-mindedness, irritation, depression and drowsiness, respiratory failure and coma.
From the cardiovascular system: myocardial depression, peripheral vasodilation as a result of hypertension and bradycardia; arrhythmias and cardiac arrest.
Rarely: methemoglobinemia is possible.
Pansoral
This is a French phytogel for children's gums, the quality and safety of which are confirmed by international certificates. "Pansoral" relieves inflammation and slightly numbs the baby's gums. Thanks to the rapid penetration of active substances into the mucous membrane, the pain subsides in just two minutes. The preparation contains chamomile and saffron flowers, an extract from marshmallow roots. These components are excellent antiseptics; they heal and disinfect well. Gel "Pansoral" can be used in children from 3 months of age, it is completely natural. The drug is also indicated for the healing of ulcers on the mucous membrane, stomatitis, and bacterial rashes in the oral cavity. It is advisable to consult a pediatrician before using the drug. Among the disadvantages of the product is that it is not available in all pharmacies, it can cause an allergic reaction.
Pansoral
Pierre Fabre Medicament, France
Pansoral is a natural herbal remedy that is used to ease teething in children.
The plant extracts included in the preparation have a calming and softening effect on the gum mucosa. The plant extracts included in the preparation have a calming and softening effect on the mucous membrane of the gums and help the child endure this period easier. from 280
416
- Like
- Write a review