A. A. Glotova , periodontist, dental clinic “DENTiK LUX”, member of the Russian Periodontal Association RPA (Krasnodar)
E. N. Shastin Professor of RAE, Head of the dental clinic “DENTiK LUX” (Krasnodar)
The article describes the etiology, pathogenesis, and clinical cases of peri-implant tissue disease. Data are presented indicating a connection between periodontal diseases and dental implants. The need for comprehensive treatment of periodontal diseases prior to implantation is described.
Dental implants have revolutionized dentistry, providing new hope for millions of people with missing teeth. Since the debut of implants in the 1960s, we have made great strides in understanding the biology of osseointegration. However, with an increase in the number of implants installed, the number of late complications also increases: mucositis, peri-implantitis, complete disintegration.
According to epidemiological studies, after 10 years, peri-implantitis develops in approximately 40% of patients who receive implants, while mucositis in the implant area occurs in approximately 80% of patients. ( Berglund at al 2015 Clin Periodontolog & Implant Dentistry, Eke at al. J Dent Res 2012, Kassebaum at ol Dent Rec 2014).
In almost every book on implantation you will find that the success rate of this treatment method today, with modern equipment and the latest technologies, is 98% or higher, and the survival rate of implants for 10 years is 95–97%.
The Heterburg Study of the Swedish Population
This study (Journal on Dental Researelu 2015 Effectiveness of Implant Therapy analyzed in a Swedish population) is by far the largest on implant survival. Of the 25,000 patients with implants installed in 2003, 4,716 patients were selected. Early implant loss was 4.4% (121 patients) on the patient side and 1.4% (154 implants) on the implant side. Nine years after implant treatment, 596 patients with 2367 implants were evaluated. Late loss was 4.2% on the patient side (25 patients), and 2% on the implant side (47 implants). Overall loss: patients 7.6%, implants 3%.
When assessing the prevalence of caries or periodontitis, the number of patients with these diseases is considered, and not the number of affected teeth, so implantation failure should be assessed in terms of the number of patients, not implants. Thus, the survival rate of implants over 10 years is 93%, and not 97%, these data allow a more realistic assessment of the result and improve clinical work.
Biological width and periodontal complex
In the implant field, biological width is also defined as the distance from the most prominent coronal projection of the connective epithelium to the alveolar bone, including the epithelium (approximately 1 mm) and the connective tissue attachment (approximately 1 mm). By analogy with a tooth, the dentogingival complex additionally contains a section of the implant-gingival sulcus (approximately 1 mm). If this distance is less, resorption of the bone ridge surrounding the implant should be expected (Clin Oral Implants Res. 1991 Apr-Jun; 2(2):81-90 “The soft tissue barrier at implants and teeth” Berglundh T., Lindhe J., Ericsson I., Marinello C.P., Liljenberg B., Thomsen P.).
Biomechanical considerations[edit]
Biological width[edit]
Biological width
is the natural distance between the base of the gingival sulcus
(G)
and the height of the alveolar bone
(I)
.
The gingival sulcus (G)
is a small gap that lies between the enamel of the crown of the tooth and the sulcular epithelium.
At the base of this gap lies the junctional epithelium, which is attached to the surface of the tooth through hemidesmosomes, and the height from the base of the gap to the alveolar bone (C)
is approximately 2 mm.
Biological width is the distance determined by the “attachment of the connective epithelium and connective tissue to the root surface” of the tooth. The concept was first published by Ingber JS, Rose LF and Coslet JG. — “Biological width” was a concept in periodontics and restorative dentistry in 1977 at Alpha Omegan. It was based on cadaver measurements by Gargiulo, Wentz, and Orban, who did not use the term "biological width" or give it any clinical meaning in their 1961 paper. The real name "Biological Width" came in 1962 from Dr. D. Walter Cohen of the University of Pennsylvania. [1] A In other words, it is the height between the deepest point of the gingival sulcus and the crest of the alveolar bone. This distance is important to consider when fabricating dental restorations, as they must take into account the natural architecture of the gingival attachment to avoid harmful consequences. The biological width depends on the patient and can vary from 0.75 to 4.3 mm. [3]
Based on Gargiulo's 1961 paper, the average biological width was determined to be 2.04 mm, of which 1.07 mm is occupied by connective tissue attachments and another about 0.97 mm is occupied by connective epithelium. [1] [4] Because it is not possible to completely restore a tooth to the exact coronal edge of the junctional epithelium, it is often recommended to remove enough bone to leave 3 mm between the restorative edge and the alveolar bone crest. [5] [6] [7] When restorations do not take these considerations into account and violate biological width, three things happen: [3]
- chronic pain
- chronic inflammation of the gums
- unpredictable alveolar bone loss
Ferrule effect[edit]
In addition to crown extension to ensure proper biological width, 2 mm of tooth structure must be available to provide a tip effect. [8] The collar, in relation to the teeth, is a strip that surrounds the outer dimension of the residual tooth structure, as opposed to the metal strips that exist around the cylinder. A sufficient vertical height of the tooth structure, which will be captured by the future crown, is necessary to ensure the ferrule effect of the future prosthetic crown; it has been shown to significantly reduce the incidence of fractures in endodontically treated teeth. [9] Because the beveled tooth structure is not parallel to the vertical axis of the tooth, it does not adequately affect tip height; thus, the desire to bevel the crown margin by 1 mm will require an additional 1 mm of bone removal when lengthening the crown. [10] However, restorations are often performed without such a chamfer.
Some recent research suggests that while a ring tip is certainly desirable, it should not be placed at the expense of the remaining tooth/root structure. [11] On the other hand, it has also been shown that “the difference between an effective long-term restoration and failure can be as little as 1 mm of additional tooth structure, which, when encased, provides excellent protection. . When it is not possible to create such a long-lasting functional restoration, tooth extraction should be considered." [12]
Relationship between crown and root[edit]
The alveolar bone surrounding one tooth will naturally surround the adjacent tooth and removing bone for a crown lengthening procedure will effectively damage the bony support of adjacent teeth to some unavoidable extent, as well as adversely increase the crown-to-root ratio. In addition, once the bone is removed, it is almost impossible to restore it to its previous level, and in the event that the patient chooses to receive an implant in the future, there may not be enough bone in the area after the crown lengthening procedure. completed. Therefore, it would be wise for patients to carefully discuss all treatment planning options with their dentist before undergoing a permanent procedure such as crown lengthening.
Treatment planning[edit]
Replacement of unsightly crowns on the upper central teeth after lengthening the crowns and making new restorations.
Crown lengthening is often performed in combination with several other expensive and time-consuming procedures, with the overall goal of improving the prognosis of dental restorations. If a tooth, due to the relative lack of solid tooth structure, also requires a post and rod and therefore endodontic treatment, the total time, effort and cost of the various procedures, as well as the worsening prognosis due to the cumulative failure rate inherent in each procedure, can combine to make it is advisable to remove the tooth. If the patient and extraction site are suitable candidates, it may be possible to place an implant, place and restore it with a more esthetic, timely, inexpensive and reliable result. It is important to consider the many options available during the planning stages of your dental care.
An alternative to surgical crown lengthening is forced orthodontic eruption, which is non-invasive, does not remove or damage bone, and can be cost-effective. The tooth is squeezed out a couple of millimeters with simple bracketing of the adjacent teeth, and with a little effort it only takes a couple of months. Fiberotomy is performed after crown lengthening and is easily performed by a general dentist. In many cases like this one shown, surgery and extraction can be avoided if the patient is treated orthodontically rather than periodontally. [ citation needed
]
Etiology
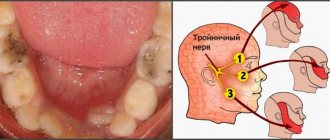
According to the report of the sixth European Workshop on Periodontology in 2008, mucositis and peri-implantitis are recognized as infectious diseases caused by bacteria (Cindy & Meyle, 2008, Consensus Report EP6). Mucositis is an inflammatory lesion that is limited to the mucosa around the implant (Fig. 1 a, b, c). Peri-implantitis is a pathological condition that occurs in the tissues surrounding dental implants, caused by microorganisms and characterized by tissue inflammation and bone loss around the implant (Fig. 2, 3 a, b).
Rice. 1 a. Level of bone tissue at the time of fixation of the metal-ceramic bridge.
Rice. 1 b. Peri-implant mucositis. The patient, 5 years after fixing the bridge, complained of discomfort in the area of the implants.
Rice. 1st century Level of bone tissue 5 years after fixation of a metal-ceramic bridge. There is no pathological resorption in the implant area, the diagnosis of mucositis is confirmed.
Rice. 2. Peri-implantitis. Bone resorption for 2/3 of the implant length 3 years after implant placement.
Rice. 3 a. Hygiene is unsatisfactory. 6 months after permanent prosthetics, peri-implantitis was diagnosed.
Rice. 3 b. Hygiene is unsatisfactory. 6 months after permanent prosthetics, peri-implantitis was diagnosed.
In recent years, numerous experimental and clinical studies have established that the formation of bacterial biofilm is the main etiological factor in the development and progression of peri-implantitis. The main types of subgingival bacteria include Peptostreptococcus micros, Fusobacterium nucleatum, Prevotella intermedia.
Inflammation of the gums and bone around implants develops under the influence of gram-negative anaerobic microflora, which is also associated with periodontitis. With peri-implantitis, a large number of periodontal pathogens are found, in particular red complex bacteria (Porphyromonas gingivalis, Tannerella Forsythia, Treponema denticola), A. Actinimycetemcomitans, Prevotella intermedia. It is assumed that the microflora of the oral cavity at the time of implantation influences the formation of biofilm on the surface of the implant. Accordingly, existing periodontal pockets in the area of natural teeth serve as reservoirs of pathogenic microorganisms that can colonize installed implants.
Periodontal and peri-implant pockets at the same probing depth in the same patient have a similar microbiological composition. Thus, rationally, periodontal diseases must be pre-treated before implantation as part of a comprehensive periodontal therapy protocol.
Risk factors
Risk factors are of great importance for the occurrence of diseases around implants. Local factors include anatomical and clinical conditions that favor the colonization of pathogenic bacteria: for example, poor oral hygiene, deep gingival pockets, unfavorable denture design (Fig. 4).
Rice. 4. The patient undergoes a routine examination 1 year after total prosthetics. Hygiene is unsatisfactory, food remains, soft plaque. The gums are hyperemic and swollen both in the area of the teeth and in the area of the implants.
Rice. 4. The patient undergoes a routine examination 1 year after total prosthetics. Hygiene is unsatisfactory, food remains, soft plaque. The gums are hyperemic and swollen both in the area of the teeth and in the area of the implants.
General risk factors determine the response of the macroorganism to the microbial load - for example, the patient’s general health, bad habits. A combination of risk factors can lead to a severe response to inflammation resulting from bacterial infection, which will increase the rate of bone resorption in peri-implantitis.
Oral microflora colonizes the surfaces of implants and prosthetics in the same way as traditional fixed dentures, so good oral hygiene is critical to the long-term success of implant treatment. The accumulation of bacterial plaque on the gingival surface of the prosthesis leads to the development of mucositis, which is clinically manifested by redness, swelling of the mucous membrane and bleeding when probing the gingival sulcus. Lack of timely treatment leads to further progression of the inflammatory process and its spread to bone tissue (Fig. 5).
Rice. 5. Implants in the area of the 32nd, 42nd, 43rd teeth. Condition of the gums 2 months after permanent prosthetics. Unsatisfactory hygiene in the area of metal-ceramic prosthesis on implants. Bleeding on probing.
When planning implant treatment, one must take into account the need to create optimal conditions for self-hygiene in the implant area. It should be remembered that in the absence of proper care, peri-implantitis develops very quickly, even if the patient has no history of periodontitis.
Removing all teeth does not completely eliminate periodontal pathogenic bacteria, since they are able to penetrate soft tissues; also, if there are family members diagnosed with periodontitis, there is a constant supply of periodontopathogenic microflora from the outside (through hygiene items, dishes, kisses).
The integration of soft tissues to the intragingival elements of orthopedic structures is important. Titanium and ceramic abutments promote the formation of a mucosal attachment strip 1.5 mm wide. There is little or no attachment to gold and veneering ceramics, which increases the likelihood of developing deep pockets. In addition, there is better adhesion of soft tissues to relatively rough surfaces. However, when a rougher surface in the mouth is exposed, bacterial plaque accumulates on it more quickly. Thus, when choosing an implant system, the dentist faces a certain dilemma. On the one hand, it is necessary to achieve better attachment of soft tissues to the intragingival structures of the structure, and on the other, to avoid excessive accumulation of bacterial plaque when exposed in the oral cavity.
It is believed that excessive occlusal load can cause bone loss around implants. Many authors have studied the relationship between implant load and marginal bone resorption. Most of these studies have been conducted in animal models over a period of 12–15 years. It turned out that the load on the implants is not accompanied by bone resorption around them. On the contrary, the degree of mineralization of the bone in direct contact with the implant increases compared to an implant that does not experience such stress. Thus, excessive loading of implants in the long term can lead solely to biomechanical damage (screw loosening, crown decementation, abutment fracture, implant fracture), and bone resorption around integrated implants is associated only with bacterial infection.
Cigarette smoking should be considered as a potential risk factor, since tobacco smoke directly affects local immunity in the oral cavity. There is a decrease in chemotaxis and phagocytosis of neutrophils, stimulation of anti-inflammatory cytokines, activation of subgingival anaerobes, all of which can cause early and late complications after implant installation.
The professionalism, theoretical knowledge and manual skills of the doctor play a big role in the success of implant treatment. Unfortunately, due to the popularization of implantation, doctors have formed the opinion that installing implants is a fairly simple manipulation that does not require much theoretical knowledge and manual skills. According to recent studies in the field of peri-implantitis, in more than 90% of cases, this disease is caused by poor planning and suboptimal treatment.
Biotype of gingival tissue
When lengthening the coronal part, it is important to take into account the biotype of the gum. According to research results, the gingival margin can “grow” along the crown from the level determined during the procedure. This growth is more often observed in patients with a thick biotype of gingival tissue, but there are also individual characteristics. In addition, it is likely that the amount of gingival retraction depends on the position of the flap relative to the alveolar ridge at suturing, as described by Deas (2004). Therefore, if the patient has gum tissue of a thick biotype, it is possible to compensate in advance for the mentioned reverse movement of the edge during the formation of the gum during the operation. A temporary crown should be placed 6-8 weeks after surgery to ensure proper gum formation before the permanent crown is placed.
Pathogenesis
Direct contact between the accumulation of microorganisms and the soft tissues surrounding the implant leads to inflammation and an increase in probing depth, similar to the processes occurring in the area of natural teeth. Experimental studies confirm a similar inflammatory response around teeth and implants in response to bacterial irritants. In both cases, the lesion is localized in the area of the gum edge. The progression of the inflammatory process and tissue infiltration by large lymphocytes leads to bone resorption. Elastase-producing cells are found in greater numbers in peri-implantitis than in periodontitis, indicating a more rapid progression of peri-implant bone damage.
As plaque accumulates, the tissue damage around the implant spreads in the apical direction. The inflammatory infiltrate includes plasma cells, macrophages, lymphocytes and a large number of polymorphonuclear leukocytes. Moreover, it is the increase in the number of polymorphonuclear leukocytes that may explain the increase in elastase concentration in peri-implantitis compared to periodontitis. The inflammatory infiltrate during peri-implantitis directly extends to the alveolar bone and penetrates into the medullary spaces. This circumstance distinguishes the nature of inflammation in peri-implantitis, since in periodontitis the inflammatory infiltrate is separated from the bone tissue by a dense connective layer about 1 mm thick. In peri-implantitis and periodontitis, cytokines are found that increase the activity of osteoclasts, however, in peri-implantitis, interleukin-1A predominates, while in periodontitis, tumor necrotizing factor alpha has a greater influence. The absence of a periodontal gap and ligament in the implant is important in the pathogenesis of the development of the process. The tooth has excellent blood supply and strong immunity; therefore, the body is able to resist infection and periodontitis lasts for years - from the moment a subgingival infection occurs until the complete loss of the tissues surrounding the tooth, it can take 15–20 years. For an implant, due to the differences in structure and pathogenesis described above, complete disintegration can occur within 3–5 years from the onset of peri-implantitis (Fig. 6).
Rice. 6 a. Level of bone tissue at the time of permanent fixation.
Rice. 6 b. The patient has no complaints. A routine examination with X-ray control 2 years after fixation revealed a saucer-shaped loss of bone tissue.
Crown lengthening techniques[edit]
Apically repositioned flap with bone recontouring (resection) [13][edit]
The apically repositioned flap is a commonly used procedure that involves lifting the flap and then contouring the bone. The flap is designed in such a way that it is replaced more apically relative to its original position, thereby achieving immediate exposure of healthy tooth structure. As discussed above, preservation of biological width must be considered when planning a crown lengthening procedure.
Typically, at least 4 mm of healthy tooth structure must be exposed during surgery. This thus promotes the proliferation of supragingival soft tissue, which is estimated to cover 2–3 mm of the coronal root structure, thus leaving 1–2 mm of supragingival healthy tooth structure. In addition, the innate tendency of the gingival tissue to overcome abrupt changes in the contour of the bone ridge must be considered. In this regard, it is recommended to carry out bone reconstruction not only around the problem tooth, but also on neighboring teeth in order to gradually reduce the bone profile.
Therefore, when crown lengthening using an apical flap, a significant number of attachments may have to be sacrificed. It is also important to remember that for aesthetic reasons it is necessary to maintain tooth length symmetry between the right and left sides of the dental arch. In some cases, this may require including even more teeth in the surgical procedure. [14]
Indications [edit]
Lengthening the crown of several teeth in a quadrant or sextant of the dentition
Contraindications [edit]
Single teeth in the aesthetic zone are becoming increasingly destructive.
Technique [13] [edit]
- The reverse incision is made with a scalpel. This initial incision is made during preoperative planning and depends on the amount of tooth structure that needs to be exposed. The beveled incision should also have a serrated contour to ensure maximum interproximal alveolar bone coverage during subsequent flap advancement. Vertical release incisions extending into the alveolar mucosa, beyond the mucogingival junction, are made at each endpoint of the reverse incision, allowing repositioning of the flap at the apex.
- The full thickness mucoperiosteal flap is then elevated to expose the root surfaces. The flap, including the buccal/lingual gingiva and alveolar mucosa, should then be elevated above the mucogingival line to subsequently be able to reposition the soft tissue apically. The marginal collar of tissue is then removed using curettes.
- The bone tissue is then recontoured using a rotating round bur and a generous spray of water or bone chisels. Recontouring should aim to recreate the normal shape of the alveolar ridge, but at a more apical level.
- After bone surgery, the flap is moved to the level of the newly reconstructed alveolar bone crest and fixed in this position. Complete soft tissue coverage is inherently more difficult and therefore a periodontal dressing should be applied to protect the exposed interdental alveolar bone to keep the soft tissue level with the bone crest.
Benefits[edit]
Immediate improvements in healthy tooth structure can be achieved.
Disadvantages [edit]
Difficult procedure for patients, increased postoperative pain [14]
Forced teething [13] [edit]
Orthodontic tooth movement can be used for teething in adults. If moderate eruption forces are applied, the entire eruption apparatus will move in unison with the tooth. Thus, the required elements must be extruded to a distance equal to or slightly greater than the portion of healthy tooth structure that will be exposed during subsequent surgical treatment. Once stabilized, the full thickness flap is elevated and bone recontouring is performed to expose the desired tooth structure. To properly restore aesthetic proportions, the hard and soft tissues of adjacent teeth must remain unchanged.
Indications [edit]
Forced tooth eruption is indicated where crown lengthening is required, but attachment and bone from adjacent teeth must be preserved.
Contraindications [edit]
Forced teething requires a fixed orthodontic appliance. This creates problems for patients with reduced dentition; in such cases, alternative crown lengthening procedures should be considered.
Technique [13] [edit]
Orthodontic braces are attached to the teeth that require crown lengthening surgery and then to the adjacent teeth, which are then combined into an arch. Then a power elastic band is attached from the bracket to the arch (or beam), which pulls the tooth coronally. The direction of tooth movement must be carefully checked to ensure that there is no tilting or movement of adjacent teeth.
Forced teething can also be performed using fibrotomy. This method is used when it is necessary to maintain the gum margins and crystalline bone height in the places where they were before treatment. During treatment, fiberotomy is performed at intervals of 7-10 days. Using a scalpel, the supracrestal fibers of the connective tissue are cut, thereby preventing the crystalline bone from following the root in a coronal direction.
Benefits[edit]
Preserves bone structure around adjacent teeth
Disadvantages [edit]
The procedure requires a fixed placement of wires. The treatment time can be extended.