A person can lose all or a large number of teeth for various reasons: due to injuries, poor quality treatment, lack of attention to hygiene and dental health. Of course, such a problem as a completely toothless jaw requires an urgent solution, and not only because without teeth a person feels insecure and is embarrassed to communicate with other people.
Missing teeth negatively affects the health of the body as a whole and can lead to:
- To premature aging of the face. In the absence of teeth, facial wrinkles appear much earlier than time;
- To violations of diction;
- To the development of chronic diseases of the gastrointestinal tract. When a person is missing all teeth or a significant number of elements of the dentition, food is not chewed correctly and this leads to disruptions in the processes of digestion and metabolism.
To restore your teeth, you need to go to dentistry, and if you have a completely toothless jaw, you may be offered removable dentures or dental implantation using the All-on-4 protocol as an option for restoring lost dental units.
YOU NEED TO REMEMBER! Removable dentures will allow you to restore teeth inexpensively, but removable dentures cannot be called convenient and comfortable in everyday use. They can rub the soft tissues of the mouth, fall out during eating, active conversation, and cause diction problems. After implantation of all-on-4, a fixed prosthesis is placed on the implants, which is free of all the disadvantages of removable orthopedic structures.
What is All-on-4 implantation, when is this method of dental restoration used, what features will the treatment have? We will answer these questions about All-on-4 implantation in our article. Also in the material you can find up-to-date information on prices for All-on-4 dental implantation in Moscow.
Take a short test and calculate the cost of treatment!
Take a short test
All-on-4 implantation - technology features
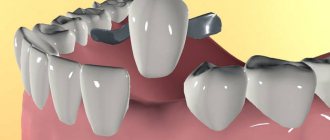
This is a technology for restoring dentition using an accelerated method for those who have lost their teeth completely or are missing a significant part of them. On the day of treatment (if there are no specific contraindications), 4 implants are implanted into the jaw within 1.5-2 hours. Two of them are located vertically in front, the rest are located on the side at an angle of 45⁰. The inclined position ensures reliable fixation of the prosthesis in the oral cavity, since the area of contact of the titanium pin with the bone tissue increases.
After installing the implants with abutments, a temporary acrylic prosthesis is attached to them. Its service life usually ranges from 3 months to six months - it is during this time that artificial roots take root. The reinforced metal-plastic adaptation structure can be used for up to 3-4 years. A permanent bridge is made of zirconia, ceramic or ceramic composite. The latter option is characterized by increased strength and durability - its service life reaches 20 years.
What is the difference between a prosthesis on 4 implants and classical methods of dental prosthetics? This technique has several obvious advantages:
- speed of treatment - you can install a prosthesis in one visit to the dentist, spending only a few hours;
- high survival rate - in 99% of cases titanium pins are not rejected (the most effective result in comparison with other types of prosthetics);
- comfort - adaptation to the design occurs quickly, in just 1-2 days, during the process of adaptation, diction is not impaired, and the mucous membranes of the oral cavity are not injured;
- minimum contraindications and restrictions - the technology allows you to restore the dentition of people who have lost all their teeth, including people over 80 years old, patients with bone tissue dystrophy, and periodontal diseases;
- aesthetics - an artificial jaw does not differ in appearance from a real one, it looks natural and attractive;
- safety and atraumaticity - soft tissues and bones are not injured during implantation, and preliminary maxillofacial surgeries and osteoplasty are also not required.
How does “All on 4” dental implantation work?
After the examination, the dentist makes a diagnosis and proposes a treatment plan. If the patient agrees to prosthetics, a day of surgery is scheduled. Preparation for it does not imply special events. General tests are performed.
The operation is performed under anesthesia. Teeth that interfere with the installation of a prosthesis on four implants are removed. Implants are implanted, which will subsequently become the basis of the structure. A temporary prosthesis is attached to them. This is a permanent acrylic plate. It follows the outline of the dentition.
Some time after the end of the operation, the patient can chew food and smile. The temporary structure looks great. It is installed until the tissues have completely healed. After this, the doctor makes an impression of the jaw to make a permanent denture. It is installed 4-6 months after surgery.
Who is All-on-4 technology suitable for?
All-on-4 implantation is the optimal way to restore both the upper and lower dentition in cases of complete edentia or the absence of a significant number of teeth. Fixed dentures, unlike removable dentures, look more natural, last much longer, do not impede diction and eating, and are securely fixed in the oral cavity.
This technology is also suitable for people who value their time. Classic implantation requires regular visits to the dentist for six months or more. In this case, visible results are achieved only at the end of treatment. A prosthesis on 4 implants is installed in just a few hours without pain or discomfort.
Dental prosthetics using the all on 4 method is indispensable when there is insufficient bone tissue. After tooth extraction, the jaw atrophies in just 2-3 months, and the installation of a classic implant requires osteoplasty - bone augmentation. This operation is not necessary when installing an “All-on-4” prosthesis. In addition, the fixed design is an excellent alternative to a removable denture if it needs to be replaced.
The benefits of this method will also be appreciated by people with periodontal diseases. In case of inflammation of the periodontal tissues, or the presence of loose or untreatable teeth, only the technology under consideration can restore the dentition completely.
All-on-4 implantation is suitable for the absence of most teeth and complete edentia
Are there any disadvantages to All-on-4 that you should know about before starting treatment?
Every dental implant technology has certain disadvantages and All-on-4 is no exception in this regard. The main disadvantages of “all on four” implantation include a wide range of contraindications and high requirements for the height and volume of jaw bone tissue.
The problem of bone deficiency can be solved by installing zygomatic implants, but so far they are produced only by the Nobel brand, which supplies the market with expensive premium implant systems. The use of Nobel zygomatic implants will significantly increase the price of All-on-4 implantation.
YOU NEED TO REMEMBER! All-on-four implantation requires careful planning, as well as high skill of the implantologist. The slightest mistakes when implanting implants can lead to their rejection, so when choosing a clinic in Moscow for All-on-4, always find out all the details regarding the level of equipment of dentistry and the competence of the specialists working in it. In our dental clinic in Moscow - “Firadent”, dental implantation is carried out by competent specialists who regularly improve the level of their knowledge and practical skills abroad - in the USA and Europe.
Take a short test and calculate the cost of treatment!
Take a short test
Contraindications
Relative contraindications to all on 4 implantation are inflammatory diseases of the oral mucosa and caries. After sanitation, implants can be installed.
It is strictly forbidden to do prosthetics using this method if the patient is diagnosed with:
- oncological processes in the body;
- blood diseases;
- inflammation in the acute phase of any localization;
- diabetes;
- drug addiction;
- tuberculosis;
- exacerbation of mental pathology.
Who is not suitable for all-on-4 (all-on-4) implantation?
Implantation all on 4x (all on four) has not only indications, but also contraindications for implementation. These include: chronic kidney and liver diseases, severe heart pathologies, blood clotting problems, autoimmune diseases, tuberculosis and diabetes.
As we noted above, All-on-4 implantation requires a fairly good condition of the bone tissue, and if the diagnosis reveals a moderate or severe form of jaw bone atrophy, then it is better to choose an alternative implantation technique - All-on-6. It uses a larger number of implants, so even with severe atrophy of the jaw bone tissue, it is possible to achieve strong fixation of artificial roots and dentures.
Advantages and disadvantages of All-on-4 implantation
Before deciding to install implants, it is necessary to analyze all the advantages and disadvantages of the technique. The advantages of the technology include:
- there is no need to carry out preliminary maxillofacial operations or build up bone tissue;
- installation of implants and prosthesis is carried out within 1 day, even immediately after tooth extraction (pins can be fixed both in the hole and nearby);
- all manipulations are low-traumatic and are performed under anesthesia, so no discomfort or pain is felt either during the procedure or after it;
- the placement of the side implants at an angle ensures reliable fixation of the prosthesis and uniform distribution of the load on the jaw;
- all on 4 implantation is the prevention of bone tissue atrophy (unlike removable structures);
- from an aesthetic point of view, “all-on-4” dentures are better than many analogues - they look as natural as possible and improve diction;
- accessibility – in case of severe or complete edentia, restoring the dentition using this method will cost many times less than classical two-stage implantation.
There are also disadvantages, but they are much fewer. The list includes allergic reactions to the material from which the prosthesis is made (rare), the presence of absolute contraindications.
The possibility of implant failure cannot be ruled out. However, it should be remembered that when contacting experienced specialists (and these are the ones who work in our clinic), this risk is less than 1%.
Dentures look aesthetically pleasing and are practically indistinguishable from real teeth
Long-term results of basal implantation. Clinical experience.
Author: implantologist-surgeon Sheleg V.L.
This article is the result of many years of accumulated experience in installing basal implants. The article will help patients planning complex dental restoration using immediate loading methods to make the right choice and forget about dental problems for a long time.
Basal implantation
In Belarus, basal implantation began to gain popularity in 2010-2011, after the registration of products from the Swiss brand Ihde Dental AG. The starting point of the era of basal (or one-stage, single-stage, single-phase, express) implantation can be considered the arrival of the company’s founder, Dr. Stephen Ihde, to conduct a demonstration operation at one of the private clinics in Minsk.
I had the opportunity to assist Dr. Ide during an operation that involved multiple tooth extractions and the placement of 18 basal compression implants. Having gained invaluable experience, we, together with our colleagues, orthopedists and dental technicians, have successfully introduced basal implantation into our practice. Over the course of 3 years, we completed several hundred complex works of varying degrees of complexity, with different numbers of implants, different positioning, different prostheses, etc.
Today, after 10 years of observing patients after basal implantation in different clinics, I have the opportunity from my own experience to compare the effectiveness of the technique with other similar implantation techniques with immediate loading.
Short and long term results
Results can be divided into short-term (0-24 months) and long-term (24-100 months). In the first 2 years, the quality of installation of basal implants is of key importance, namely:
• correct positioning, • parallelism, • density of fixation, • fixation into the cortical bone, • and much more, which makes up a high-quality implantation .
Positive short-term results are quite easy to achieve. It is enough for a surgeon to learn a little from experienced colleagues, perform 10-20 operations and evaluate all the technical nuances with his own hands. Negative aspects in short-term results are possible 1) due to gross mistakes by the surgeon due to lack of experience (rarely); 2) due to the individual characteristics of the patient (rarely).
As for long-term results, the picture is somewhat different. The results of basal implants are significantly inferior to classical implants installed and replaced using an immediate loading protocol.
Let's look at several cases and identify several key problems that are highly likely to await the patient after 24 months after basal implantation.
Basal implantation. Case No. 1
December 2014: complex implantation of the upper and lower jaw with basal implants with immediate loading was performed. A temporary reinforced acrylic prosthesis was installed and fixed with temporary cement.
March 2016: a patient from the Russian Federation contacted the KANO clinic with complaints of a broken upper prosthesis.
The patient wrote by e-mail: “I would like to ask you for help in solving the problem. At my place of residence, I was denied warranty service due to the statute of limitations. I am sending you a picture after the destruction of the upper prosthesis. The image shows that the last right and left implants on the upper jaw (in positions No. 18 and No. 28) remained in the body of the bone. You can also see implants that have become loose.”
Comment: in this case, the patient did not perform the prosthesis replacement recommended to him at his place of residence 12-14 months after implantation. Also, according to the patient, he did not correct the prosthesis. As a result, he began to “overload” the right side. The basal implant, installed in the area of the right tubercle of the upper jaw at an angle, could not withstand the load and broke at the bend. The load shifted to the left side and within a week a similar situation occurred on the left side.
Solution: classic implantation protocol in the upper right and left segments. Removal of problematic implants, bone augmentation (open sinus lift) + simultaneous implantation of 3 classic implants + installation of 3 implants in the right side. After 6 months prosthetics of implants with metal ceramics (permanent prosthesis).
Basal implantation. Case No. 2
March 2014: comprehensive implantation of the upper jaw with basal implants was carried out, 3 basal implants were installed on the left and right sides of the lower jaw. February 2015: metal-acrylic prostheses were replaced with metal-ceramic ones. Testing of the implants showed 100% stability (according to the patient).
December 2022: Contacted the KANO clinic. Complaints about the mobility of the upper prosthesis. An inspection has been scheduled. Micromobility of the prosthesis was revealed. Observation 2 weeks. Mobility has increased significantly. The decision was made to remove the prosthesis. Lack of stability was revealed in 3 implants in the area of teeth 22, 23, 24.
A treatment plan has been drawn up. The implants were removed + 3 basal implants were installed, temporary prosthetics were performed using a metal-acrylic prosthesis with fixation using temporary cement.
July 2022: a complaint was received about the mobility of the upper prosthesis. The examination revealed mobility of the implants in the cusp areas in the area of teeth No. 18, 28.
Together with the patient, it was decided to remove all basal implants and carry out work according to the immediate loading protocol on classic implants with multi-unit abutments - ALL-ON-6 (all on six implants). The work was completed according to the agreed plan. A temporary prosthesis with screw fixation was installed (without restrictions on food intake). Detailed care instructions are provided + an irrigator as a gift (promotion from the equipment supplier!).
July 2022: Follow-up inspection. Removal of the prosthesis. Lack of implant mobility. No complaints.
Basal implantation. Case No. 3
September 2016: total rehabilitation of the upper jaw was performed using one-stage basal implants, without gum incision. 9 implants were installed, 2 of which were in the tuberosities of the maxillary bone.
November 2022: the patient contacted the KANO clinic for advice regarding the mobility of the prosthesis. At the site of implantation, the patient did not receive any practical proposals to correct the situation. After carefully removing the upper jaw prosthesis, the implant on the right side was broken and was partially removed along with the prosthesis.
Why did it break? Before installing basal implants, surgeons often bend them (by hand or with pliers) to achieve parallelism with other implants. In 90% of cases, such manipulation is performed “by eye”.
This slightly barbaric method is required due to the fact that basal implants are single-component, because... the implant and abutment are one. Unlike classic implants, in which an abutment can be selected separately for each implant.
As the structure is used and chewed continuously, a microcrack gradually appears in the bending area, which ultimately leads to implant failure.
Why is All-On-4/6 better in the context of such breakdowns?
All-On-4/6 operations, classic, two-piece implants are used. Consisting of the implant itself and the abutment. The bottom line is that for techniques with immediate loading, special angular abutments (multi-unit abutments) have been developed.
Thus, if the surgeon needs to install the implant at an angle, he does not need to bend the structure with his own hands. After installing the implant at an angle, a multiunit abutment with the appropriate angle of inclination is screwed to it.
November 2022: additional classical implants were installed in the area of teeth 17.27. The part of the basal implant remaining in the bone in area No. 18 was removed. A temporary prosthesis was made.
April 2022: after 5 months, a follow-up examination showed complete integration of the classical implants. Combined metal-ceramic prosthetics was performed.
Patient complaint: mobility of the lower left bridge.
Solution: CT and OPTG revealed no problems. The prosthesis was carefully removed. Mobility of 2 out of 4 basal implants was revealed. During extraction, one of the implants broke. 1 classic implant installed. After integration, after 3 months, it was decided to carry out combined prosthetics on basal and classic implants (due to the patient’s financial capabilities).
What implants and prostheses are used?
The “all on 4 implants” prosthetic technology was developed and introduced into global dental practice by the American company Nobel Biocare. Since then, the components of this brand have been considered the standard of quality. However, over the twenty-year period of use of the technique, many worthy analogues have appeared, produced by domestic and foreign enterprises.
Implants
The YuliSTOM dental clinic in St. Petersburg offers a wide range of titanium pins and abutments from different manufacturers for installation. The patient can choose the most suitable option in terms of quality and cost from the following brands:
- Rusimplant are universal orthopedic elements of the ConeFit system, produced in Russia using German technologies. Made of Grade 5 (titanium) alloy, corrosion resistant, highly compatible with biological tissues, lightweight and durable.
- Superline is a Korean middle-class prosthetic system made of Grade 4 alloy with a conical connection type.
- Nobel is the standard of all on 4 implantation components from the technology developer. Design features - different types of threads, a special microporous Ti-Unite surface, ensuring almost 100% engraftment, Grade 4 alloy (ultra-pure titanium).
- Straumann - are distinguished by a unique Roxolid alloy (titanium with zirconium dioxide) and a hydrophilic surface. These features of Swiss pins reduce the time of osseointegration to one and a half months.
- Prodigy is a product of BioHorizons Implant Systems, Inc., USA. They take root well due to the unique Laser-Lok surface and microchannels located on the neck of the titanium root.
- Adin Implant - implants made in Israel, characterized by a relatively low survival rate and outdated design. Made from Grade 5 titanium alloy with aluminum and vanadium.
- Hi-Tec Implant - in terms of properties and design, the products of the Israeli brand are as close as possible to the original Nobel implants. This explains the rather high rates of osseointegration.
The table contains brief basic information about each type of implant:
| Name | Class | Survival rate, % | Guarantee | Price, rub |
| Nobel | premium | 99,3 | for life | 198 000 |
| Superline | average | 98,2 | 120 000 | |
| Straumann | premium | 99,7 | 200 000 | |
| Adin Implant | average | 85 | 90 000 | |
| Hi-Tec Implant | average | 92 | 110 000 | |
| Prodigy | average | 97,5 | 115 000 | |
| Rusimplant | economy | 85 | 15 years | 50 000 |
Prostheses
After selecting the appropriate type of titanium roots, it is necessary to select fixed prostheses on 4 implants, as well as an adaptive (temporary) design. Manufacturers offer four main types of artificial teeth. The best option is metal-ceramic products from the Nobel company, the best acrylic bases are produced by the German brand Heraeus Kulzer, and crowns are produced by the Japanese company Yamahachi.
- Metal-free base with acrylic or zirconium dioxide crowns. The base of the artificial jaw is made of zirconium dioxide, which allows you to evenly distribute the load on the gums and give additional strength to the bridge. However, to reduce the cost of construction, a fiberglass frame lined with ceramics can be used. The product is quite durable - its service life is about 10 years.
- Metal-free crowns made of zirconium dioxide or acrylic. In the first case, the design is more durable and looks as aesthetically pleasing and natural as possible. Artificial teeth made of acrylic are cheaper, but they look less natural and wear out faster (their service life is limited to 5 years).
- Metal ceramics. A metal-ceramic prosthesis with a titanium beam is an expensive option characterized by increased strength. It is indispensable in the case of elongated side consoles of the structure. Among the disadvantages, one can note reduced aesthetics, since the titanium frame gives the ceramic a grayish tint. The cheaper option is not a titanium alloy, but a cobalt-chromium alloy (CHC), but it will weigh more.
- Milled titanium base with acrylic prosthesis. Beam prosthesis on 4 implants, with a hot polymerization plastic base from the German manufacturer Heraeus Kulzer. The base is elastic and impact-resistant. Yamahachi acrylic crowns made in Japan are characterized by increased strength and wear resistance. The milled titanium base ensures uniform load on the jaw.
- Acrylic prosthesis. Orthopedic design made of acrylic obtained by processing under high pressure at high temperatures. This technology will reduce the amount of monomer in plastic and reduce the risk of an allergic reaction. The advantages include a relatively low cost, and the disadvantages are low strength indicators and rapid wear of the crowns.
All-on-6 dental implantation: features and prices in Moscow
The name of the technology for installing a fixed prosthesis on all-on-6 implants can be translated into Russian as “all on six.” This technology is an improved version of the all-on-4 technology and involves the implantation of not four, but six implants.
How is All-on-4 dental implantation performed and how long does it last?
All on 4 implantation is carried out in several stages, the longest of which is preparatory. Direct installation of pins and prostheses takes only a few hours. Soft tissues heal within a week; osseointegration of implants requires an average of 3 to 6 months (premium models take root faster).
Preparation for implantation includes several stages
Preparatory stage
Before installation of implants and artificial jaws, the patient must undergo a thorough examination to exclude complications. The list of diagnostic measures includes:
- Initial appointment and examination. The implant surgeon visually assesses the condition of the gums and teeth and collects anamnesis. Based on the data obtained, recommendations are given on the choice of implants and prostheses, and the preliminary cost of treatment is announced.
- Comprehensive diagnostics. The most important study is computed tomography, which evaluates the location of nerves, vessels and maxillary sinuses, and determines the characteristics of bone tissue (its density, width, height). In addition, CT reveals hidden pathologies - various types of neoplasms, cysts. To assess the condition of the temporomandibular joint, condylography is performed. To make adaptive and permanent dentures, the doctor makes a cast of the jaws.
- 3D modeling. The information obtained during the diagnostic examination is processed by a special program. The result is a three-dimensional model of the jaw, which allows you to create a digital template - visualization of treatment. 3D modeling is necessary to determine the location of fixation of titanium pins and prototyping fixed prostheses on 4 implants.
- Sanitation. Before installing artificial teeth, you need to cure your own teeth from caries, clean them of tartar and plaque. If there are pockets of infectious inflammation in the oral cavity, they also need to be eliminated. These procedures are necessary to prevent complications (inflammatory processes) after implantation.
Surgical stage
Before the procedure begins, anesthesia is administered. Anesthesia can be local or general (in the second case, the patient will not feel anything at all, as he will be asleep). After premedication, the surgeon begins the implantation procedure:
- Untreatable, loose teeth, as well as infected areas of soft tissue are removed.
- In one of two ways – transgingival or flap – titanium pins are inserted into the jaw. The first method is minimally invasive; the implant is fixed through a small puncture in the gum. In the second case, the mucous membrane is incised.
- After completion of the manipulation (on average after 1.5 hours), the wounds are sutured.
Orthopedic stage
The final stage of the “all on 4 implants” method of restoring the dentition. The dentist takes impressions that are needed to make a permanent orthopedic structure. Then abutments are installed on the pins - straight in front and angled on the sides, and then the temporary prosthesis is fixed to them using special screws.
Delayed installation of artificial teeth is also practiced (at the patient’s request) - after the mucous membrane has healed and the sutures have been removed a few days later. After completion of the osseointegration process, which usually lasts from 3 to 6 months, the adaptive orthopedic design is replaced with a permanent one. If a reinforced bar prosthesis is used, replacement can be delayed for up to 3-4 years.
Rehabilitation and care
In the postoperative period, you must visit the dentist according to a pre-agreed individual schedule. Within a week, the sutures are removed and the condition of the soft tissues is assessed. A repeat visit is recommended after a month and a half for those who live near the dental clinic. For out-of-town patients, a delay in visiting a doctor is allowed for up to three months.
The first time after surgery you need to visit the dentist regularly
Pain and swelling in the first days are normal, and they are insignificant, since all manipulations are minimally invasive and are performed by professionals working in our clinic. To eliminate pain, the doctor may recommend taking analgesics, and to prevent inflammation, a course of antibiotics is prescribed. At the same time, the functionality of the prosthesis on 4 implants is assessed. If the patient experiences significant discomfort, the position of the artificial jaw is adjusted. In addition, in the early recovery period there are a number of restrictions associated with habits and lifestyle:
- You should not eat hard, sticky, difficult to chew or too sour foods;
- It is forbidden to drink too hot or cold drinks;
- you should limit physical activity, do not visit the sauna, bathhouse;
- do not use rinses or toothpastes containing fluoride;
- avoid traumatic sports.
During the rehabilitation process, it is important to properly care for the oral cavity and the orthopedic structure itself. Since the base of the denture does not fit tightly to the gum, plaque from food debris and bacteria will form in the resulting space.
Once every six months, professional cleaning of the prosthesis is necessary. The doctor removes the structure, removes plaque from it, and then polishes it. If daily hygiene is insufficient, as evidenced by bad breath, you will have to visit the clinic at least once every 3 months. In addition, acrylic and porcelain composite teeth must be replaced every few years due to wear.
For high-quality cleansing at home, you will need special threads - super-flosses, as well as an irrigator and rinses. In addition, artificial teeth need to be cleaned regularly with a toothbrush.
Comparison with traditional methods of dentures for edentulous patients
There are several alternative options for standard dental prosthetics in the absence of a large number of dental elements or in complete edentia. Let's compare them:
- complete removable dentures – their main advantage is their low price. There are many more disadvantages: unstable fixation in the oral cavity (they can fall out while eating or talking), progressive atrophy of the jaw bone tissue;
- partial removable – used for incomplete edentia, attached to the remaining natural teeth (which gradually become loose).
Note: despite all the advantages of prosthetics on four implants, the patient must remember the need for preventive visits to his doctor twice a year. This is necessary to prevent possible complications and to revise the prosthesis. You can make an appointment at any of the branches of our clinic by calling the number listed on this website.
The network of dental clinics “Smile” offers patients “All-on-4” implantation (implantation on four implants). Contacting our branches has a number of significant advantages:
- operations are performed by highly qualified implantologists;
- diagnostics, surgical stages and prosthetics are carried out in accordance with international standards;
- We practice a highly personalized approach;
- We provide family and cumulative discounts;
- We work according to a schedule convenient for patients: every day until 21:00 (on Sunday until 16:00).
You can make an appointment at any of the branches of our clinic in Moscow, located within walking distance from metro stations:
- Alekseevskaya (VDNKh district, etc. Mira), address: st. 3rd Mytishchiskaya house 3, building 2;
- Shelepikha, address: Shelepikhinskaya embankment, building 34, building 1.
The use of innovative technologies, extensive practice and equipping the clinic with the latest equipment allows us to successfully perform “All-on-4” implantation (implantation on four implants). We guarantee the safety and effectiveness of the services provided. We will restore the attractiveness of your smile!
Possible complications
It must be taken into account that after implantation, complications may develop, the most likely of which are:
- implant rejection – occurs due to biological incompatibility of living tissues with the metal of the structure;
- peri-implantitis is a purulent inflammatory process provoked by infection;
- pain – headaches, as well as localized in the area of implants, temporomandibular joint;
- swelling of the soft tissues, minor bleeding is the norm in the early postoperative period, but if these phenomena are protracted, they are a sign of pathology;
- an unpleasant odor is usually a consequence of improper care of an artificial jaw with 4 implants.
To exclude post-implantation complications, three conditions must be met. First, choose high-quality implants with prostheses from reliable well-known manufacturers. Secondly, contact dental clinics where highly qualified implant surgeons work, like in Yulisty. Thirdly, take proper care of the orthopedic structure - clean it regularly, use an irrigator, and come for professional cleaning on time.
When urgent help is needed
Normally, pain and swelling of the gums disappear a few days after the procedure. Headaches or discomfort in the temporomandibular joint may occur due to atrophy of the masticatory muscles after a long period of absence of teeth. As a rule, they also pass quickly after restoration of muscle function. However, in some cases, urgent medical intervention is necessary:
- prolonged bleeding - can be caused by damage to blood vessels during surgery;
- increasing swelling and pain, increased temperature - signs of an inflammatory process;
- discharge of fluid from the nose is a consequence of damage during implantation of the maxillary sinuses;
- numbness of the jaw is the result of cutting or pinching of the conductive nerves during the installation of implants.
Who is indicated and contraindicated for installation of an “all-on-six” implant prosthesis?
Most of the indications for implantation with six implants will be similar to the indications for the use of all-on-4 technology, however, this type can be used in patients with moderate degrees of bone tissue atrophy. The use of six implants makes it possible to obtain a strong and stable fixation of the temporary prosthesis and reduces the risks of complications.
Contraindications to all-on-6 will also be approximately the same as to all-on-4 technology. Surgery on six implants cannot be performed if the following conditions and diseases are diagnosed in the patient:
— Serious pathologies of the heart and cardiovascular system;
- Diabetes;
— Tuberculosis;
— Hepatitis;
- Oncological diseases;
— Blood diseases that cause deterioration of blood clotting.
Note that these contraindications are relevant not only for all-on-6/ all-on-4, but also for other dental implantation technologies.
Types of implants
All-on-6 implantation technology uses slightly different types of implants than all-on-4 surgery. For all-on-6, special one-piece (one-piece) implants have been developed, which are combined with an abutment. The type of thread on implants is different, this makes it possible to ensure high-quality fixation of the artificial root in the desired area of the jaw.
Is there an alternative to All-on-4
If for some reason prosthetics using the “all on 4 implants” technology cannot be performed, the patient is offered an alternative option.
All-on-3
This technique from Nobel Biocare is used only to restore the dentition of the lower jaw. The operation - surgical and orthopedic stages - lasts about 6 hours. There are two differences from the all-on-4 technology. The first is the number and method of fixing the implants: three support pins are used (one in the center, two on the sides). The second is the possibility of installing a permanent orthopedic structure made of acrylic immediately. Due to these features, the cost of treatment is significantly reduced.
All-on-3 or Trefoil implantation
All-on-6
Suitable for prosthetics of the lower or upper jaw (or both) in the absence of teeth. It is optimal in case of significant lack of bone tissue, its low density, as well as in case of periodontal diseases and bruxism (increased tone of the masticatory muscles). The adaptation prosthesis is fixed on 6 implants on the day of surgery (single-stage technology) or after 3 days. Due to the increased consumption of materials, the procedure is more expensive.
Classic two-step protocol
It is distinguished by its duration and high prices. Before implantation, osteoplasty is required - bone tissue augmentation and sinus lifting (correction of the maxillary sinuses). This stage lasts 4-5 months, after which implants are implanted for each tooth. Osseointegration will take another 1-2 months, and only then the doctor will install abutments with crowns. The cost of this technique exceeds the cost of implantation per day all-on-4 and its analogues.
The table provides a brief comparative description of popular dental implantation techniques. The price for the two-stage protocol is minimal, using the cheapest materials.
| Name | Duration | Traumaticity | Osteoplasty | Total cost, 1 jaw |
| All-on-4 | 1 day | low | Not required | 400 000 |
| All-on-3 | low | 300 000 | ||
| All-on-6 | average | 500 000 | ||
| Two-step protocol | From 6 months | high | Mandatory | From 600,000 |
All-on-4: errors in the clinical approach and ways to solve them
Since its introduction in 2003, the All-on-4 implant treatment concept (Nobel Biocare) has already gained enormous popularity among dentists during the rehabilitation of patients with symptoms of complete edentulism. The high prevalence of the technique is justified by at least two main factors: the predictability of successful treatment results and the economic feasibility of the surgical algorithm.
The essence of the technique is the mandatory use of 4 dental implants, the distal ones of which are deliberately installed in an inclined position at an angle of up to 45 degrees, after which the titanium supports are immediately loaded with provisional structures. According to the literature, the success rate of immediate and long-term treatment results using the All-on-4 concept exceeds 98%. However, although many studies have been devoted to studying the effectiveness of the technique, as well as various options for its modification, the issue of possible complications that may arise with a specific treatment algorithm still remains insufficiently clarified in both scientific and clinical publications. Therefore, the purpose of this article was to demonstrate possible complications when implementing the All-on-4 treatment protocol, as well as to describe effective methods for solving them to achieve the most successful clinical outcome.
The recommendations given are based on the personal experience of the author, who has installed more than 500 prosthetic superstructures, as well as more than 2,000 dental implants during the rehabilitation of his patients using the All-on-Four technique.
Complications before the start of the surgical stage of treatment
Tooth extraction by impression
For many patients, before starting implant treatment, the remaining teeth are often in very poor condition. Due to pathological mobility or periodontal disease, it happens that the teeth “go away” along with the impression taken, therefore, after a thorough examination, the doctor should warn the patient about the possible prospect of “unintentional removal”, so as not to shock him with the current situation (photo 1).
Photo 1. Orthopantomogram of a patient with signs of complex periodontal lesions - a potential candidate for implantation using the All-on-Four technique.
In such situations, the author recommends removing the extracted teeth from the impression, cleaning them, reducing the length of the root and installing them in place in the dentition, connecting them with adjacent teeth like an adhesive Maryland bridge. In this case, the newly installed tooth, of course, must be removed from occlusion. It also happens that a tooth removed through an impression was one of the supports of a partial removable denture: in such cases, the author uses a temporary mini-implant, which he installs in the same procedure, modeling a temporary crown on it. The latter will provide the necessary retention of the removable superstructure before the start of full implantation.
Complications during surgery
Trauma to the artery during the separation of the mucogingival flap
After performing local anesthesia, according to the All-on-4® protocol, the doctor must separate the full mucogingival flap. Given that the anatomy of the vascular structures is quite variable, during this manipulation it is easy to provoke injury, for example, to the great palatine or hypoglossal arteries, which, in turn, will lead to excessive bleeding, limiting the visibility of the working field and increasing the risk of subsequent complications.
Initial treatment in such cases consists of administering a local anesthetic with a concentration of epinephrine of at least 1:100,000, which, due to the vasoconstrictor effect of the drug, helps stop the bleeding. If this approach is ineffective, you can use an electrosurgical coagulator or a laser with a coagulation option. Eventually, the wound can be sutured distal to the bleeding site (Figure 2).
Photo 2. Ligation of a branch of the hypoglossal artery using 4-0 chrome-plated sutures.
Nerve exposure
In cases of severe mandibular atrophy, there is a risk of exposure of the mental or inferior alveolar nerves (Figure 3). To prevent such a complication during surgery, it is necessary to take into account the design of the incision, the degree of separation of the mucogingival flap, the amount of bone resorption, the topography of the implantation area, the degree of soft tissue reduction and the characteristics of wound suturing. When the inferior alveolar nerve is exposed, the author recommends placing an amnion-chorionic membrane (DHACM) directly on the nerve fiber, since the positive results of using it to restore the integrity of the nerve bundle have already been demonstrated during operations to remove the prostate. In only 4 cases from the author’s personal practice, such an approach failed to restore adequate nervous sensitivity, as a result of which the patients experienced symptoms of transitive or permanent anesthesia, paresthesia, hypoesthesia or dysesthesia.
Photo 3. CBCT section: crestal position of the inferior alveolar nerve (at the intersection of the yellow lines), formed as a result of secondary bone resorption. Reduction of bone tissue in this area can cause nerve damage.
Expansion of the volume of the pneumatized maxillary sinus
After tooth loss in the posterior parts of the upper jaw, the so-called process of pneumatization of the maxillary sinus often occurs, the volume of which may extend beyond the level of the expected horizontal plane necessary for the implementation of the “All-on-four” approach (photo 4).
Photo 4. Expansion of the maxillary sinus beyond the horizontal plane of bone reduction (yellow line).
With inadequate bone support, the risk of fracture in the area of supra- and infrastructures increases, not to mention the fact that a deficiency of bone tissue in the distal areas can also provoke perforation of the Schneiderian membrane during surgery. To prevent such complications, the author recommends providing the maximum available visual control of the implantation area, as well as performing apical displacement of the membrane using curettes to form the necessary residual space for the implants (photos 5 - 6).
Photo 5. Exposure of Schneiderian membrane during horizontal bone reduction.
Photo 6. Raising the Schneiderian membrane using a curette.
Bone reduction and membrane elevation are carried out until the necessary clinical conditions for the placement of intraosseous supports are recreated (Figure 7). At the same time, the author does not augment such surgical sites and simply sutures mucogingival flaps. So far, none of the author’s personal patients have had any complications due to the implementation of this particular surgical approach (photo 8).
Photo 7. View of the ridge after lifting the Schneiderian membrane, horizontal reduction of the bone tissue and installation of the implant.
Photo 8. Orthopantomogram of the patient shown in photos 5-7.
Bleeding from bone nutrient tubules
During the All-on-4 protocol, alveolar ridge and/or basal bone reduction procedures are typically required (Figure 9) to provide adequate space for subsequent placement of provisional and definitive prosthetic restorations. During the leveling of bone tissue, its nutrient canals are exposed, which provokes bleeding. The latter, in turn, not only limits visual control of the working field, but also carries the risk of excessive blood loss. It is even possible that several sources of bleeding may form, but such cases are extremely rare in practice. If such complications occur, the author recommends the use of a blunt-tipped Woodson hand instrument (Figure 10), which can apply firm pressure to the area of bone immediately adjacent to the bleeding nutrient canal. This technique helps to deform the adjacent bone area so that it simply plugs the hemorrhage. In the author’s personal practice, such an approach always ensured the achievement of the desired clinical result.
Photo 9. Reduction of the bone crest of the lower jaw before implantation.
Figure 10. Using a Woodson instrument to condense bone during nutrient tubule bleeding.
Additional mental hole
According to the literature, the frequency of the presence of additional mental foramina ranges from 2.7-13% (photo 11). These anatomical formations significantly complicate the implantation procedure using the “All-on-4” protocol, since the topography of the mental foramen is a kind of landmark for determining the position of installation of implants in the distal parts of the jaw (photo 12).
Photo 11. Presence of an additional mental foramen.
Photo 12. CBCT view of the accessory mental foramen.
Due to the presence of an additional mental foramen, doctors often have to install intraosseous supports in a more mesial position, thereby reducing the anteroposterior length of the prosthesis supported by 4 implants. In cases where the additional mental foramen is located above the main one, the doctor is also limited in the possibilities of performing bone tissue reduction, which increases the risk of a possible fracture of the prosthetic superstructure. Therefore, to verify such anatomical variations before implantation, the patient must undergo cone beam computed tomography (CBCT), which will help detect all mental foramina at the stage of intervention planning (photo 13).
Photo 13. The mental foramen is a kind of landmark for determining the inclination of the implants in the distal areas.
Although, according to the literature, even a thorough analysis of CT images does not provide conditions for 100% identification of all mental foramina, so the doctor should always remain extremely careful when separating flaps in the area of the implantation bed to prevent possible nerve damage.
In the presence of additional mental foramina, the author recommends a modified bone reduction procedure, combining it with a more mesial placement of dental implants in the posterior areas of the jaw. This approach helps to avoid possible neurological complications in the form of permanent or transient anesthesia, paresthesia, hypesthesia or dysesthesia.
Damage to the hypoglossal artery in the anterior region of the lower jaw
Given that the All-on-4 protocol involves placing implants anterior to the mental foramen, special attention should be paid to studying the vascular system of this area. A number of publications have even described potentially life-threatening iatrogenic complications that can arise from damage to blood vessels in the frontal region of the mandible. According to a 2015 literature review, the majority of immediate or delayed bleeding after implantation was compromised by damage to the hypoglossal artery. And although the review of the literature noted that no deaths from such complications have yet been recorded, 41% of patients required tracheal intubation, and 47% required a tracheotomy. Therefore, prevention of damage to the hypoglossal artery in the anterior region of the mandible is a key aspect of well-planned iatrogenic intervention. During the study of cadaveric material and CBCT results, it was found that most often the opening of the entrance of the hypoglossal artery into the bone tissue is located in the middle of the lower jaw. Normally, this anatomical formation does not in any way affect the effectiveness of the bone reduction procedure, but with significant resorption of the alveolar ridge, it becomes a real problem for clinicians. In such situations, the author simply recommends modifying the amount of bone reduction in the frontal area of the lower jaw, thus providing conditions for safe installation of the implant without the risk of damaging the vascular bundle, as well as for creating the necessary space for the construction of a provisional prosthesis.
Inadequate bone density
Numerous studies indicate that high primary implant stability is favorable for successful immediate loading of the intraosseous support, and high screw torque values correlate with primary stability parameters of the infrastructure. However, both torque and primary stability of the implant are largely dependent on bone density: denser bone provides more favorable conditions for implantation. In case of insufficiently dense or “soft” bone, some authors recommend underpreparing the implantation area, which, in their opinion, helps to achieve improved stability of the structures. On the other hand, there are situations in which, even with an underprepared bone bed, it is not possible to achieve correspondingly high torque values.
In such cases, regardless of whether the operation is on the lower or upper jaw, the author recommends installing an implant of a larger diameter and the same length than the one with which it was not possible to achieve an adequate torque parameter. If this approach fails to achieve the desired stability, it is recommended to choose a longer implant. In the maxilla, the support can be extended to the vomer or lateral pyriform ridge, thus providing better stability of the structure in its apical part. In the area of the lower jaw, a similar effect can be achieved by fixing the implant in the area of the lower cortical plate (photo 14 - 15).
Photo 14. View of dental implants, additionally fixed in the area of the cortical plate of the lower edge of the jaw.
Photo 15. CBCT slice: fixation of the implant in the area of the dense cortical plate of the lower edge of the mandible.
Removal of dental implants
In some clinical cases, the implementation of the “All-on-4” approach requires the removal of previously installed dental implants (photos 16 - 17), some of which may be quite well osseointegrated. The inability to use such structures with the All-on-4 protocol is most often due to the level of their installation, which is too coronal for fixation with a full prosthetic restoration on four supports. In addition, previously placed implants limit the ability to achieve adequate bone reduction. From the author’s personal experience, it can be summarized that the use of previously installed intraosseous screws in the algori structure provokes a decrease in the thickness of future superstructures, which, in turn, significantly increases the risk of their fracture during operation. In order to prevent such complications, it is still better to remove previously installed implants.
Photo 16. Orthopantomogram of the patient before treatment: the presence of previous implants requiring removal; implants in the right lower quadrant are too close to the inferior alveolar nerve.
Photo 17. View of the same patient after implementation of the All-on-4 protocol.
As a rule, the diameter of the implants to be removed and the implants suitable for future installation is similar. Removal, of course, is best done with a reverse torque tool (photo 18), since this allows for the maximum amount of bone to be preserved, providing conditions for the installation of a similar implant. If it is not possible to remove the implant in the manner described above, then it is no longer possible to do without trepanation intervention. Such a procedure is fraught with significant loss of surrounding bone volume, which limits the immediate installation of the required implant with its immediate loading with a provisional prosthesis. The author recommends removing most implants using a reverse torque instrument, and when performing trephination, installing wider and longer intraosseous supports.
Photo 18. Using a reverse torque device to remove implants.
Postoperative complications
Fracture of temporary structures
With adequate implementation of the All-on-4 protocol, postoperative complications occur quite rarely. The most common of them, according to the literature, are fractures of provisional restorations, which occur with a frequency of 4.17% to 41% of cases. Such complications are quite serious, since they limit the stabilization of the prosthetic arch and also provoke an incorrect distribution of operating stresses. For patients, fractures of provisional restorations are also fraught with the fact that they disrupt the function of normal chewing of food, not to mention compromising aesthetic parameters. The causes of fractures of suprastructures are insufficient amount of bone tissue reduction, errors in the manufacture of prostheses, as well as fixation of incorrect bite position. In some cases, fractures may occur due to prolonged use of acrylic and polymethyl methacrylate materials under severe occlusal loads.
In order to reduce the incidence of such complications, the author strengthens temporary prostheses using steel wire 1 mm in diameter (photo 19 - 20). The effective results of this approach have already been quite well described in studies by Yamaguchi, Li and other clinicians. After reinforcement of temporary superstructures, the author’s fracture rate decreased from 16.14% to 4.17%.
Photo 19. Reinforced provisional prosthesis.
Photo 20. The final view of the provisional restoration supported by 4 implants.
conclusions
Although the “All-on-4” approach to dental rehabilitation of patients with complete edentia provides some of the highest success rates, it should be remembered that this method is also one of the most difficult to implement and is fraught with its own specific complications. But with careful planning and understanding of the nature of such complications, as well as taking all measures to prevent them, doctors can safely guarantee the high efficiency of prosthetic rehabilitation of patients supported by only four dental implants.
Author: Dan Holtzclaw, DDS, MS (Austin, TX, USA)
How much does All-on-4 implantation cost?
When planning the cost of prosthetics using the “all on 4 implants” technology, you should take into account that the final cost is always calculated individually. The prices listed on the website are approximate, since the final amount for treatment is determined by a combination of several factors. These include:
- The severity of the clinical case. The degree of edentia, the condition of the remaining teeth and soft tissues significantly affect the price of prosthetics. The need for large-scale treatment at the preliminary stage increases it.
- A variety of titanium implants, as well as adaptive and permanent orthopedic structures. The more famous the manufacturing company, the better and more expensive the materials (they take root easier and last longer).
- Qualification, experience, regalia of an implant surgeon. The services of a high-class professional are always expensive, since in this case the quality of prosthetics and the absence of postoperative complications are guaranteed.
- Costs for replacing prosthetic elements. Crowns wear out over time and need to be replaced periodically. Acrylic - once every 4-5 years (with a 2-year warranty), metal-ceramic - less often. In this case, accidental breakdowns and damage to the structure may occur after the warranty period has expired. In such cases, maintenance costs also increase.
It should also be taken into account that hygienic care of an artificial jaw will also require material costs. If it is enough to simply clean a removable denture with a brush every day, to maintain fixed structures you will have to additionally spend money on super-flosses and an irrigator.
Disadvantages of fixed prosthetics on all-on-4 implants and their possible risks
The all-on-4 dental implantation operation has its disadvantages, including:
1. The inability to apply this implantation technology in some clinical cases. All-on-4 implantation is strictly contraindicated in some chronic general diseases. For example, it cannot be used in patients with diabetes. All-on-four and all-on-six implant technologies are not suitable for smokers. For nicotine-dependent people, basal implantation is more suitable.
2. All-on-4 surgery requires careful planning and, ideally, the development of surgical templates in a guided implantation program. This definitely increases treatment costs, but guarantees high quality implantation.
3. “All on four” is an implantation technology that is applicable for bone tissue atrophy, but it cannot be used in patients with excessively loose bone, which will not allow for high-quality primary stabilization of implants.
And one more important point: all-on-4 implantation has been used relatively recently in Russia. For this reason, not every dental clinic has a doctor who can perform this complex operation accurately, competently and without errors. And for the same reason, you should pay maximum attention to the choice of dentistry where you will receive all-on-4 dental implantation. The slightest inaccuracy in choosing the place for implantation, or deviation when screwing them in by even a millimeter can lead to loosening and rejection of artificial roots. Treating such complications after implantation is both difficult and expensive!
Is preparation necessary?
The prosthetic procedure using All on 4 technology refers to a one-stage type of implantation with instant loading and is performed in one session. But implantation involves surgical intervention and implantation of a foreign body, so it is impossible to do without preliminary preparation aimed at reducing the risks of complications.
Preparation for implantation with complete edentia includes:
- laboratory blood test;
- computed tomography of the jaw;
- treatment of diseases of the oral cavity (gums, mucous membranes, etc.).
Since the prosthesis will be installed immediately after the installation of the implants, the preparation period also includes the manufacture of the structure. To do this, impressions can be taken or a model of the jaw can be created using special 3D programs.
Diagnostics is necessary to determine the characteristics of the condition of the jaw, the location of implantation and to exclude contraindications.
It is not recommended to do implantation if you have developed periodontitis or periodontal disease, diseases of the immune system, severe heart or vascular disease, bleeding disorders and diabetes mellitus. Contraindications are pregnancy and lactation.