A core inlay is a special dental structure that is made using an impression and then acts as a support for the installation of an artificial crown. Dental prosthetics with inlays is carried out in cases where there is severe tooth decay.
This design consists of two parts: root and crown. The first is installed in the tooth root canal, and the second is a tooth stump, fully prepared for the installation of a crown. Unlike a pin, a stump tab is installed in several stages. At the same time, this technique ensures that the tooth will not break and will no longer be susceptible to decay. The design ensures uniform distribution of the chewing load - this is one of its most important advantages.
The tightness of the structure is due to its fixation using a special composition. It fits tightly to the remaining tooth and eliminates the possibility of cracks. The choice of material depends on many factors. Stump inlays made of zirconium dioxide are in wide demand today - given its properties, this is not surprising.
General information about designs
Zirconium dioxide inlay - what is it? You need to understand that inlays in dentistry belong to the field of prosthetics, or more precisely, microprosthetics. That is, these are small-sized prostheses, which come in 2 types:
- restorative (or coronal): independently restore the integrity of the tooth,
- stump (or pin): serve as a support for another prosthesis - a crown, bridge, removable orthopedic structure.
Both restorative and pin inlays are made from zirconium oxide1 - we will describe below what each of these zirconium inlays is and what it looks like. It is worth noting that zirconium dioxide is a very strong material in compression and bending (more than 1400 MPa), in this it can even be compared with metal alloys. However, zirconium dioxide is more often called ceramics - more precisely, metal-free ceramics, since purely externally the material is white, like your own teeth.
%akc72%
Restorative microprostheses - features and advantages
Restorative inlays made of zirconium dioxide are small-sized microprostheses. They are fixed on a natural dental crown, provided that it is destroyed by no more than 50%. You can compare restorative ones with fillings (only very strong ones). Because both are installed in a dental cavity cleared of caries and restore the integrity of the tooth. However, if the filling is formed directly in the tooth during 1 visit to the clinic, then the microprosthesis is made only in the laboratory using impressions (casts) taken in advance.
In most cases, restorative ones are installed on the chewing surfaces of the teeth in the lateral sections of the row - on premolars (“fours” and “fives”) and molars (“sixes”, “sevens”, less often - on “eights”, i.e. wisdom teeth) . In size, microprostheses can be small - inlay, or almost completely cover the top of the crown along with chewing tubercles or cutting edges - onlay, overlay, pinlay varieties.
Features of stump microprostheses
A stump or pin inlay, unlike a restorative one, is not an independent prosthesis. But it is used as a kind of microprosthesis, which is installed in the tooth under a crown or bridge. In essence, the stump is a support, and a very reliable one. The upper part of the stump is an analogue of a ground natural crown, and the lower part is analogous to miniature roots that are inserted into the root canals of the tooth.
Stump microprostheses can be one-piece or dismountable. Solid ones are installed in teeth with 1-2 roots, and collapsible ones are installed in teeth with 3 or more roots. After all, the canals in the roots diverge at different angles, and inserting a solid tab on three or four supports simply won’t work. If we consider single-channel and multi-channel tabs, then single-channel ones are always solid, and multi-channel ones can be either solid (for 2 channels) or collapsible (for 3 or more channels).
A prerequisite for prosthetics is if your own crown is destroyed by 70% or more, if only 1 wall is preserved, if the crown is completely broken at the root. But with all this, the roots must be healthy and intact. Stump zirconium inlays are placed on both the front and chewing teeth.
What is a core inlay for a crown?
A stump inlay is an orthopedic structure that serves as a support for installing an artificial crown on a severely damaged tooth. This prosthetic element is also called a pin stump inlay, since its root part resembles a dental pin. It is inserted into the dental root canal, and a crown is placed directly on the coronal tip of the inlay, similar to the stump of the prepared tooth. The post-stump inlay should not be confused with a regular dental inlay, which is used as an alternative to fillings.
Advantages of using stump tabs
- The core inlay is made according to individual impressions of the patient and completely reproduces the space of the canals of the tooth to be restored with a crown.
- The stump inlay also has an upper part - in the shape of a tooth ground for a crown. This structure of the microprosthesis ensures uniform load distribution even under strong pressure while chewing food.
- The core tab may have several pins to restore a multi-rooted tooth.
Advantages of microprostheses made of zirconium dioxide
If the question arises, which is better - a zirconium restoration inlay or a filling, then the first has the following advantages:
- more reliable: it is made of the strongest zirconium dioxide, and the filling is made of liquid composite or cement. In the future, these factors seriously affect the service life,
- more durable: a microprosthesis made of zirconium dioxide can last more than 20 years, and a large filling - on average 3-5 years, maximum about 7 years,
- tighter fit to the walls of the cavity: the microprosthesis is created in the laboratory using special equipment, and in exact accordance with the dimensions of the cavity - therefore it adjoins it without gaps. And over time, the tab, unlike a filling, does not peel off from the walls,
- does not wear off or sag during use: let us remind you that the material is extremely durable, which cannot be said about the filling - it begins to wear out and sag within a year after installation.
There are 2 moments when the filling wins. The first is if the cavity is very small, i.e. the microprosthesis will not be qualitatively fixed in it. The second is the front teeth, since they have a very thin cutting edge instead of an extensive chewing surface (like premolars and molars). More often, front teeth with small defects are restored with fillings or veneers - they, by the way, can also be made of zirconium dioxide. Restorative (pinlay varieties) in some cases can be placed on the lingual surface of an incisor or canine.
Patients often ask which inlays are better – fiberglass or zirconium? You need to understand that the fiberglass pin is not a tab, but a thin rod (just like a metal pin). Let's see what important advantages zirconium dioxide core inlays have over conventional pins:
- made individually for the patient, so they fit tightly to the root canals,
- very durable: while fiberglass pins are less durable, metal pins are thinner, so they often break,
- do not shine through the prosthesis: because are white in color, and the metal pin is visible through the filling material,
- qualitatively transfer the load to the root and jaw bone due to the anatomical shape of the microprosthesis,
- serve for about 15-10 years: and the maximum service life of a conventional pin is 5 years, because it leads to overload and destruction of the tooth root.
Installation of a core inlay on a front tooth
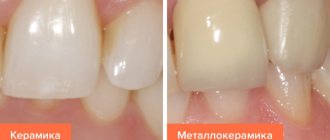
When a large part of the tooth is broken off or a carious process that can completely destroy the crown part, various types of dental inlays are used. An individually made crown from selected material is installed on the microprosthesis, which exactly replicates the color and shape of natural front teeth (zirconium, ceramics, metal-ceramics).
Dental inlays can be made for orthopedic treatment when one or more front teeth are destroyed. In case of a very extensive defect in the area of the anterior dentition, caused by aggressive (decompensated) caries or trauma, it is worth prosthetic restoration with a bridge structure, which can be supported well by two dental inlays for a crown. Quite often there are incisors or canines of irregular shape or size. These deformities can also be corrected by placing a microprosthesis made using ceramic material or zirconium oxide. If the position is incorrect due to the rotation of one of the teeth around its axis, inlay prosthetics can serve as an alternative to longer orthodontic treatment.
What is known about the shortcomings
According to reviews from some patients, a zirconium inlay (restorative or stump) has only one drawback - its high cost. Another disadvantage is the time spent on prosthetics - it takes about 2 weeks to complete the treatment. Although, for example, CEREC technology allows you to make a restorative microprosthesis in 15-20 minutes - and it will be installed on the day you go to the clinic. However, such equipment is not available everywhere.
Read on the topic: what is CEREC technology - when does the dentist and patient need it, its pros and cons.
Another disadvantage is the pure white color of zirconium dioxide (several shades lighter than natural enamel) and its opacity. But dental technicians solve this problem by applying liquid ceramic, colored in the shade of enamel, to the upper part of the zirconium restorative microprosthesis. Or you can use alternative prosthetic options (more on them below).
How to fix zirconium: APC concept
Some of the new materials introduced recently have had a huge impact on the development of the entire clinical dentistry, greatly helping to improve existing restorative treatment concepts.
Ceramics based on zirconium dioxide (ZrO2), in turn, have significantly expanded the possibilities of using all-ceramic restorations both in cases of restoration of single teeth and in the course of total rehabilitation of dental patients supported by implants. The first zirconia coping produced by CAD/CAM technology (although it would be more accurate to call it yttrium-stabilized zirconia or yttrium-stabilized zirconia tetragonal polycrystalline [Y-TZP] coping) was introduced in the late 1990s, thus marking , a new era of aesthetic rehabilitation with zirconia-ceramic restorations (PFZ).
First, Nobel Procera Zirconia (Nobel Biocare) material appeared on the market and a little later in the 2000s, LavaTM Zirconia (3M ESPE). The demand for zirconium-ceramic restorations increased due to their unique highly aesthetic characteristics, as well as due to the high bending strength of zirconium, the parameter of which reached more than 1000 MPa. Early studies of new restorations, however, often reported high rates of chipping and fracture of the veneering material, especially in veneer cases. As a result of subsequent improvements in the physical properties of the material, zirconium-ceramic structures were improved so much that the long-term performance of their use was almost no different from that of metal-ceramic crowns.
However, given that there were still some concerns about ceramic chipping, and the sintering process was very, very sensitive, monolithic all-zirconium restorations produced by CAD/CAM milling became extremely popular as an alternative. It is logical that in the manufacture of such, the need to use facing ceramics simply disappears.
The advantages of all-zirconium crowns are the cost-effectiveness and speed of manufacturing these structures compared to multilayer indirect restorations; in addition, the transparency parameters of second-generation zirconium materials have apparently improved compared to the first, without compromising the flexural strength indicators. However, to achieve individual shades, at the green stage of milling or before sintering, a liquid dye must be applied to the workpieces, and after sintering, the external coloring of the structure must also be provided. To simplify this process, some manufacturers have developed pre-colored zirconia blanks in a variety of shades, some of which have separate shade parameters for enamel and dentin, helping them better mimic the appearance of natural teeth. However, even multilayer zirconia restorations can be color modified to provide an external color or a similar result can be achieved by polishing to the desired level of gloss.
The latest generation of zirconium materials is characterized by a significantly greater degree of translucency, providing improved aesthetics of restorations, which is extremely important for the prosthetic rehabilitation of the anterior areas of the teeth. The increased degree of translucency of the materials is achieved through small changes in yttrium (Y2O3) in the composition of the preform (5 mol% or more instead of the usual 3 mol%), which is essentially used to stabilize the tetragonal phase of zirconia, resulting in the formation of more particles in cubic phase. Cubic zirconium provides significantly greater light transmission of the material, but at the same time reduces its physical resistance. The bending strength of highly transparent workpieces ranges from 550-800 MPa, depending on the degree of translucency: the higher the translucency parameter, the lower the bending strength. But despite some problematic aspects, the specific properties of zirconia make it a reliable and promising alternative for use in the practice of aesthetic dentistry, especially in the manufacture of veneers and onlays, provided an adequate bonding protocol is ensured.
Bonding ceramics
Ceramic materials are brittle and cannot undergo plastic deformation, which is characteristic of metal alloys. Thus, their elastic modulus and functional stress behavior differs from metals: the crystalline structure compromises crack propagation when the outer surface is damaged and excess loads are applied. Thus, the type of luting agent, as well as the luting technique itself, significantly influences the clinical success of all-ceramic restorations. Adequate treatment of the supporting tooth stump, as well as sufficient bonding strength of the composite material, promote retention of ceramic restorations, reduce the risk of microleakage, and also increase the parameters of their resistance to possible destruction during operation. Clinical procedures and pretreatment steps for material and tooth surfaces differ depending on the composition and mechanical properties of the ceramic substrate. The two main types of ceramic materials remain those based on silica (i.e., feldspathic, leucite and lithium disilicate ceramics), as well as those without the presence of silica in their structure. The latter include materials based on aluminum oxide and zirconium oxide. The quality and durability of the bond between the composite and the ceramic surface remains a key aspect to ensure the clinical success of such restorations. These, in turn, depend on the surface topography of the ceramic base and its chemical interaction with the composite cement. As with any other adhesive bond, contamination at the material interface will negatively impact the long-term performance of esthetic crowns. To treat the glassy matrix of ceramics, it is recommended to use hydrofluoric acid and a binding agent - silane. The first component selectively dissolves the glass matrix and allows the formation of a porous, uneven ceramic surface with an increased wettability parameter. The use of silane after etching helps to increase adhesion through improved mechanical adhesion and the formation of silicon compounds (silicon oxides) in the structure of the organic matrix of polymer materials through siloxane bonds. It is not advisable to treat the inner surface of silicon-based ceramics using surface abrasive methods, such as air abrasion or grinding, since such approaches can provoke the occurrence of microcracks, which subsequently lead to fractures of the ceramic structure.
High-strength metal oxide ceramics such as alumina and zirconia are generally only considered “cementable” due to their high flexural strength, which exceeds typical masticatory loads. Thus, crowns and bridge structures with adequate retention parameters and the required thickness of ceramic material can be fixed in the most conventional way. It is optimal for such purposes to use resin-modified glass ionomer cement or its self-adhesive analogue, since approaches using these materials are both the least time-consuming and optimally accessible. In this case, you should strictly follow the manufacturer’s instructions, since some of them require air-abrasive treatment of the ceramic surface, while others, on the contrary, do not recommend it. Some self-adhesive cements must first be spot-exposed, then proceed to remove excess material, and only then carry out final polymerization. It is also important to remember that before bonding, each indirect restoration should be cleaned in an ultrasonic bath using ethanol or acetone.
APC concept for zirconium bonding
So-called “cemented” zirconium restorations are characterized by a number of problematic aspects, including insufficiently reliable structural strength, problems with adhesion to the composite, and lack of sufficient retention. All this makes the doctor think about what is better to choose in certain situations: solid crown designs or vestibular veneers. The success of bonding restorations depends on the adequacy of the choice of the required material, the necessary processing of the tooth stump and the inner surface of the restoration. Tooth surface treatment should be carried out strictly according to the manufacturer's protocol and only with the use of dentin bonding agents, since most self-etching bonds form too thick a film during photopolymerization. Research into the bond quality between composites and ceramics has been conducted over the past two decades. Classic articles by Kern and colleagues demonstrate that for high-strength ceramics, most of the available bonding protocols provide treatment success only in the short term, while long-term results can only be achieved through preliminary air-abrasive treatment followed by the use of composite cement, which must contain special phosphate agents. monomers like 10-methacryloyloxydecyl dihydrogen phosphate (MDP monomer). Some of the known composite cements have been developed specifically to provide adhesion to the metal coping of the restoration. The first studies on the issue of bonding to aluminum and zirconium began in the 2000s, and included the testing of thousands of known materials along with various protocols for treating the surface of abutment teeth. Unlike other studies that used polished ceramic specimens, we analyzed the actual internal surfaces of CAD/CAM ceramic restorations and found that the use of phosphate monomers, such as MDP, in addition to composite cement helps to significantly improve bond strength and thus , achieve almost similar efficiency parameters for air-abrasive processing of high-strength ceramics. Other methods of processing structures such as acid etching and plasma spraying have also proven promising, but their use in everyday clinical practice is very, very limited.
In order to practically achieve a high-strength and durable connection of composite cement with zirconium, we recommend using the following three-stage algorithm, which for simplicity we call the “APC concept”: stage A (air particle) – air-abrasive surface treatment with aluminum oxide; stage P (primer) – stage of applying a special primer; Stage C (composite resin) - use of self-adhesive or dual-cure cement.
Stage A
After cleaning the restoration, the zirconia is treated by air abrasion using alumina powder or silica-coated alumina particles. Some authors call this procedure sandblasting or micro-etching. It is effective to use particles ranging in size from 50 microns to 60 microns at low pressures of up to 2 bar. The effect of this treatment is very important, since it simultaneously allows decontamination of the surface of the restoration. The results of this approach are widely highlighted in the literature and the use of smaller particles ultimately only allows for strengthening the structure without compromising its integrity in any way.
Stage P
This step involves the use of a special ceramic primer, which usually contains special adhesive phosphate monomers. The primer is applied to the surface of the zirconia. MDP monomer, which is also used in some dentin adhesives and some resin cements, has been shown to provide a more highly effective bond to metal oxides. In addition, such primers can also enhance the bonding abilities of other cements, such as glass ionomer-modified composites. An important aspect remains the need to use different materials from the same manufacturer, avoiding the use of cements and primers of different brands, which, most likely, also have different chemical compositions and, therefore, may be incompatible with each other. Some confusion arises when using special zirconia primers that contain silanes, which makes the latter universal materials applicable to various materials, including silica-based ceramics. In such cases, the main thing to remember is that these materials provide a long-term bond with metal-based ceramics only if they contain silica particles, or particles containing this chemical base.
Stage C
Self-curing or dual-curing cements are used to ensure an adequate level of material conversion under zirconia restorations that limit light exposure. But, on the other hand, the transparency of the zirconium structure is such that the shade of the cement fixing the crown still significantly influences the final aesthetic appearance of the restoration. Therefore, before final cementation, it is recommended to use special try-in pastes, which will help you choose the optimal shade of the fixing material. The APC concept is not limited only to the peculiarities of fixing zirconium structures on natural teeth, but can also be used in a dental laboratory for fixing supraelements supported on implants. For new products containing high levels of translucent zirconia with low flexural strength, the aspect of adequate bonding is even more critical because the thickness of such structures is significantly less than their standard counterparts. Veneers, inlays, onlays or prostheses can only guarantee long-term functioning when the stage of their adhesive fixation was carried out strictly according to the protocol. The concept proposed by APC is not new, but is the result of twenty years of practice and testing of different adhesion protocols. The conclusions drawn from existing systematic reviews of the literature, which analyzed data from 140 different studies, are similar to those obtained at the end of this article, but the further search for methods to optimize the adhesion stage of zirconium restorations remains one of the most pressing tasks of modern dentistry.
Clinical case
A 40-year-old patient sought dental care with the chief complaint of cracked teeth and a desire to restore his previous habitual bite. During the dental examination, class I occlusal relationships and a slight discrepancy between teeth 8 and 9 were recorded. The patient also had a widespread form of pathological abrasion and class I mobility in the area of teeth 23-26. Carious lesions were found in the area of teeth 2, 4, 6, 8, 9 and 14, and wedge defects were found in the area of 4, 5, 10, 11, 13, 20 and 21. Photos 1-3 illustrate the clinical situation of the patient before treatment .
Photo 1. View of the patient’s smile: a compromising aesthetic situation.
Photo 2. Front view with maximum teeth closure before treatment.
Photo 3. View of the upper jaw before treatment.
As a treatment, the patient was offered a total rehabilitation protocol. The purpose of the complex intervention was to correct the erosive etiology of the lesions and protect the hard tissues of the tooth with the help of long-term restorations. The diagnostic wax-up guide was instrumental in determining functional and aesthetic treatment goals and shaping the anterior insertion path (Figure 4).
Photo 4. Diagnostic wax reproduction.
After periodontal treatment, restoration of carious defects and the use of provisional restorations, the doctor began the final preparation of the front teeth (photo 5) with their subsequent restoration.
Photo 5. Preparation of the upper anterior teeth to control the vertical parameters of occlusion.
CAD/CAM all-zirconium structures with a high degree of transparency (Katana UTML Ultra Translucent Multi-Layered, Kuraray Noritake Dental) were used as crowns (photos 6 - 7), which were cemented with self-adhesive composite cement (Panavia S.A., Kuraray Noritake Dental) .
Photo 6. CAD/CAM design of all-zirconium crowns in the area of the anterior teeth.
Photo 7. View of monolithic zirconium crowns on the model.
Photo 8 shows the situation after cementation of the anterior structures and gentle preparation of the posterior tooth area. For the distal supports, highly esthetic monolithic zirconium crowns and onlays were fabricated (Katana Zirconia UT, Kuraray Noritake Dental, photos 9-12).
Photo 8. Occlusal view of fixed zirconium crowns in the area of the anterior teeth. Conservative preparation of distal teeth for crowns and onlays.
Photo 9. Occlusal view of zirconium restorations in the posterior teeth.
Photo 10. View of the right zirconium restorations from the lingual side on the model.
Photo 11. View of the left zirconium restorations from the lingual side on the model.
Photo 12. Monolithic zirconium onlays and crowns.
Restorations in the area of distal teeth were fixed according to the protocol of the APC concept. First, the structures were sandblasted with 50 µm aluminum oxide particles at a pressure of 1.5 bar (photo 13), after which a special ceramic primer (ClearfilTM Ceramic Primer, Kuraray Noritake) with adhesive phosphate monomer (MDP) was applied (photo 14).
Photo 13. ARS concept: stage A - air-abrasive treatment with aluminum oxide particles of 50 microns at a pressure of 1.5 bar.
Photo 14. APC concept: P stage - application of a primer with active phosphate monomers.
Isolation of the working field was carried out using cotton rolls and retraction thread, since the use of a rubber dam was difficult in this clinical situation. The enamel of the abutment teeth was selectively etched (Figure 15) using 35% phosphoric acid (K-Etchant Gel, Kuraray Noritake Dental), and the dentin was conditioned using (Figure 16) a self-etching dentin primer (Panavia V5 Tooth Primer, Kuraray Noritake Dental). Dual-curing composite cement (Panavia V5 Paste Universal, Kuraray Noritake Dental) was dispensed directly onto the restoration using a special syringe mixer.
Photo 15. Selective etching of the enamel of abutment teeth with phosphoric acid for 20 seconds.
Photo 16. Application of self-etching dentin primer.
After planting the structures, excess cement was removed (photos 17 - 18), and only after that complete polymerization was carried out (photo 19). The appearance of the teeth after the end of treatment is shown in photos 20-22.
Photo 17. APC concept: Stage C - application of dual polymerization composite cement. Installation of restoration and removal of excess cement.
Photo 18. Removal of excess cement from the proximal sides.
Photo 19. Polymerization of the material for 60 seconds on each side.
Photo 20. Occlusal view of restorations on the upper jaw.
Photo 21. View of restorations in a state of maximum closure of teeth.
Photo 22. View of the patient’s smile after treatment.
conclusions
Reliable cementation protocols, as well as the materials used for them, are the basis for achieving long-term clinical success of indirect ceramic restorations, including those based on zirconia. The latter, thanks to their optical properties, provide the most adequate aesthetic result of treatment in both the anterior and chewing teeth. Composite adhesion ensures retention of ceramic onlays, veneers and even dentures, and the systematic APC protocol, based on many years of research, helps achieve excellent long-term results of fixation of zirconia structures with composite cement. The algorithm consists of three simple steps: (A) - air abrasive treatment, (P) - application of zirconium primer and (C) - use of composite cement.
Authors: Markus B. Blatz, DMD, PhD Marcela Alvarez, DDS, MSD Kimiyo Sawyer, RDT Marco Brindis, DDS
Indications for prosthetics
Restorative and core microprostheses made of zirconium dioxide are indicated for installation in adult patients, less often - in adolescents with permanent teeth (such prosthetics are not performed on dairy patients). Let's look at the readings in more detail in the table below.
| Factor | Restorative microprostheses | Stump microprostheses |
| Installation location | On a natural crown | To the root canals |
| Initial preservation of the natural crown | 50% or more | Less than 70% or complete destruction to the root |
| Root condition | Healthy, no cracks, cysts or granulomas | |
| Presence of dental nerve (pulp) | As a rule, the pulp should be healthy | Subject to mandatory removal, root canals are filled |
| What teeth are they placed on? | Mainly for chewing | Stump inlays can be placed under chewing and front teeth |
| Fixing another prosthesis on top | Not required | Mandatory |
When choosing a core microprosthesis made of zirconium dioxide and the patient wants to put a ceramic crown on the front teeth, the dentist can tell you why zirconium inlays are dangerous in this case. The aesthetics of the restoration will certainly be high. But the fragile ceramics of the crown will quickly become unusable - it will simply crack on a strong support. Therefore, it is better to give preference to a zirconium crown.
Don't know what type of prosthetics to choose?
We will help in the selection, advise where to read more information and compare types of prosthetics.
Consultation with an orthopedic doctor in Moscow clinics is free! Call now or request a call
Working hours: from 9:00 to 21:00 - seven days a week
Pros and cons of stump inlays
A significant advantage of these microprostheses is their high reliability and preservation of the anatomical structure of the tooth. The root is intact, so the dental unit receives full load when chewing. This means that the bone tissue of the jaw does not degrade, and normal bite and diction are maintained.
The installation procedure is minimally invasive and usually easy to tolerate.
Contraindications for installation
A contraindication to fixation of a restorative microprosthesis is extensive destruction of the natural crown. If, for example, more than half of it is missing due to caries or injury, or there is a very large cavity inside, surrounded by thin walls.
“I had a zirconium core inlay and the same crown made by my dentist. Probably 6 years have passed, but the tooth feels great and looks like a real one. Before this, I constantly had to change the filling - but in chewing ones, the fillings are large and not very beautiful, they fail over time.” Tatyana P., review from the woman.ru forum
It is contraindicated to install a stump if the dental nerve is preserved, if there are cracks in the root or if a pin/instrument fragment is stuck. Also considered a contraindication is the presence of inflammatory processes under the roots, formations (granulomas, cysts). It is also not recommended to install core microprostheses on teeth with pronounced mobility.
Making a core inlay for a crown
For the manufacture of stump pin inlays, direct and indirect methods are used. The direct method of manufacturing a stump insert has the following steps.
- After preliminary treatment of the tooth canals and its preparation for the stump inlay, the cavity is treated with Vaseline.
- The plastic, heated to a viscous state, is poured into a syringe and squeezed into the cavity through a wide needle to form an inlay.
- The pin is processed with the same material and inserted into the canal.
- After the plastic structure has hardened, the finished model of the inlay is removed from the cavity and sent to a dental laboratory for the manufacture of a microprosthesis from the material chosen by the patient.
The indirect method includes the following stages of manufacturing a stump inlay:
- After preliminary preparation of the tooth and canals, the doctor takes an impression and transfers it to the dental laboratory.
- The technician casts a plaster model and creates a prototype of the inlay from wax.
- Based on the wax sample, a metal stump inlay is made.
If we talk about stump inlays made of zirconium or ceramics, then CAD/CAM technologies are used for their production, which involve computer modeling of a microprosthesis, transferring the model to a milling machine and subsequent “cutting out” of the inlay from the workpiece.
How are dentures made and installed?
The processes of preparation for prosthetics, creation of a zirconium dioxide microprosthesis and its fixation consist of the following stages:
- Stage 1 – diagnosis: also at this stage, contraindications are excluded, the condition of the tooth itself, as well as neighboring and opposite ones, is studied,
- Stage 2 – preparation: the dentist-therapist removes all carious tissues, if necessary, depulps the tooth and fills the root canals, leaves a cavity for a classic restorative inlay or forms it inside the roots,
- Stage 3 – taking impressions (impressions): for example, using wax or silicone (this depends on the type of future prosthesis), the color of the restoration is selected. In clinics with modern equipment, digital impressions of the oral cavity can be made using an intraoral 3D scanner - this is fast, convenient and very accurate,
- Stage 4 – modeling: a real model of the prosthesis is created based on impressions in a dental laboratory, and a virtual model is created in a computer program based on digital impressions. But the real model will also need to be digitized and worked out in a CAD/CAM system for the next stage,
- Stage 5 – manufacturing: production occurs by milling on a machine, because the material is so strong that it will not be possible to create a prosthesis by hand. Usually the workpiece is made 20-25% larger than the actual size, because After milling, it is baked - in this case, the material “shrinks” to the required parameters. If necessary, the microprosthesis is covered with a layer of colored ceramics. Next, the product is sent to an orthopedic dentist,
- Stage 6 – fixation of the zirconium inlay into the patient’s tooth.
Why core inlays are better than fillings and pins
Fillings and pins are only applicable if the tooth has a sufficient amount of healthy tissue. If only the root or thin walls of the tooth remain, it will not be possible to restore it with a pin, since this restoration method will not differ in either quality or reliability.
Firstly, under load, the pin can break and damage the tooth root. Trauma to the root of a tooth is a direct indication for its removal; In case of damage to the root system, no technique will help save the tooth.
Secondly, dentures installed on large fillings and pins are more likely to fall out some time after prosthetics. In this case, the treatment will have to be repeated, and this entails new significant financial costs.
Important: Some dentists try to cement a fallen crown and post using cement. But this is useless - the structure will not hold firmly and, moreover, an inflammatory process can begin under it, which leads to caries.
Therefore, in the case of severe caries, only an abutment inlay can provide high-quality and durable prosthetic results.
Service life and care features
The service life of zirconium dioxide is very long - 15, 20 and even 25 years. Such long-term operation will depend both on the quality of preparation of the tooth for prosthetics and the accuracy of the fit of the orthopedic structure, as well as on compliance with the rules of wearing and caring for prostheses. What is needed for this? Do not forget about regular brushing of your teeth in the morning and evening, avoid hard and stretchy products (so that the denture does not come off). Ideally, you should also visit your podiatrist twice a year for a checkup.
Cost of prosthetics in Moscow and other cities
How much does a zirconium inlay cost? Its price is 18-20 thousand rubles. Moreover, prices in the capital and other cities are approximately equivalent, because the basis is the cost of the material (which is purchased from the same manufacturers or suppliers).
1Zinovenko O.G., Shinkevich M.V., Sadovskaya I.V. Aesthetic prosthetics using zirconium dioxide, 2014.
Author: Sambuev B. S. (Thank you for your help in writing the article and the information provided)