Publication date: March 13, 2022.
Information on this page was updated on December 31, 2021.
TMJ dysfunction is a fairly common pathology these days, as it is largely caused by stress factors. Here it can be difficult to understand what is primary and what is secondary, because people with joint dysfunction usually come with bite pathology, pathology of the musculoskeletal system (curvature of the spine, neck). Therefore, joint treatment is a complex story. It happens that the primary pathology is a pathology of the joint, and sometimes it is the musculoskeletal system.
Comprehensive treatment of TMJ
When the doctor has determined the cause of the joint pathology, or causes, he determines the patient's readiness for a comprehensive treatment plan. In addition to the orthodontist, an osteopath or chiropractor may be involved, or even an orthopedist if more complex correction of the musculoskeletal system is required.
The patient should be aware that it is possible to straighten the jaw using a splint or splint, but this will not solve the problem of malocclusion. Orthodontic treatment will be required to correct the bite. If you have already had orthodontic treatment before, then it is more difficult to decide on repeated treatment.
Therefore, first the problem with the joint is solved using a splint or joint splint, then bite correction is carried out, and, if necessary, prosthetics. In parallel, work is underway with an osteopath to restore the muscular corset of the back and neck.
It happens that a patient refuses treatment with braces after the problem with the joint has been resolved. In this case, we warn him about the need to wear a joint splint constantly in order to avoid the recurrence of old problems with the TMJ. After all, a relapse can happen quite quickly due to stress.
Reasons for the development of the disease
The causes of the pathology are:
- excessive displacement of part of the joint, overcoming the traction of the ligaments;
- weakening of the TMJ, which allows the head to freely come out and move.
These two mechanisms cause the following phenomena:
- mouth opening becomes excessive;
- the joint is exposed to a traumatic effect from the outside;
- it becomes difficult for the patient to bite and chew;
- dislocation develops with any pressure on the joint, even the smallest.
It should be borne in mind that pathology can develop even in completely healthy people. In this case, the cause will be a strong impact on the jaw, injury. Among the reasons for the development of dislocation in the remaining groups are arthritis, severe weakening of the ligaments, and lack of treatment for TMJ subluxation.
What may be the symptoms of TMJ dysfunction?
- Tenderness or pain in the area of one or both TMJs at rest or when opening the mouth.
- Crunching, clicking, crepitation and other noises in the area of one or both TMJs when opening the mouth.
- History of TMJ injuries (previous), incl. dislocation, subluxation, chronic subluxation.
- Restrictions in the mobility of the TMJ, restrictions in opening the mouth.
- Excessive tone of the masticatory muscles, bruxism (“grinding” of teeth in sleep, at rest).
- Asymmetry of the chin, lips, lip frenulum, asymmetry of mouth opening, S-shaped opening.
- Suspicion of a forced position of the lower jaw.
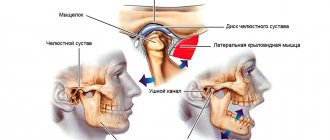
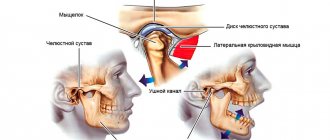
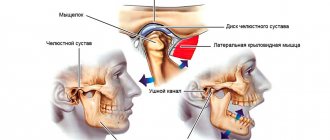
Structure of the TMJ
The presence of one or more of the above symptoms may indicate TMJ dysfunction.
Traditional orthodontic treatment does not address TMJ dysfunction. During orthodontic treatment, the severity of dysfunction may not change, decrease or increase. At the moment, in the world scientific orthodontic literature there is no convincing data on the connection between orthodontic treatment and the condition of TMJ. Deterioration of the joint after treatment may have nothing to do with this treatment.
Note! Even in the absence of visible clinical manifestations of joint dysfunction, hidden disorders may occur that require special diagnostics to identify them.
If there is a forced incorrect position of the lower jaw, its position may change during the treatment process with changes and complication of the treatment plan (the need to remove individual teeth, increasing the duration of treatment). A reliably forced position cannot be diagnosed by traditional orthodontic methods; to verify its presence, as a rule, a special analysis is required (manual functional analysis, determination of the central relationship of the jaws), the use of a special articular splint for a period of several months, which, however, does not give 100 % guarantees.
To conduct a detailed articular diagnosis, explain the specifics of your case, and further manufacture an articular splint, you can make an appointment with an orthodontist who deals with the issue of TMJ dysfunction.
TMJ dysfunction is a chronic condition that can be compensated, but not cured (i.e., it is possible to eliminate symptoms, however, pathological changes in the joints, if they have already occurred, will most likely persist).
What is a temporomandibular joint dislocation?
The extraordinary mobility of the TMJ, which provides all the variety of movements of the lower jaw, also has a downside - these joints are subject to frequent subluxations and dislocations.
During normal functioning of the joint, the head of the mandibular bone leaves the glenoid fossa and then returns back. But under certain conditions, this reverse movement may not occur: the head extends too far and gets stuck in that position. Most often this occurs due to weakening of the articular ligaments, the function of which is to hold the joint together. As a rule, the situation is complicated by the fact that during a dislocation or subluxation, the facial muscles are seized by a spasm, which fixes the displaced position of the joint.
There are dislocations and subluxations of the TMJ. With subluxation, the articular head only deviates slightly from its natural position, while with dislocation, complete displacement and exit from the articular fossa occurs.
Both pathologies are unilateral and bilateral. This means that displacement of the articular head can occur on one side (right or left) or simultaneously in both joints. In addition, depending on the direction of displacement, anterior, posterior and lateral violations are distinguished. If this happens for the first time, they speak of an acute form of the disease. There is also a chronic dislocation of the TMJ, which is characterized by numerous relapses. The pathology acquires a chronic form when the ligaments of the joint are significantly weakened, as well as in the absence of teeth, impaired occlusion (closing) and other defects.
The most common are anterior acute bilateral dislocations. Lateral forms, as a rule, accompany injuries of the lower jaw, including fractures.
What happens if TMJ dysfunction is not treated?
If the dysfunction is not treated, the compensatory capabilities of the body may sooner or later be exhausted, the symptoms will worsen, the pathology will begin to progress, causing greater discomfort (sometimes for several years), thereby affecting the deterioration of the function of the dental system.
In order to try to prevent this and carry out treatment taking into account the individual characteristics of the structure and functioning of the temporomandibular joints, patients are usually offered the following approach.
Signs and causes of TMJ dislocation
The pathology of the TMJ is accompanied by a mechanism of muscle compensation. To prevent further loosening of the joint, the chewing muscles tense, trying to hold the jaws. This results in the development of hypertonicity syndrome of the masticatory muscles on the right, left or both sides of the skull. A person does not always realize the cause of regular headaches, numbness in the cervical spine, and excessive tension in the upper back muscles. But a common cause of dysfunction of the sternocleidomastoid and trapezius muscles is a dislocation of the TMJ. Visually, it seems that the patient’s scoliosis is increasing, but in reality, the deformation of the mandibular joint is progressing.
The main causes of TMJ disorder are recognized to be:
- Skull injury received by a child during childbirth;
- Damage to the jaw as a result of any other trauma;
- Scoliosis;
- Incorrectly formed bite due to various circumstances;
- A large number of missing chewing teeth;
- Poor quality prosthetics or orthodontic intervention.
Let's take a closer look at how the listed sources influence the development of TMJ dysfunction.
Birth injury
The newborn's skull is plastic. When passing through the birth canal, the bones of the head close tightly to make it easier for the baby to be born. In the first weeks of life, the bone plates in most cases stabilize on their own, move apart and “fall into place.” But sometimes it happens that self-correction does not occur or is insufficient.
This condition of the baby is characterized as a birth injury to the skull. The lack of symmetry of the head and its deformation are visible to the naked eye, even to a non-specialist. This negatively affects the child’s health and his ability to adapt to the world around him. The compressed bones of the skull lose mobility, completely or partially, and this leads to an interconnected loss of normal tension of the fascia and membranes in the baby’s head and body. Often, the consequence of a birth injury to the skull is a variety of developmental disorders presented in the list:
- Torticollis, or an inclined position of the head with a turn of the face in the opposite direction of the inclination.
- Increased intestinal spasms, constant and frequent colic.
- Hypertonicity of the muscles, leading to escalation of mobility. The baby constantly straightens and bends his limbs, is overly excited, and begins to walk too early.
- Numerous hormonal changes.
- Delayed physical development.
- Pathologies of the ENT organs: partial loss of smell, persistent rhinitis of various etiologies, swelling of the nasopharynx, proliferation of the tonsils, increased readiness of the mucous membrane to perceive pathogens.
- Tendency to convulsive twitching.
- Breathing disorders, mouth breathing due to a deformed nasopharynx.
- Vision disorders.
- Speech dysfunction and other abnormal changes of varying severity.
In newborn children, the skull is easier to correct. The more the “fontanelles” overgrow, the lower the degree.
If you do not take any action to correct the situation, the body’s compensatory processes are activated, and some manifestations from the above list entail others. Gradually, the body of a growing person will adapt to life with a deformed skull, but the child will not look healthy and anatomically perfect.
Traumatic skull injury before or after age 12
Children fall, hit their foreheads, fight, jump from heights, slide down potholes from ice slides, and in many other ways test their own body’s resistance to damage. It sounds unpleasant, but sometimes a seemingly insignificant injury becomes a trigger for the development of TMJ dislocation and malocclusion. The bones of the skull are displaced, especially within the boundaries of the scaly sutures, but on an x-ray the doctor will not see fractures or other deviations in the integrity of the bone.
Meanwhile, the upper jaw slightly deviates from a clearly horizontal line in the three-dimensional space of the skull. The distortion begins to affect its closure with the mandible.
First, the masticatory muscles will react, tensing and trying to hold the joint while talking or eating. On the side where the misalignment is lower, the upper and lower teeth will begin to hit each other excessively. This will result in numerous dental and periodontal diseases. At the clinic, the patient will be treated for caries, pulpitis, gum disease, etc., but the pain will continue to plague him with its persistence.
As a result, advanced joint pathology develops into TMJ dislocation.
It should be added that a similar situation can develop without external physical impact specifically on the skull. It makes no sense to prohibit a child from jumping and running; TMJ can also suffer as a result of postural disorder in the spine, which is responsible for changes in posture and muscle tone of the entire body.
For diagnosis and treatment of the temporomandibular joint, contact Dr. Lopaeva Olga Zhorzhevna. Make an appointment
Make an appointment
Or call +7(985)532-21-01
Scoliosis of the spine
The human body is a living and functioning system of very fine organization. Any change in one part or organ triggers a cascade of responses in all departments and organ systems. And the musculoskeletal system is almost never left out.
Most doctors consider the patient’s complaints separately from the pathology of the TMJ and do not even attach importance to the diagnosis of the latter. Meanwhile, TMJ dysfunction can be associated with posture—the habitual posture of the body. The relationship between posture and occlusion (dental bite) must certainly be taken into account when identifying problems in both cases. And it is especially necessary to monitor the position of the sacroiliac joint when treating disorders in the jaw joint.
Inside the skull and spinal column is the dura mater, a dense structure attached to the bones and incapable of stretching. Thanks to it, there is communication between all departments of this system. There is fusion of the dura mater with the bones of the occipital bone of the skull and with the bones of the sacrum. When a person moves normally, these areas perform synchronous vibrations. If the membrane is stretched unnaturally (due to scoliosis, as a result of pelvic or cranial pathology), this affects the normal functioning of two areas at the same time. The disorder from the pelvis instantly ascends to the thoracic and cervical spine, affecting the functioning of the TMJ. The mechanism works in the opposite direction in a similar way.
Now let's try to imagine the system in action. Suppose a person injured his leg and a spasm developed. To avoid pain, he will begin to take care of the sore limb and transfer the entire weight of the body to the healthy one.
The postural system operates in the same way when a misalignment occurs in one area of it. If there is excess tension, the body will try to stabilize and shift the center of gravity so that balance returns to the system. Therefore, the body, with the help of the central nervous system, will send commands to various muscles so that they relax or, conversely, contract, supporting the person in the most comfortable position. This flow of commands will also affect the head, which will bend when searching for balance.
What happens inside the skull? In that part of it that is inclined lower from the vertical axis, intracranial pressure will increase. The brain, in order to neutralize the created dangerous situation, will send a signal to the masticatory muscles, which will contract on the opposite side. In this case, the head will turn around so that the pressure inside the skull returns to normal limits. How it will look externally depends on the degree of imbalance of the postural system.
Three developed systems are responsible for the balance of the body in space - the eyes, feet and vestibular apparatus. If there is a violation in any of them, the remaining ones take on part of the load. If a spasm of the neck muscles in an attempt to restore balance has led to a tilt of the head, then a discord arises between the information that enters the brain from the eyes and from the vestibular system. Therefore, the central nervous system commands the muscles to return to an order in which the received signals are synchronized. The muscles of the skull and other parts of the neck contract, returning the eyes to the horizontal plane.
Malocclusion
Common causes of occlusion:
- Trauma to the jaw, which led to a shift in the relative position of the upper and lower rows of teeth;
- Absence of molars and premolars;
- Poorly performed prosthetics or orthodontic treatment.
In case of birth or life injuries, the upper jaw is blocked in an unnatural position. This provokes improper movement and growth of the bones of the palate and the jaw itself. As a result, the dentition develops incorrectly. The teeth grow crowded, at an angle, sometimes even in several rows.
When the upper jaw moves back from its natural projection, the airway part of the nasopharynx loses volume. Now the lower jaw strives to “catch up” with the upper jaw in order to combine the teeth in an acceptable occlusion. As a result of this transformation, the intracranial bones responsible for breathing through the nose become blocked. The soft tissues deep in the nasal passages begin to swell, the lymphoid tissue grows, creating additional interference with air exchange. The mucous membrane also loses elasticity, loosens, and becomes susceptible to pathogenic bacteria.
If a child’s mouth breathing predominates, this is most likely caused by similar pathological transformations. Adults develop snoring and possibly apnea. One problem leads to another. Trying to give access to air, the central nervous system sends a command to the head to shift its position relative to the body. This provokes other adverse reactions in the form of decreased immunity and loss of mucosal resistance to allergens. The tonsils become enlarged and polyps develop in the nose. Subsequently, the general reactivity of the body becomes tense, and a wave of allergic reactions to food, household dust, medications, etc. increases.
Consequences of orthodontic intervention and prosthetics
The human body is highly lable and adapts to many influences from the outside and inside. We adapt to changing temperatures, adapt to darkness and light, get used to smells and sounds and stop perceiving them as irritants. Of course, the adjustment mechanism is activated when the cranial bones become imbalanced. However, the result is a displacement of the bite from the normal boundaries. If the dentist does not pay attention to the entire jaw system as a whole, but is concerned with the condition of a single tooth, then the slightest deviation in the height, size, or inclination of the filling or prosthesis will destroy the achieved stability and affect the entire body.
If the upper jaw is blocked at an angle, there will be a strong load on the teeth on the lower side. Even neuritis of the nearby part of the trigeminal nerve is possible. Along the way, enamel wears off, gums recede, and periodontal pockets grow. A person becomes a regular patient of a dental clinic.
Behind the upper jaw, the lower jaw invariably begins to move, obeying signals from the brain. No matter which direction the upper jaw turns, the mandible always turns next. These geometric deformations greatly harm the TMJ. The head of the lower bone gradually squeezes out the articular disc and collapses itself, causing pain.
Treatment method for TMJ dysfunction
1. Diagnosis of TMJ dysfunction.
- When diagnosing a joint in the clinic, a series of measurements and tests are carried out, all sensations in the joint area are recorded (discomfort, clicks, pain, deviation of the jaw when opening and closing), the difference in sensations in the right and left joint.
- The orthodontist also takes impressions of the jaws and takes photographs of the face and intraoral photographs, and also performs three-dimensional computed tomography of the face (3D CT); if necessary, the doctor can give a referral for an additional study - magnetic resonance imaging of the TMJ (MRI).
- Often, the orthodontist, in addition to manual functional analysis, conducts a visual assessment of: posture, symmetry of the shoulder girdle, shoulder blades, hip bone structures, etc., performs the necessary tests and photographs. Based on the results, it is possible to schedule a consultation with an osteopath or chiropractor to jointly manage the patient. Related specialists (orthopedist, surgeon, periodontist) can also be involved in drawing up a treatment plan.
What exercises are prescribed to patients to normalize the work and relax the masticatory muscles?
Exercise No. 1
Draw a vertical line on the mirror with a marker, stand opposite so that the line divides your face into the right and left halves, place your fingers on the area of the articular heads, lift your tongue up and back, open and close your mouth along the line (it may not work right away), 2-3 times /day 30 repetitions. There is no need to open your mouth wide (a comfortable width), the main thing is symmetrically (so that the jaw does not “move” in any direction). If there is a click, open until it clicks.
Exercise No. 2 (cycle)
Do it whenever possible, for example, in front of the TV, at the computer, or in a traffic jam while driving. Open and close your mouth without closing your teeth for 30 seconds, then alternately reach your right and left cheeks with your tongue for 30 seconds. Open - close your mouth again, then for 30 seconds move your tongue in a circle inside the vestibule (behind the lips), first in one direction, then in the other direction (clockwise - counterclockwise), open again - close your mouth, etc.. For this a half-hour cycle, the teeth should not touch, the lips should be closed. If you want to close your mouth or swallow, place your tongue between your teeth. Repeat the cycle for 20-30 minutes 2-3 times/day
Occlusive therapy for TMJ dysfunction
After diagnosis, the patient is scheduled for an appointment with the orthodontist to determine the central relationship of the jaws (“true” position of the lower jaw, the position in which your joint and chewing muscles will be most comfortable).
In order to more accurately establish and fix this position, an occlusal splint (splint) will be individually made for the patient from a special plastic, which is erased as it is worn. The splint must be worn constantly (sleeping, talking, eating in it if possible) - this is the meaning of occlusion therapy, which will help the joint and masticatory muscles rebuild into the most comfortable functional state.
Cleaning and caring for the splint is very simple - after eating (as well as while brushing your teeth), brush with a soft brush with toothpaste or soap.
Installation of a brace system for a patient with TMJ dysfunction
Installation of a brace system on the upper jaw is carried out on average after 3 months of occlusion therapy. The splint is adjusted once every 1-2 weeks, or at the discretion of the doctor, until the main complaints from the TMJ are eliminated (in parallel with the alignment of the teeth in the upper jaw), then a brace system is installed on the lower jaw with partial reduction (grinding) of the interfering parts of the occlusal tires, or complete removal. Here the patient needs to be patient - the process may take several months.
At the same time, the new position of the lower jaw is monitored: repeated manual functional analysis, photometry, bite registration is possible, computed tomography of the face during treatment, continuation of orthodontic treatment with a brace system.
Upon completion of orthodontic treatment, final monitoring of the position of the lower jaw follows (manual functional analysis, photometry, bite registration, 3D CT scan of the face upon completion (after) treatment).
Joint splint
Joint splint with braces