A child’s malocclusion is not a problem today. An orthodontist will definitely be able to solve it. Basically, parents resort to his help when the child is 5-6 years old. The most important thing is to consult a doctor in time without waiting for the eruption of permanent teeth. There are different ways to correct a bite in children. A child's bite can be corrected faster than an adult's. A child is a growing organism. His teeth are easy to move during this period.
Periods of occlusion
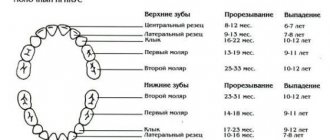
There are several periods of development of occlusion in humans:
- First period: newborn period. During this period, babies still have no teeth.
- Second period: teething time. It begins from the moment the first baby tooth appears and ends with the eruption of all twenty.
- Third period: time of mixed dentition. It begins from the moment the milk teeth are replaced by permanent ones.
- The fourth period (final): the time of formation of a permanent dentition. During this period, all molars should be in the mouth.
Classification and stages of development of open bite
Open bite is distinguished depending on its location. In this case, front and side options are distinguished. There are also types of open bite based on jaw location. These are combined options that affect both jaws, as well as the maxillary and mandibular.
Traditionally in dentistry, there are three stages of development of such a defect as an open bite, which differ in the degree of its severity:
- At the first stage, the gap between the teeth does not exceed 5 mm.
- At the second stage, it can range from 5 to 9 mm.
- The third stage is characterized by a gap larger than 9 mm.
Depending on the stage of the disease, the doctor will select the most effective treatment method.
Ways to correct bite in children
There are several ways to correct a child’s bite:
1. Myotherapy. With its help, the bite is corrected in children without braces. The method includes special exercises that perfectly train the chewing and facial muscles. The method is popular in the treatment of young children (from four years old). When prescribing and applying such treatment, it is very important to know that the child consciously understands why and how he needs to perform the exercises correctly. During classes you cannot do without adult supervision. You should also remember about the regularity of exercises.
2. Hardware. The method consists of the use of special structures (braces, trainers, plates). These devices can be used after the age of six.
3. Surgical. The method involves performing surgery on the jaw.
4. Orthopedic . The bite is corrected using orthopedic structures (veneers).
5. Comprehensive . Consists of several methods.
Consequences
What complications can arise if a child’s malocclusion is not corrected? Possible consequences:
- tooth abrasion, premature wear, increased risk of caries;
- difficulty chewing causes gastrointestinal problems;
- mucosal injuries, gum inflammation, periodontal disease;
- increased load on the temporomandibular joint, pain, inflammation;
- breathing problems, ENT diseases;
- pinched nerves in the cervical spine;
- aesthetic facial defects, asymmetry;
- psychological problems;
- violation of diction.
Thus, malocclusion in children is dangerous for the development of diseases. It directly affects the emotional state of the individual, self-esteem, and self-confidence. If the bite is not corrected in time, physiological, psychological and aesthetic problems may develop.
Application of records
The design does not require constant wear and is a removable device. It is usually removed during meals or under other circumstances when the baby feels discomfort from it.
The design has several metal elements (screws, hooks, arcs and springs). It is made separately for each patient. The manufacturing procedure is as follows: an orthodontist examines, takes impressions of the jaw, a plaster model is cast in the laboratory based on the impressions, and a plate is made based on the resulting model. The orthodontist independently adjusts the position of the springs and hooks. Such actions by the doctor allow you to move the teeth and dentition in the right direction.
Plates effectively correct malocclusion in the early stages. But sometimes you can hear from friends that the above-described structures did not allow their children to correct their bite. It is not true. With constant wear and compliance with all the recommendations of the orthodontist, the desired result will definitely occur. Although the plates are not permanently installed devices, they must be worn without removing them. It is allowed to remove the structures only when eating, brushing your teeth and in some other life situations (for example, when taking photographs).
Some capricious children do not want to wear records. The task of parents is to convey to the child information about the need for treatment. At the same time, there is an urgent need for constant monitoring of the child. You will need to monitor whether the child has removed the device.
Why are braces better than removable appliances?
Recently, parents are increasingly choosing braces instead of plates. Modern children live an active life - they attend clubs and sports clubs. With this rhythm, parents, who themselves usually work a lot, cannot control the child all the time. Children often forget to put on records and lose or break them. And in orthodontic treatment, regularity and continuity are important. If you do not wear the device for more than 1-2 weeks, it will not fit and you will have to make a new one. Each repair and replacement is subject to payment. As a result, treatment becomes unproductive and expensive.
The braces cannot be removed or lost, but they are quite difficult to remove. In addition, they do not need to be cleaned and washed separately; it is enough to use a brush and a special brush when brushing your teeth as usual.
The most important advantages of braces are the speed of alignment, the ability to correct complex pathologies and a more stable result.
Using trainers
Trainers are not made from casts. They are produced by special companies. They are made from silicone. Such designs are also widely used to correct malocclusion in early childhood.
Trainers are removable devices. This device for correcting malocclusion in children only needs to be worn for a short time. For example, at night and three hours during the day.
The material allows the teeth to quickly adapt to the correct position. In addition to the main treatment, trainers are used to consolidate the achieved results in teeth alignment and to eliminate certain defects.
The main indication for the use of trainers is crowded teeth. In addition, the devices effectively straighten teeth if there are gaps between teeth. However, correction of bites with large gaps is more relevant to adult patients. In children with baby teeth, the defect will correct itself when permanent teeth appear.
In addition to trainers, modern orthodontic practice uses LM-activator and myobrace devices.
A favorite benefit of trainers for patients is their invisibility. Little patients who wear such designs do not feel discomfort when communicating.
Dental trainers are recommended for use in the following cases:
- It is impossible to install an effective braces system.
- The patient's speech is impaired.
- There is an urgent need to wean yourself from a bad habit: thumb sucking.
- Improper swallowing.
- Difficulty breathing through the nose.
- With a deep, open bite.
- With a small bite defect.
Types of trainers in orthodontics
- Initial (blue). It is made from a very flexible material.
- Final (pink, red). The trainer material is harder. It has a stronger effect on the teeth than the initial trainer.
At what age should you start correcting bites in children with trainers? It's better if it's 5-8 years. The method is effective and painless. Early treatment for malocclusion in children will give a 90% success rate.
At the age of 6-12 years, the first teeth of babies change to permanent ones. During this period, the jaw bones grow very actively, giving space for new teeth to emerge. If you use trainers during the specified period of change in bite, then in the future the jaw will develop correctly. This will avoid expensive treatment in the future.
Trainers must be washed after food has entered your mouth. You need to hold them firmly in your hand. This device must not be allowed to fall. Even for disinfection, trainers should not be boiled or washed under very hot (and, conversely, cold) water.
You should always remember that there are leveling devices in your mouth. Therefore, it is forbidden to chew trainers and squeeze them tightly with your teeth.
Trainers need to be carefully monitored. Carry out periodic inspection. Damage is not acceptable. It is better to store devices in a special container.
Prevention
Prevention of the development of malocclusion in children begins at an early age. By following simple recommendations, you can avoid problems and maintain your baby’s beautiful smile.
Dentists' advice:
- Correct attachment to the breast or bottle. Usually a new mother will be helped with this by a pediatric nurse or a breastfeeding specialist.
- Prevent the development of bad habits, gradually abandon the pacifier when the first teeth appear.
- Supplement your diet with solid food in a timely manner.
- Keep your mouth clean.
- Perform gymnastics to develop facial muscles.
The effectiveness of preventive measures can be monitored by a local dentist, whose consultation is recommended for children at least once a year.
The health of a child’s teeth affects not only the appearance, but also the functioning of the entire body. Incorrect bite is the cause of serious illnesses. Therefore, it is important to identify pathologies in time and correct them using methods available for a given age.
Application of braces
These are permanent structures. Braces are attached to each tooth individually. The design includes ligatures, arches, springs and braces. These devices are installed at the age of 12. Then the baby has only permanent teeth in his mouth.
While wearing them, you often have to visit the orthodontist. He adjusts the tension using a wire. The little child will have to wear them around the clock. Therefore, it is important to convey to the little patient that he will have to do this. In addition, the child will have to change his favorite habits. For example, he is strictly forbidden to chew gum and eat solid (nuts) food.
Braces are:
- sapphire;
- metal;
- ceramic.
Sapphire systems, due to the material used, are not noticeable on the teeth. But they are only suitable for people with white enamel color. The design is not painted and does not retain plaque or food debris. The disadvantage is the time it takes to correct uneven teeth. It is larger than that of metal braces.
The metal version is the simplest, cheapest and very old. The entire structure is attached to the outside of the teeth. The positive feature of steel braces is their good strength, the disadvantage is their unaesthetic appearance.
The modern version of braces includes ceramic braces. They are aesthetic, relatively inexpensive and invisible.
Possible complications
Open vertical occlusion does not remain without consequences. The aesthetics of the face and smile suffer, difficulties develop in other functional departments:
- Digestion is disrupted due to problems with biting and chewing;
- the person has a lisp, and with a large gap, speech is slurred;
- The TMJ (temporomandibular joint) experiences difficulties, muscle tone decreases;
- the condition of the periodontium worsens (it experiences excessive load);
- the abrasion of the enamel of the teeth, on which all the work “falls”, increases, they are more loaded and experience increased pressure;
- Mouth breathing develops problems with the ENT organs and respiratory system.
Surgical method
The treatment methods described above are conservative methods for correcting malocclusion in children. But they don't always help. If the defect and anomalies are very pronounced, then they resort to the help of surgeons. During treatment, the orthodontist and surgeon work together.
There is no need to assume that surgical care is needed only for aesthetics. Here the health of the patient is at stake. An incorrect bite will lead to gastrointestinal problems over a short period of time.
Orthodontists do not undergo surgery if the problem can be solved with mouthguards or other devices. Such an intervention allows you to shift the facial structure and correct skeletal deformities.
The operation to correct the bite is performed under general anesthesia. The jaw system is placed in the correct position and fixed with a prepared splint. It is worn for 2 weeks.
Methods for correcting malocclusion in children sometimes require the removal of one or more teeth. Doctors use the gaps left after teeth removal for straightening. Removal is resorted to in the presence of very important factors and a complete diagnosis of the mouth.
When does a child need to have their bite corrected?
Parents should note all important details in the child’s unconscious behavior. Pay attention to how the child breathes, whether his mouth is often open, whether he snores in his sleep, what position the lower jaw is in, whether he likes to gnaw hard objects - these factors have a huge impact on the development of dental pathologies. Take a closer look at the posture and structure of the foot, these are also important indicators of possible violations. Did you find any deviations? Consult a professional.
Risk factors
- difficulties with nasal breathing, for example, due to adenoids or allergies;
- spinal column deformity;
- bad habits;
- genetic predisposition to dental anomalies;
- diseases of the central nervous system.
If the listed risk factors are present, treatment will be effective only with the participation of doctors from related fields. Therefore, it is best to contact myofunctional centers, which unite orthopedists, pediatric dentists, orthodontists and osteopaths. The joint work of specialists guarantees accurate diagnosis and successful resolution of the issue.
Orthodontic method
Incorrect child bites can be corrected using screws, trays and veneers.
Mouthguards align the entire row of teeth. They are made individually. Once every 2 months the structures are replaced with new ones. Mouthguards cannot correct complex cases (mesial, deep, distal bite).
Veneers restore the front teeth well, thereby helping to visually hide an incorrect bite. Composite veneers are not durable, ceramic ones are expensive. The use of veneers requires grinding down the tooth enamel.
Orthodontic screws and appliances are used for crossbites. The devices operate on the principle of mechanics.
Types of violations
Dentists distinguish the following types of malocclusion:
- distal – the upper part protrudes forward;
- mesial – the lower jaw protrudes forward;
- deep – the upper teeth overlap the lower teeth excessively;
- open – there is no closure of the front teeth while the back teeth are closed;
- cross – the lower teeth overlap the upper teeth partially or completely.
Additionally, excessive crowding or sparseness of teeth and disorders affecting individual elements (turns, tilts, various displacements relative to the axis) are also distinguished. There are often conditions in which a combination of several problems occurs simultaneously.
Care
Parents should show their child how to properly care for installed devices. Poor hygiene will greatly increase the risk of dental caries. Maintenance consists of regular cleaning. It is advisable to have a separate brush for plates and trays. In addition to it, you can use pastes and gels sold through the pharmacy chain.
Special attention must be paid to braces systems. Due to the fact that it is not removable, a large amount of food gets stuck in the structure. Therefore, it needs to be cleaned after each use. Threads and brushes will be used to help the patient.
Parents either must teach the baby to perform care procedures correctly or take on the entire process themselves. Here control from the older generation is necessary.
Signs
Visual signs of an open bite:
- a downwardly displaced chin and an enlarged lower part of the face;
- half-open mouth;
- the upper lip is narrow and tense at the moment of closure;
- the sky is shifted down and back;
- the nasolabial fold is smoothed.
Intraoral symptoms:
- vertical interdental gap;
- the first molars close in their normal position, but the incisors do not;
- trapezoidal shape of the lower jaw;
- the jaw arches narrow;
- crowding of the lower incisors due to lack of space;
- the height of the lateral parts of the jaw is greater than usual;
- the mucous membrane is often inflamed, the gingival papillae are deformed;
- macroglossia (enlarged tongue).
Lisp and slurred speech are also one of the signs of pathology. The patient breathes frequently through his mouth. Swallowing is infantile. It is difficult for him to bite off due to a violation of the closure of the teeth and chew food.
How to warn?
If a child has a malocclusion at the genetic level, then, unfortunately, this fact cannot be prevented. But other factors can be significantly minimized. To do this, read the following tips:
- The rudiments of teeth are formed in the fetus at 20 weeks. Therefore, the expectant mother is obliged to eat foods with fluoride and calcium.
- Artificial feeding has a bad effect on the bite. The upper jaw of newborns is larger than the opposite one. Their sizes eventually come to the same value due to breastfeeding. At this time, the facial muscles are actively trained. When your baby feeds from a bottle, the hole in the nipple is larger than the “hole” in the breast. It turns out that the child does not suck, but drinks milk in sips.
- Always pay attention to your child's breathing. It should be through the nose. Be sure to consult a specialist if you notice any irregularities.
- When your baby's first teeth begin to appear, wean him off the pacifier or your finger (if he takes it). The risk of malocclusion increases.
- Visit the dentist even for no apparent reason (2 times a year).
In conclusion, we remind you that for a small child the time needed to correct the bite will be less than for older children.
Sources used:
- https://www.dentsplysirona.com
- Feres MF, Abreu LG, Insabralde NM, Almeida MR, Flores-Mir C (June 2016). “Effectiveness of the open bite treatment in growing children and adolescents. A systematic review". European Journal of Orthodontics.
- Fishchev, S.B. Emergencies in dentistry and maxillofacial surgery.
Short frenulum of the tongue, upper and lower lips
- A short frenulum of the tongue is, in most cases, a hereditary problem that leads to problems with sucking, diction, and in complex cases, over time leads to recession (loss) of the gums on the lingual side of the lower dentition. Often the best option is frenuloplasty at an early age (often before one year), in which case speech therapy problems will not arise. The procedure itself takes several tens of seconds, since the frenulum has neither blood vessels nor nerve endings. Therefore, if a pathology is detected by doctors or parents, plastic surgery is performed at any age, including immediately after birth.
- A short frenulum of the upper lip is a common anomaly (occurs in 10% of the population). Likewise, it can lead to problems with sucking, diction and gum recession in the future. Among other things, low attachment of the frenulum (normal attachment of the frenulum is 0.5 cm above the necks of the incisors) leads to the appearance of a gap between the central incisors - a diastema. In most cases, frenuloplasty is required. It is believed that the optimal age for this is about 7-8 years (after the eruption of the upper lateral incisors), but it can fluctuate. Before this age, interventions are not recommended for two reasons: the problem may disappear on its own (as the jaw grows and permanent teeth erupt, the frenulum may stretch and the place of its attachment may shift), secondly, plastic surgery of the frenulum at an early age can cause the correct development of the upper jaw and lead to malocclusion. Plastic surgery is not a traumatic procedure and is performed on an outpatient basis under local anesthesia.
Short frenulum of the upper lip, diastema, as a result.
- A short frenulum of the lower lip is less common and can also lead to problems with sucking and gum recession in the future. Treatment is similar to the previous anomaly at the age of 6-7 years (after the eruption of the 4 lower incisors).