Materials Manufacturing of removable dentures Manufacturing of fixed dentures Service life
The absence of teeth affects not only the function of chewing and speech, but also the emotional state, socialization and self-esteem. Prosthetics restores physiological functions, equalizes the emotional background, and increases self-confidence.
Making dentures is the result of a joint effort between a dentist and a technician. Each stage of work affects the final result. The manufacturing process depends on the type of structure and materials used.
There are the following types of restorations for restoring the dentition:
- Removable
. They are divided into full and partial. Full ones are used for edentia, when there are no teeth left at all. Partially removable ones are attached to the remaining teeth, which serve as support. - Fixed
. Unlike removable structures, inlays, crowns and bridges are fixed in the mouth for the entire period of use. They are removed only to replace them with new ones. - Conditionally removable
. Such dentures can be removed, but under certain conditions. The removable jaw is fixed on implants. You will not be able to remove the restoration yourself. The dentist will do this without difficulty, and after the necessary procedures, he will put it back.
Materials for the manufacture of prostheses
For permanent restorations, metals, ceramics and zirconium dioxide are used. Metal-ceramic crowns consist of 2 layers: a metal base, which is lined with a ceramic composition. Thick double walls require strong turning. Zirconium crowns are very durable, so the teeth need to be prepared minimally for them. New ceramic compositions, such as E-max, are quite durable and at the same time make it possible to choose the color of teeth of any shade.
The same materials can be used for conditionally removable prosthetics.
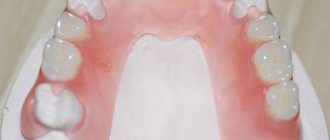
For removable dentures, the most important element is the base. The base is made from:
- Acrylic
- Acry Free
- Nylon
The hardest material is acrylic. Its disadvantages are microporosity and rapid wear. Acrylic contains substances that cause allergies. Pros: low cost and ease of processing.
Acry Free is a material that contains no allergens, it is softer and thinner than acrylic. It is easier to get used to such a product.
Nylon restorations fit comfortably in the mouth and do not cause allergies, but do not distribute the chewing load well enough due to their softness.
Metals and plastics are used for fastening elements of partial removable structures. And for the base - the same acrylic and plastics based on acrylic resins.
The service life of acrylic restorations is about 3 years, Acry Free and nylon restorations are 5 years. Dentures are replaced for several reasons. This could be a breakdown, an allergy, or a desire to replace an old design with a more modern one. The main thing is that removable structures do not stop bone loss. The relief of the oral cavity changes, the gums sag, and the restoration no longer fits.
Manufacturing of removable dentures
The process of manufacturing restorations is called clinical-laboratory because it is carried out in close cooperation between the clinic and the laboratory. There are 4 clinical stages in the technology of removable dentures. Between them they carry out work in the laboratory.
First clinical stage
It is performed by an orthopedic dentist. Work begins with collecting anamnesis. The doctor collects information about health status, allergic reactions, and working conditions.
Then the dentist carries out:
- General examination
of the patient. The orthopedist pays attention to the bite, the structure of the jaws, and the condition of the prosthetic bed. The level of preservation of the remaining teeth, if any, is determined. - Special examination
. This includes motor and speech tests, registration of chewing and swallowing characteristics. An X-ray examination is performed and a tomography is performed. - Drawing up a treatment plan
. At this stage, the type of restoration and material for production are determined. - Taking impressions
. Using an orthopedic spoon, the doctor makes anatomical casts of the jaws. In simple cases, this is enough. For complex defects, individual spoons are made. The impressions are sent to the laboratory, where a technician gets to work.
Based on the plaster models, the technician makes an individual spoon. To do this, he uses plastics, thermoplastics or wax. After finishing the work, he hands the spoon to the doctor.
A custom tray is used by the orthopedist to obtain a functional impression. This method is used when:
- severe atrophy of bone tissue;
- some anatomical features (folds on the palatine bed, for example);
- with single-standing teeth, in the case of partial structures.
Second clinical stage
Determination of central occlusion (places of contact when closing the jaws).
Denture manufacturing techniques include casting plaster models and casting wax bases with occlusal ridges. Using them, the doctor determines the central relationship of the jaws. To do this, a wax model is placed in the mouth and height measurements are taken. The orthopedist places marks on the rollers to secure the teeth. At this stage, the color for future crowns is selected.
In the laboratory, the technician places the model in the occluder, selects the size, color and shape of the artificial teeth in accordance with the recommendations of the orthopedist and distributes them into the jaw. He then checks all structural elements.
When making clasp restorations, at this stage the frame is cast. It is ground and polished.
Third clinical stage
Fitting. The goal is to eliminate errors, check aesthetics and conduct speech tests. The doctor makes the adjustment himself; to eliminate complex errors, the product is sent to the laboratory.
After adjustment, installation is carried out. The moment the patient receives the restoration is considered the final clinical stage of the work.
The production of dentures in the clinic’s own laboratory helps the orthopedist and the technician to interact on an ongoing basis and clarify certain issues during the production of the restoration. In addition, working directly in the clinic, the technician is more interested in how the denture is made; the reputation of the clinic depends on his qualifications. This increases responsibility, which affects the quality of structures and ease of use.
Removable dentures using injection molding IVOCAP
Continuing the topic “Removable dentures using injection molding,” I would like to dwell on dentures manufactured using the IVOCAP system. Nowadays, many people are carried away by the manufacture of thermo-molded removable dentures, having forgotten that for many years the IVOCAP system has been in the arsenal of dental technicians. The IVOCAP system allows you to obtain high-precision removable dentures with an ideal fit to the mucosa of the prosthetic bed, precise occlusal relationships and bases without residual monomer. Massive interest in thermo-molded prostheses, in my opinion, is associated with many problems plaguing prostheses made by packing plastic dough into a collapsible cuvette. Many dental technicians and orthopedic dentists, having tried in their practice dentures made by thermomolding, were delighted with the quality of such dentures. However, not many people decided to analyze the reasons for quality. The thermomolding system is very different from the system of packaging plastic dough into a collapsible cuvette, and it is these differences that give the quality that dentists are so pleased with.
What makes dentists happy?
- Exact fit of the prosthesis to the prosthetic bed.
- Precise occlusal relationship of the dentition without overestimating or distorting the bite.
- The absence of residual monomer and, as a consequence, rare cases of allergies to such prostheses.
- Flexibility of prostheses
- Fracture strength and impact resistance of dentures.
Well, these are all good and wonderful properties of removable dentures, but they could have been achieved decades ago using the IVOCAP system, minus, of course, the high flexibility.
The IVOCAP system allows the production of high-quality prostheses; This system is most suitable for the production of complete removable dentures, in contrast to thermomolding systems. What is the advantage of prostheses made using the IVOCAP system over prostheses made by thermomolding? Let me start with the fact that acrylic dentures can be repositioned quite simply and even in the oral cavity. Acrylic plastic is well polished and chemically bonds with acrylic teeth , thereby the aesthetics of acrylic dentures is higher than that of thermo-cast ones (there are no black halos around the teeth, they remain shiny longer). What many dentists love about thermomolded dentures - flexibility - is lost when making complete removable dentures due to the bulk of complete removable dentures. As for the fracture strength and impact resistance of acrylic prostheses, they are, of course, inferior to many thermomolding materials, but not all. In addition, Ivoclar has special reinforced base plastics that have some increased flexibility.
Considering that the only objective indication for the manufacture of a complete removable denture from thermomolded plastics is an allergy to acrylic , it becomes obvious that in most cases for complete dentures it is worth using the IVOCAP injection molding system.
How does it work? Let's look at the step -by-step production of two complete removable dentures using the IVOCAP injection molding system.
After trying on and arranging the teeth on wax bases, we model the bases, so to speak, in their final form. We do not give any permission for processing. The wax base should look the way we would like to see the finished prosthesis. We pour the wax base onto the working model.
We separate the model from the plaster plate of the articulator and prepare the necessary accessories for the IVOCAP system.
We install an analogue cannula in the first half of the cuvette. Cover the bottom of the cuvette with a paper gasket. We mix 2nd class plaster in a vacuum mixer and pour it into the first half of the cuvette, then place the model with the wax composition of the prosthesis soaked in water.
We level the plaster surface and create smooth transitions to the model. After the plaster has cured, we replace the cannula analogue with a cartridge connector with a cannula and install the gating system.
Wet the first half of the cuvette with a release agent. Again, mix the 2nd class plaster in a vacuum mixer and apply a thin layer of plaster to the surface of the prosthesis using a sponge, paying special attention to the interdental spaces.
We assemble the cuvette and fill its second part with plaster. After the plaster has cured, place the cuvette in hot water to remove the wax. Having opened the cuvette and removed the wax, we carefully parasitrate the model and teeth. After cleaning the teeth and plaster molds, we apply an insulating varnish to the plaster.
After the varnish has dried, the cuvette is assembled and installed in a special clamping device. Using a hydraulic press, we clamp the cuvette in this device.
In a special cartridge, which contains a precisely measured amount of polymer powder and monomer liquid at the factory, the base plastic is mixed in a vibrating mixer.
The cartridge is placed in a cuvette, and plastic, using a piston, fills the cuvette under a pressure of 6 atmospheres.
The cuvettes are placed in a polymerization bath with water heated to 95-98 degrees for 35 minutes. After this period has expired, the cuvettes are still placed under pressure in cold water for 10 minutes.
After completion of the polymerization process and cooling, the cuvettes are unpacked.
Without separating the prostheses from the models, we free them from plaster. And after washing and cleaning, we para-jet it and return it to the articulator for adjustment to the bite.
Dentures adjusted to the bite are freed from models, processed and polished.
Prostheses made in this way have a high precision fit to the prosthetic bed, the absence of residual monomer (due to the precise factory dosage of ingredients and their homogenization in a vibrating mixer). Such dentures do not have overbite. The base plastic has a high density and the absence of micropores, which makes such prostheses durable and strong . Even with prolonged use, dentures do not absorb odor or change color . The ability to quickly and accurately reline without large material costs allows you to use such prostheses for many years.
Material for posting on the portal was provided by Mikhail Sledkov.
Similar articles:
Mger Markaryan
Phantom E-max
Cancel
Layer-by-layer application of metal-free ceramics E-max.
Mger Markaryan Read Greggory Kinzer
Who should choose the abutment: the doctor or the technician?
Cancellation
Considering the patient's main complaint about the darkening of the soft tissues in the area of the installed implants, I wanted to choose something more aesthetic than a metal abutment.
Greggory Kinzer Read
Mikhail Sledkov
Saving metal in a foundry laboratory. Problems and consequences
Cancel It
is no secret that foundries cast dental alloys with the addition of the alloy already used in casting. The manufacturers of these alloys write about this in the instructions.
Mikhail Sledkov Read
Mikhail Sledkov
Balance in casting! The foundry man is to blame! Styxes are a way to avoid “balance” when casting extended structures
Cancel
The main issue that concerns all technicians working with metal-ceramics is high-quality casting without “balance”.
Mikhail Sledkov Read
Mikhail Sledkov
Press ceramics - pressing process
Cancel
Continuing the topic of pressed ceramics, I want to talk about some aspects of pressing and possible errors. Many technicians involved in pressing ceramics experience various difficulties and failures in pressing.
Mikhail Sledkov Read
Petr Yanev
Zirconium dioxide: criticism and facts
Cancel
I will try to explain why zirconium dioxide has become my favorite material when it comes to solving complex aesthetic problems using prosthetics.
Petr Yanev Read
Stankevich Ekaterina
Morphology of mandibular molars
Cancel
The article presents various options for the morphology of the lower molars, accompanied by detailed illustrations.
Stankevich Ekaterina Read
Antonyuk Sergey
How to choose the right 3D printer for dentistry
Cancel
How can 3D printing be used, or is already being used, in medicine and, in particular, in dentistry, quite a lot of notes and articles have been written, a large number of reports and lectures have been held.
Antonyuk Sergey Read
Chavushyan Karen, A. V. Krasnopir
Fabrication of ceramic restorations in the anterior region in difficult clinical conditions
Cancellation
Today, patients and dentists pay increased attention to the anterior teeth. This is not surprising, since the requirements for aesthetics and proper functioning are becoming ever higher.
Chavushyan Karen, A. V. Krasnopir Read
Filinov Dmitry
Model builder from 3shape - a simple path from a digital cast to a collapsible model
Cancellation
Digital technologies in dentistry are steadily replacing traditional methods of obtaining impressions and working models.
Filinov Dmitry Read Konstantin Vyshemirsky
How to make an alveolar model
Cancellation
The alveolar model or Heller model is named after its inventor. This model is very beautiful and informative, as it preserves all the gingival tissue, which is very important in aesthetic modeling.
Konstantin Vyshemirsky Read
Simon Haug
Variety of occlusal surfaces of the tooth
Cancel
Modeling natural fissures is one of the most difficult tasks when creating artificial teeth.
Simon Haug Read
- ‹
- 1
Fixed dentures
Fixed restorations include inlays, veneers, crowns and bridges. The manufacturing scheme differs only in small details. For example, let's take the manufacture of a bridge structure.
Preparation for the manufacture of a fixed denture begins with collecting anamnesis, making a diagnosis and preparing the teeth. The first clinical stage ends with the taking of impressions.
First laboratory stage
The impression technician makes a plaster cast and wax base with occlusal ridges. The model is then handed over to the doctor to determine the central occlusion. After this, the model goes back to the technician.
Second laboratory stage
The technician places the model in an articulator (a dental apparatus that simulates the closure of the jaws) and prepares models of ground teeth. Models crowns on abutment teeth and artificial teeth between them. Depending on how the denture is made, the technician makes metal crowns by casting, ceramic ones by pressing, and grinds zirconium crowns on a milling machine. The bridge is transferred to the orthopedist.
The dentist tries on the crowns and adjusts them. Notes any imperfections and sends them to the technician for final processing.
Third laboratory stage
The structure is polished and ground. In the case of metal ceramics, the metal base is processed and a ceramic coating is applied to it. The finished bridge is sent to the orthopedist, who fixes it on the patient’s teeth.
The production of dentures for the upper jaw follows the same protocol as for the lower jaw.
Examples of work “Before” and “After”
Partial restoration of teeth on both jaws
Case: partial absence of teeth on both jaws.
Complete prosthetics of the upper and lower jaws
Case: absence of teeth in the upper jaw (completely), absence of an orthopedic structure in the lower jaw on existing implants (installed in the USA two years earlier) Work: production of a complete removable denture in the upper jaw as a temporary structure until the installation of one-stage implants with subsequent prosthetics.
Combination of removable and fixed prosthetics
Case: Partial absence of chewing teeth on the upper and lower jaws, the need for prosthetics of the anterior teeth of the upper jaw.
Installation of plate dentures with complete edentia (April 2012)
Case: complete absence of teeth in the upper and lower jaws, weak fixation of the removable denture in the lower jaw.