general information
The trigeminal nerve consists of sensory and motor fibers. It originates in the structures of the brain and is divided into three branches:
- ophthalmic: responsible for the eye, forehead and upper eyelid;
- maxillary: innervates the area from the lower eyelid to the upper lip;
- mandibular: involves the chin, lower jaw, lips and gums.
With neuralgia, one or more branches of the trigeminal nerve are affected, which determines the main symptoms of the pathology. People over 45 years of age are most susceptible to the disease, and women get sick more often than men.
Make an appointment
Serious diseases of the body
If the lower jaw is numb and the symptom either goes away or systematically appears again and again, then this may indicate cervical osteochondrosis. The problem arises due to poor circulation, compression of nerves and blood vessels in the cervical spine. In this case, the jaw, chin, lips become numb, and dizziness becomes a constant companion of the sick person.
Often, facial paresthesia (a sensitivity disorder characterized by tingling and numbness) occurs due to serious illnesses that require immediate medical attention. Let's list them:
- neuritis and neuroses,
- diabetes mellitus: an unpleasant symptom appears due to a decrease in blood glucose levels,
- hypertension,
- epilepsy,
- sinusitis and sinusitis: the upper jaw goes numb,
- meningitis,
- stroke and cerebrovascular accident,
- vegetative-vascular dystonia and anemia,
- oncology: the problem occurs due to compression of the spinal cord or brain by a tumor.
This symptom may be a consequence of a serious illness in the body.
Causes
The causes of trigeminal neuralgia can be of different nature:
- compression of the entire trigeminal nerve or its branches against the background of: enlargement of the arteries or veins of the brain (aneurysms, atherosclerosis, strokes, increased intracranial pressure due to osteochondrosis, congenital developmental features);
- tumors of the brain or facial tissues in close proximity to nerve fibers;
- congenital anomalies of bone structure, narrowed openings through which nerve branches pass;
- injuries of the skull, facial area: bone fractures, post-traumatic scars of soft tissues;
- proliferation of scar tissue after injury, surgery, inflammation;
The risk of developing trigeminal neuralgia increases significantly:
- over the age of 50;
- against the background of mental disorders;
- with regular hypothermia;
- with insufficient intake of nutrients and vitamins into the body (anorexia, bulimia, malabsorption, etc.);
- with regular overwork, stress;
- for helminthic infestations and other helminthiases;
- for acute infections: malaria, syphilis, botulism, etc.;
- for chronic inflammation in the oral cavity (caries, gingivitis, abscesses, etc.);
- against the background of autoimmune lesions;
- with excessive exposure to allergies;
- for metabolic disorders.
Causes of arthrosis of the temporomandibular joint
Arthrosis can be triggered by a one-time injury (compression, blow, bruise), as a result of which cracks and erosions appear on the articular surfaces. The disease is caused by a fracture of the condyle and condylar process if the fusion is incorrect.
Other reasons:
- prolonged stress;
- consequence of acute traumatic arthritis;
- birth trauma (arthrosis develops due to improper application of forceps);
- underdevelopment of the jaw (microgenia);
- sudden removal of molars (accident, fight);
- errors during dental prosthetics;
- impaired coordination of muscle contractions during dislocation and subsequent sharp (jerky, zigzag, circular) movements of the jaw;
- complete absence of teeth;
- deep bite;
- introduction of drugs into the joint cavity (for example, hydrocortisone, glucose solutions, novocaine).
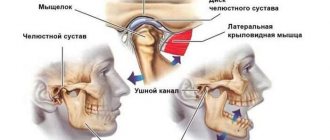
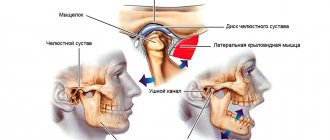
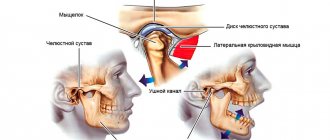
Structure of the TMJ
Etiological factors of arthrosis (without which the disease does not develop):
- infections;
- metabolic disease;
- injuries;
- atherosclerosis of the terminal branches of blood vessels;
- prolonged spastic contraction of the lateral pterygoid muscle (responsible for moving the jaw forward and to the side).
Even children are diagnosed with TMJ arthrosis. In newborns, the disease develops as a result of birth trauma. Dysfunction in the joint due to various malocclusions is observed in 40% of children from 4 to 14 years old, but in only 1% x-rays reveal coracoid (myogenic) arthrosis.
During menopause, the likelihood of developing arthrosis due to endocrine disorders increases. With age, it is possible to develop senile, i.e. invaluable arthrosis, when cartilage tissue cannot recover, dries out and collapses.
At risk are people whose professional activities involve inadequate load on the joint (violinists), or those suffering from spasms of the masticatory muscles (bruxism).
Symptoms
The main characteristic symptom of trigeminal neuralgia is paroxysmal pain. It comes suddenly and in its intensity and speed of spread resembles an electric shock. Typically, intense pain forces the patient to freeze in place, waiting for relief. The attack can last from a few seconds to 2-3 minutes, after which there is a period of calm. The next wave of pain may come within hours, days, weeks or months.
Over time, the duration of each attack of neuralgia increases, and periods of calm are reduced until a continuous aching pain develops.
The provoking factor is irritation of trigger points:
- lips;
- wings of the nose;
- eyebrow area;
- middle part of the chin;
- cheeks;
- area of the external auditory canal;
- oral cavity;
- temporomandibular joint.
A person often provokes an attack when performing hygiene procedures (combing hair, caring for the oral cavity), chewing, laughing, talking, yawning, etc.
Depending on the location of the lesion, the pain takes over:
- the upper half of the head, temple, orbit or nose if the ophthalmic branch of the nerve is affected;
- cheeks, lips, upper jaw – if the maxillary branch is affected;
- chin, lower jaw, as well as the area in front of the ear - with neuralgia of the mandibular branch.
If the lesion affects all three branches or the nerve itself before it is divided, the pain spreads to the entire corresponding half of the face.
Painful sensations are accompanied by other sensory disturbances: numbness, tingling or crawling sensations. Hyperacusis (increased hearing sensitivity) may be observed on the affected side.
Since the trigeminal nerve contains not only sensory, but also motor pathways for the transmission of impulses, with neuralgia the corresponding symptoms are observed:
- twitching of facial muscles;
- spasms of the muscles of the eyelids, masticatory muscles;
The third group of manifestations of neuralgia are trophic disorders. They are associated with a sharp deterioration in blood circulation and lymph outflow. The skin becomes dry, begins to peel, and wrinkles appear. Local graying and even hair loss in the affected area is observed. Not only the scalp suffers, but also the eyebrows and eyelashes. Impaired blood supply to the gums leads to the development of periodontal disease. At the time of the attack, the patient notes lacrimation and drooling, swelling of the facial tissues.
Constant spasms of muscle fibers on the diseased side lead to facial asymmetry: narrowing of the palpebral fissure, drooping of the upper eyelid and eyebrow, upward movement of the corner of the mouth on the healthy side or drooping on the diseased side.
The patient himself gradually becomes nervous and irritable, and often limits himself to food, since chewing can cause another attack.
General clinical recommendations and prevention
With arthrosis of the temporomandibular joint, it is necessary to reduce the load on the joint. To do this, you need to restore the integrity of the dentition and periodically wear braces. If you are involved in (and cannot quit) contact sports (boxing, martial arts), be sure to wear sports mouthguards.
To restore blood circulation in the joint, it is recommended to slowly (!) open and close your mouth (without sudden or lateral movements).
You will also have to get rid of habits that create additional stress on the joint:
- chew gum vigorously;
- support your cheek with your palm;
- chew seeds, nuts, hard cartilage.
Osteoarthritis of the jaw joint is called a disease of suppressed emotions. The illness can be a consequence of divorce, dismissal, or critical life situations. The most severe forms develop in nice and non-conflict people who keep their own emotions to themselves. You need to learn to enjoy life and stop seeing the world in gray colors.
Diagnostics
A neurologist diagnoses trigeminal neuralgia. During the first visit, he carefully interviews the patient to find out:
- complaints: nature of pain, its intensity and localization, conditions and frequency of attacks, their duration;
- medical history: when pain attacks first appeared, how they changed over time, etc.;
- life history: the presence of chronic diseases, previous injuries and operations is clarified, special attention is paid to dental diseases and interventions.
A basic examination includes assessing the condition of the skin and muscles, identifying asymmetry and other characteristic signs, checking the quality of reflexes and skin sensitivity.
To confirm the diagnosis, the following is carried out:
- MRI of the brain and spinal cord with or without contrast: allows you to identify tumors, consequences of injuries, vascular disorders; sometimes the study is replaced by computed tomography (CT), but it is not as informative;
- electroneurography: study of the speed of nerve impulse transmission through fibers; allows you to identify the fact of nerve damage, assess the level of the defect and its features;
- electroneuromyography: not only the speed of impulse passage along the nerve bundle is studied, but also the reaction of muscle fibers to it; allows you to assess nerve damage, as well as determine the sensitivity threshold of trigger zones;
- electroencephalography (EEG): assessment of the bioelectrical activity of the brain.
Laboratory diagnostics includes only general studies to exclude other causes of painful attacks, as well as to assess the condition of the body as a whole (usually a general blood and urine test is prescribed, as well as a standard set of biochemical blood tests). If the infectious nature of the disease is suspected, tests are carried out to identify specific pathogens or antibodies to them.
Additionally, consultations with specialized specialists are prescribed: ENT specialist (if there are signs of nasopharynx pathology), a neurosurgeon (if there are signs of a tumor or injury), and a dentist.
Hemifacial spasm (facial hemispasm) - symptoms and treatment
The main goal of treatment for hemifacial spasm is to achieve stable remission without losing the patient’s ability to work and social activity [25].
medications are used to treat hemifacial spasm : clonazepam, levetirace, carbamazepine, baclofen, gabapentin [7]. They belong to anticonvulsants and muscle relaxants, affecting muscle tone and the ability to conduct nerve impulses. However, their effectiveness has not been reliably proven. In addition, patients are forced to take drugs for a long time in fairly high doses, which inevitably leads to side effects such as lethargy, drowsiness, lethargy, dizziness, muscle weakness, dyspeptic disorders, fluctuations in blood pressure, rhythm disturbances and cardiac conduction, and many others. which affects the quality of life.
For primary hemifacial spasm, neurosurgical intervention (microvascular decompression of the facial nerve) is possible, which has shown its effectiveness in 86-93% of cases of surgical treatment. It was developed and first performed in February 1966 by the American neurosurgeon Peter Jannetta [7]. First, the doctor makes an incision in the area behind the ear on the affected side, then cuts out a small area of bone. Having displaced the cerebellar hemisphere, the doctor determines the compression zone and eliminates it: delicately separates the vessel from the nerve and places a special biologically inert material - Teflon wool - between them. The bone defect is replaced with a bone fragment or a special plate, which is firmly fixed.
For secondary hemifacial spasms, it will be effective to eliminate the cause (removal of the tumor, exclusion of the aneurysm from the bloodstream, treatment of the underlying disease, etc.).
In the presence of contraindications to surgical treatment, in case of secondary hemifacial spasm, when surgical treatment is not indicated (stroke, multiple sclerosis, etc.), refusal of surgery, and in elderly people, injections of botulinum toxin type A (BTA) [1 ][7]. According to the recommendation of the European Federation of Neurological Societies (EFNS, 2011), BTA drugs are recommended as the first line of treatment for hemifacial spasm (recommendation class C) [28].
BTA is a highly effective treatment method for hemifacial spasm with minimal risk of adverse events and can be considered as an alternative to surgical treatment. It has been verified by controlled studies and 35 years of clinical practice [26]. Moreover, it is known that in 20% of cases of surgical treatment of hemifacial spasm, a relapse develops; side effects are frequent (impaired functions of the cranial nerves, infections, liquorrhea, hemorrhages), which are more difficult for patients to tolerate than BTA [7].
Californian ophthalmologist Alan Scott first used BTA in 1977 to treat strabismus. In 1985, he was the first to use local injections of BTA in humans for the treatment of blepharospasm and hemifacial spasm [29]. In 1985, neurologist Mitchell Breen published results of successful treatment of blepharospasm and hemifacial spasm using BTA [30]. Since then, BTA has been used not only in ophthalmology, but also in the treatment of diseases of the nervous system. The use of BTA was officially approved by the FDA (Food and Drug Administration - USA) in 1989. One of the first indications for the use of BTA was hemifacial spasm [31].
Botulinum toxin is produced by the gram-positive bacterium Clostridium botulinum. It is a neurotoxin that blocks the release of acetylcholine (a neurotransmitter that mediates the transmission of signals between neurons) from the presynaptic nerve ending. Thus, peripheral cholinergic (excited by acetylcholine) transmission at the neuromuscular synapse is disrupted. This reduces muscle contraction and leads to a dose-dependent, reversible decrease in muscle strength [25][26].
In Russia, the following BTA preparations are approved for use: conditionally 100-unit - "Botox", "Lantox", "Xeomin", "Relatox", "Botulax" (some drugs are available in bottles of 50 and 200 units) and " Dysport" (in bottles of 300 and 500 units). The drugs have similar effectiveness; they differ in storage and dilution features. Only in the instructions for the drug "Relatox" (Russia) hemifacial spasm is not included in the indications for use. The dosage of the drug is calculated individually for each patient and in accordance with the instructions for medical use. The conversion factor for units of action between Dysport and 100-unit drugs has been scientifically calculated; it is 3:1 or less for neurological indications and 2.5:1 for aesthetic indications [32]. The final dose calculation remains with the doctor. In Wolfgang Jost's atlas of botulinum therapy, doses are already indicated taking into account this recalculation per point of administration [33]. When treating hemifacial spasm, the average dose for Dysport can be 120-170 units. [14], for Xeomin - 30-50 units. depending on the muscles involved. The dose of administration at one point for Xeomin is 1.25-5 units. [33][34].
BTA is able to eliminate hyperkinesis during hemifacial spasm while preserving muscle function; it must be prescribed as soon as the diagnosis is made. Before carrying out botulinum therapy, the doctor must obtain voluntary informed consent for BTA injections. Injection sessions are recommended every 3-4 months in the target muscles. It is permissible to carry out injections “at the patient’s request,” that is, earlier or later than the recommended dates. This depends on the resumption of hemifacial spasm symptoms. After injections, it is recommended to actively contract the injected muscles for 20 minutes, and the patient should be under medical supervision for 1 hour to monitor for immediate allergic reactions [26]. To reduce the risk of developing intradermal hematomas on the face, it is recommended to cool the injection sites for 10-20 minutes.
A decrease in hyperkinesis after the administration of botulinum toxin is usually observed quite quickly - already on days 2-5, sometimes reaching the maximum effect by the end of the week (less often by days 10-14). The effect lasts up to 3-6 months. With regular repeated administrations of BTA, in most cases the positive effect is consolidated. The severity of hyperkinesis when they resume is less than before botulinum therapy and tends to decrease [14]. For facial symmetry in the muscles contralateral (on the opposite side) to the hemifacial spasm, it is necessary to perform BTA injections at 50% of the dose administered into the ipsilateral (on the side of the disease) muscles. It is advisable to do this after 2-3 weeks to evaluate the effect of the injected BTA and identify the muscles requiring aesthetic correction [35]. There is usually no decrease in sensitivity to BTA. Against the background of the effect of therapy, there is the possibility of gradual withdrawal of previously received medications [14][34].
More often, injections are performed in the following muscles: the circular muscle of the eye (orbicularis oculi); zygomaticus minor (zygomaticus major et minor); circular muscle of the mouth (orbicularis oris); subcutaneous muscle of the neck (platysma); frontal muscle (frontalis); muscle that wrinkles the eyebrow (corrugator supercilii); muscle that lowers the nose (procerus); nasal muscle (nasalis); muscle that lifts the upper lip and wing of the nose (levator labii superioris alaeque nasi); muscle that lifts the upper lip (levator labii superioris); laughter muscle (risorius); muscle that lifts the angle of the mouth (levator anguli oris). The drug should not be injected into the middle zone of the upper eyelid - in the projection of the muscle that lifts the upper eyelid, as this can lead to drooping of the eyelid [26][28].
Treatment with the drug should be carried out by specialists (neurologists, neurosurgeons) who have experience in the diagnosis and treatment of such conditions and have been trained in the treatment.
Contraindications to the use of BTA include pregnancy, hypersensitivity to one of the components of the drug, and acute diseases [26]. In the treatment of hemifacial spasm, according to various authors, temporary adverse reactions . They are distributed according to frequency as follows: very often - ptosis (drooping); often - weakness of the facial muscles, diplopia (double vision), dry eyes, swelling of the eyelids, lacrimation; infrequently - paresis (weakening) of facial muscles; rarely - ophthalmoplegia (paralysis of the eye muscles), entropion of the eyelid [26]. They do not require additional interventions and regress on their own within a few weeks [14][26][34]. To reduce the risk of side effects, it is important to maintain the dose of BTA and begin treatment with the minimum effective doses. Drugs that affect neuromuscular transmission, such as aminoglycoside antibiotics, should be used with caution during the period of BTA action [26].
To assess the effectiveness of treatment, scientists have developed a special system using five- and six-point scales. For example, according to Vincent Marneffe (neurosurgeon) [36], the result is considered “excellent” with the complete disappearance of hyperkinesis, “good” - if the disappearance is more than 80%, “satisfactory” - if the disappearance is from 20 to 80%, “unsatisfactory” - if hyperkinesis disappeared by less than 20%. Tetsuo Iwakuma et al [37], Peter Giannetta [21], Robert Auger et al [38] suggested “excellent,” “good,” “satisfactory,” “unsatisfactory,” “poor,” and “recurrent” results for the treatment of hemifacial spasm. One should strive to achieve “excellent” and “good” treatment results [7].
Drug therapy for hemifacial spasm is a thing of the past. Only in the presence of comorbid disorders (depression) can a doctor prescribe antidepressants in addition to the main treatment [25][26].
Thus, the use of BTA requires visiting a doctor 3-4 times a year without the need to constantly take other medications and undergo other procedures. It is also necessary to conduct cognitive behavioral therapy with patients for better social adaptation [25][26].
Treatment of trigeminal neuralgia
Treatment is aimed at:
- to eliminate the cause of damage;
- to alleviate the patient's condition;
- to stimulate the restoration of nerve structures;
- to reduce the excitability of trigger zones.
Properly selected treatment can reduce the frequency, intensity and duration of pain waves, and ideally achieve stable remission.
Drug treatment
Trigeminal neuralgia requires complex treatment using drugs from several groups:
- anticonvulsants (carbamazepine and analogues): reduce the excitability of nerve fibers;
- muscle relaxants (baclofen, mydocalm): reduce muscle spasms, improve blood circulation, reduce pain;
- B vitamins (neuromultivit, milgamma): stimulate the restoration of nerve fibers, have an antidepressant effect;
- antihistamines (diphenhydramine): enhance the effect of anticonvulsants;
- sedatives and antidepressants (glycine, aminazine): stabilize the patient’s emotional state.
For severe pain, narcotic analgesics may be prescribed. Previously, drug blockades (injecting the problem area with anesthetics) were actively used, but today this method of treatment is almost never used. It contributes to additional damage to nerve fibers.
Treatment of the root cause of the disease is mandatory: elimination of dental problems, taking medications to improve cerebral circulation, etc.
Physiotherapy and other non-drug methods
Non-drug methods complement drug therapy well and help stabilize patients’ condition. Depending on the condition and concomitant diseases, the following may be prescribed:
- ultraviolet irradiation: inhibits the passage of impulses along nerve fibers, providing an analgesic effect;
- laser therapy: reduces pain;
- UHF therapy: improves microcirculation and prevents muscle atrophy;
- electrophoresis with analgesics or antispasmodics to relieve pain and relax muscles;
- diadynamic currents: reduce the conductivity of nerve fibers, significantly increase the intervals between attacks;
- massage of the face, head, cervical-collar area: improves blood circulation and lymph outflow, improving tissue nutrition; must be carried out with caution so as not to touch trigger zones and provoke an attack; the course is carried out only during the period of remission;
- acupuncture: helps relieve pain.
Surgery
The help of surgeons is indispensable when it is necessary to eliminate nerve compression. If indicated, the following is carried out:
- removal of tumors;
- displacement or removal of dilated vessels pressing on the nerve (microvascular decompression);
- expansion of the bone canals in which the branches of the nerve pass.
A number of operations are aimed at reducing nerve fiber conductivity:
- exposure to a gamma knife or cyber knife;
- balloon compression of the trigeminal node: compression of the node using an air-filled balloon installed in close proximity to it, followed by death of the nerve fibers; surgery often leads to partial loss of sensation and decreased muscle movement;
- resection of the trigeminal node: rarely performed due to the complexity and large number of complications.
Make an appointment
What to do
To get rid of unpleasant sensations, you need to identify their cause.
In most cases, it is enough to adjust the regime - take breaks from work, exercises to strengthen the neck muscles, choose a comfortable pillow.
If numbness is a symptom of the disease, treatment is selected depending on the etiology.
Changing mode
The following recommendations will help you get rid of this unpleasant symptom:
- normalization of the work and rest regime (take short breaks every 45 minutes of work);
- physiotherapy;
- massage of the collar area;
- properly selected pillow and mattress.
Following these recommendations will relieve sensitivity disorders if there is no organic cause.
Drug treatment
Treatment consists of eliminating the cause, that is, the underlying disease. Symptomatic therapy is not provided.
| Disease | Treatment methods |
| Transient ischemic attack | The main goal of treating TIA is to restore normal blood flow. The following drugs can be used for this: · antiplatelet agents (Aspirin, Clopidogrel); · indirect anticoagulants; · infusion therapy. It is also important to treat concomitant diseases that increase the risk of stroke - arterial hypertension, atherosclerosis and diabetes. |
| Trigeminal neuralgia | For treatment, antiepileptic drugs are used - Carbamazepine, Oxcarbazepine. Additionally: · anti-inflammatory drugs; · painkillers; · sanitation of the oral cavity. |
| Osteochondrosis | Treatment of osteochondrosis is complex: · drug therapy, which includes anti-inflammatory drugs, muscle relaxants, B vitamins; · physiotherapy; · fixation of the cervical spine (Schanz collar). |
| Migraine | Drug treatment includes the following drugs: · analgesics (Solpadeine, Ibuprofen); · serotonin inhibitors (Naratriptan, Sumatriptan); · beta blockers (Metoprolol, Propranolol); · antidepressants (Amitriptyline). |
Complications
Without treatment, trigeminal neuralgia gradually progresses. Over time, a pathological pain focus forms in one of the parts of the brain. As a result, the pain covers the entire face, is provoked by any minor irritant and even the memory of an attack, and subsequently becomes permanent. Vegetative-trophic disorders progress:
- irreversible atrophy of the facial muscles is formed;
- teeth become loose and begin to fall out due to advanced periodontal disease;
- baldness is increasing.
Due to constant pain, the patient's sleep is disturbed and severe depression develops. In severe cases, patients may commit suicide.
Prevention
Prevention of trigeminal neuralgia is a set of simple measures that significantly reduce the risk of developing pathology. Doctors recommend:
- undergo regular preventive examinations;
- at the first signs of the disease, seek help (the sooner treatment is started, the greater its effect will be);
- eat right, get the required amount of vitamins, minerals, unsaturated fatty acids;
- regularly engage in light sports and gymnastics;
- get enough sleep and rest;
- minimize stress and physical overload;
- avoid hypothermia and harden yourself;
- to refuse from bad habits.
Treatment at the Energy of Health clinic
If you or your relative are bothered by severe pain in one or another part of the face, the neurologists of the Health Energy clinic will come to the rescue. We will conduct a full diagnosis to identify the causes of the pathology and prescribe comprehensive treatment. At your service:
- modern drug regimens to reduce the frequency and intensity of attacks;
- physiotherapeutic procedures: magnetotherapy, laser therapy, electrophoresis, phonophoresis, etc.;
- delicate therapeutic massage;
- acupuncture;
- help from a psychologist if necessary.
Problems in the lower jaw
Loss of sensitivity after bone grafting, like any other surgical interventions, is much more common in the lower jaw. This is due to the fact that during surgery, with an atypically high location of the mandibular canal or a small amount of bone tissue, nerve damage or compression may occur.
Nerve damage during surgery
Thanks to the widespread use of radiography and computed tomography, such a complication is now extremely rare. It may be associated with an atypical location of the mandibular canal, fragility of bone tissue, or medical error.
During the process of access, removal of tooth root debris, and formation of new bone tissue, the nerve may be damaged by the instrument or compressed by excessive amounts of new bone mass. In this case, after the end of anesthesia, numbness of the teeth anterior to the site of bone grafting, the lower lip, chin, and part of the cheek may persist.
Nerve compression due to implant displacement
If a dental implant changes its location due to injury, inflammation, or violation of medical instructions, compression of the mandibular nerve may occur. A similar situation can develop both in the first days and weeks after surgery, and after a long time.
With such a nerve trunk injury, extremely severe pain may initially be felt, and only then numbness may appear.
Nerve compression due to abnormal healing
After bone grafting, the slow process of new bone formation begins. Sometimes regenerative processes follow a pathological path, when newly formed tissues compress surrounding structures, blood vessels, and nerves.
This condition develops gradually, over 1-3 months after surgery. Numbness also does not appear immediately. Initially, it may be almost invisible or appear occasionally, passing after some time. Over time, numbness may increase or may remain at the same level.
Advantages of the Health Energy Clinic
The Health Energy Clinic is a multidisciplinary medical center where every patient has access to:
- screening diagnostic programs aimed at early detection of diseases and pathologies;
- targeted diagnostics using modern equipment and laboratory tests;
- consultations with experienced specialists, including foreign ones;
- modern and effective comprehensive treatment;
- necessary certificates and extracts;
- documents and appointments for spa treatment.
Trigeminal neuralgia is a serious pathology that can seriously disrupt a person’s normal lifestyle. Don't let pain and fear take over your thoughts, get treatment at Health Energy.