Bone exostosis or osteochondroma is the most common skeletal tumor. It accounts for about 20% of all cases of the formation of bone tumors and almost 40% of the development of all benign bone tumors. Most often it is detected before the age of 20, although it is usually asymptomatic. Only in isolated cases does pain and other disorders occur. Nevertheless, the formation of a growth on the bone necessarily requires consultation with a doctor, since malignancy or malignancy of osteochondroma is rare, but still possible.
What is bone exostosis
Osteochondral exostosis is a benign osteochondral formation on the outer surface of the bone. Most often, it is detected at a young age before the end of skeletal growth, including in children.
The formation of osteochondroma provokes a disruption of the natural processes of resorption (resorption) and the formation of new bone tissue (remodeling).
Exostosis is a growth formed by spongy bone and having a cortical layer (a strong, hard “shell”). It can grow on a stalk or be attached to a bone with a wide base. On the outside, the bone growth is covered with cartilage tissue, which has much in common with articular cartilage. Its thickness does not exceed 1 cm. The top layer of exostosis is also called a cartilaginous cap.
Osteochondroma is a consequence of impaired bone growth in the area of the epiphyseal plates, i.e., their displacement from the anatomically correct position with the “throwout” of cartilage tissue to the side. Subsequently, just like the metaphysis, it ossifies in the direction from the base to the apex, which leads to the formation of bone exostosis with a cartilaginous cap. At the same time, it continues to increase in size until the growth zones close, and can appear in absolutely any bone. The bony part of osteochondroma is formed from unevenly distributed bone beams. Between them there is adipose tissue with islets of hematopoiesis. Bone septa are formed due to enchondral ossification of cartilage. This raises the possibility of the presence of calcifications in the cancellous bone.
The metaphyseal areas of long tubular bones are most often affected:
- femoral (30%);
- shoulder (10-20%);
- tibial (15-20%).
Metaphysis (sometimes neck) is a small part of a tubular bone that is located between its epiphysis (head) and diaphysis (body). At 18-25 years of age, it stops growing and ossifies, which indicates the completion of bone formation.
Thus, articular exostosis is often observed - the formation of a growth on the upper (proximal) part of the tibia or lower (distal) part of the femur, i.e. the tumor is localized just below or just above the knee. Damage to flat bones, i.e. exostosis of the rib, scapula, pelvic bones, are less common. Osteochondromas of the bones of the fingers, toes, and clavicle are diagnosed even less frequently. The most rare occurrence is the formation of bone growths in the spine.
Also, bone exostosis can form on the lingual or buccal surface of the jaw. At the same time, it can take the form of a ridge, protrusion, mound, or take on bizarre shapes. In such cases, patients are advised to consult a dentist.
Diagnosis and treatment of epulis
Diagnosis of epulis comes down to collecting complaints, clinical examination, radiography and histological examination of the material.
The primary task in making such a diagnosis is to eliminate the provoking factor: professional cleaning of dental plaque, treatment of caries and its complications, replacement or correction of orthopedic structures according to indications. In fibromatous and angiomatous forms, dynamic observation is indicated, since after sanitation of the oral cavity and elimination of the causes of the disease, the tumor may decrease in size until it disappears completely.
Treatment of epulis is carried out surgically. The growth on the gum under local anesthesia or general anesthesia is excised with a scalpel or laser within the healthy tissue along with the periosteum. The second method is preferable, since the laser simultaneously coagulates the vessels and stops bleeding. With giant cell epulis, the area of bone tissue involved in the process is also removed. To do this, use a bur or cutter. The wound is closed with gauze with an iodoform mixture or a formed mucoperiosteal flap. If necessary, the material is sent for histological examination.
Intact teeth in the area of tumor localization must be removed with a high degree of mobility and severe exposure of the roots. If the bone lesion is extensive or epulis recurs, partial resection of the alveolar part along with the teeth is performed.
To speed up the healing of a fresh wound, the doctor prescribes compresses with medicinal ointments and rinses to the patient.
Exostosis in a child
It is in children that osteochondroma is most often first diagnosed, which is due to its formation from cells of the epiphyseal plate that is present only until the end of the growth period, which is adjacent to the metaphysis. It is also called the bone growth zone, since it is a hyaline cartilage whose cells are in constant miotic division. As a result, new chondrocytes (cartilaginous tissue cells) are formed, forming the epiphyseal plate, and the old ones are shifted to the metaphysis and subsequently replaced by osteoblasts (bone tissue cells).
In infants, violation of the rules for the prevention of rickets, in particular excessive use of vitamin D preparations, increases the likelihood of the formation of exostoses.
After puberty, the growth plates gradually close and are replaced by bone tissue, transforming into a thin epiphyseal line. If hormonal imbalances occur during this period, it is possible that the growth zones may remain open, which creates the preconditions for the formation of osteochondromas.
Usually, until the age of 7-8 years, bone exostosis does not manifest itself in any way in a child and makes itself felt only during the period of intensive growth, i.e., at 8-16 years, since it also begins to grow actively. In young children, such growths are present in the metaphysis area immediately near the epiphyseal plate, but subsequently move away from it and approach the diaphysis. Therefore, by how far the bone exostosis in children is from the epiphysis, the time of its formation is determined.
The growth of the neoplasm continues until the end of the growth period.
GENERAL VIEW
Exostosis of the oral cavity is the proliferation of bone and cartilage tissue in a certain area of the jaw row. Visually, it looks like a lump or nodule that tends to grow rapidly.
The sharp edges of the hardened cartilage tissue that forms exostosis can damage the mucous membrane covering it, leading to injury and severe pain, making it difficult to open the mouth and eat.
On the upper jaw, exostotic formations are most often localized in the area of masticatory elements on the outer or inner side of the row. When the lower jaw is affected, growths form at the base of the incisors, canines and premolars.
As a rule, cartilaginous growths have a benign structure, but there are known cases of their transformation into malignant neoplasms.
Types and stages of development
Exostosis can be present only on one bone, i.e., be solitary, or affect all metaphyses of the bones of the skeleton. In the second case, they talk about a generalized form of the disease, which is more common in men and is mainly hereditary. It is also called multiple exostotic chondrodysplasia. In this case, several bones or the vast majority of them are affected, but the formations have different shapes and sizes.
Depending on the shape and direction of growth, there are:
- hilly;
- linear;
- spherical exostoses.
Single exostoses have a narrow or wide base, while multiple ones are usually spherical or oval growths measuring 2-12 cm, sometimes more.
In its development, any osteochondroma goes through 3 successive stages:
- the formation of cartilaginous exostosis, which is not determined by palpation (palpation);
- ossification and active growth of growth;
- stopping the growth of the bone part of the neoplasm while maintaining the possibility of increasing the size of the cartilaginous cap.
Bone exostoses can already be felt during examination and can lead to discomfort, pain during physical activity and other symptoms.
Based on the nature of development and clinical picture, osteochondromas are divided into the following types:
- With normal growth rate. The osteochondral formation grows slowly, and there is a correspondence between the growth rate of the cartilage and the affected bone. Such osteochondromas have the most favorable prognosis, since after the end of the growth period they do not tend to continue to grow and almost never become malignant.
- With a high growth rate. An increase in the size of the growth occurs due to the proliferation of cartilage tissue and can also continue after the completion of the formation of the skeleton due to the preservation of the growth zone. In such cases, removal of exostosis is indicated, since there is a fairly high risk of malignancy.
- Malignant exostosis has the most unfavorable prognosis. Most often, osteochondral neoplasms of the ribs, pelvic bones, scapula and spine degenerate into chondrosarcoma or osteogenic sarcoma.
Indications and contraindications for removal of exostoses in dentistry
Indications
- Progression of growth, increase in its size;
- Pain in the patient;
- Feeling of discomfort in the oral cavity;
- The appearance of a cosmetic defect;
- Upcoming orthopedic treatment (prosthetics).
Contraindications
- Diseases that are characterized by blood clotting disorders;
- Diabetes;
- Pathological conditions of the thyroid gland and adrenal glands.
They are all common; There are no restrictions associated with the dental system.
Causes of exostosis
There is still no consensus on the reasons for the appearance of exostoses. A number of authors believe that they are of a tumor nature. But most agree that they are a consequence of disorders of enchondral ossification processes that arise as a result of dysembryogenesis (disorders of embryonic development). Therefore, today the main theory of the formation of bone exostoses is the displacement of the epiphyseal plate during intrauterine development of the fetus. It is a bone growth zone located directly below the epiphysis and is responsible for its lengthening. Therefore, the disease is considered congenital, and its development continues throughout the entire period of growth.
The following can increase the risk of osteochondroma:
- ionizing radiation (in 10% of cases the disease develops in patients who underwent radiation therapy in childhood);
- disturbances in the functioning of the endocrine system, taking hormonal drugs;
- smoking and alcohol abuse of parents.
The disease can also be hereditary and transmitted to the child from one of the parents. Especially often, multiple bone lesions due to exostoses are genetically determined.
The acquired nature of the disease cannot be ruled out. The following can provoke the appearance of neoplasms:
- bone injuries;
- microtraumas caused by excessive physical activity, which is typical for professional sports;
- infectious diseases and chronic inflammatory processes of any localization (for example, a heel spur often develops against the background of plantar or plantar fasciitis);
- pathologies of the periosteum, degenerative-dystrophic diseases of cartilage, ankylosing spondylitis;
- microcirculation disorders in soft tissues;
- muscle dystrophy;
- obesity;
- severe forms of allergic diseases;
- compression of the limbs, including an incorrectly applied plaster cast or tourniquet.
Wearing improperly selected clothing and shoes, in particular frequent hypothermia of exposed areas of the body, increases the risk of developing bone tumors.
Of particular importance in the development of osteochondroma is hormonal imbalance in children during puberty. Often the formation of bone exostoses is observed against the background of increased synthesis of sex hormones in adolescents. This can provoke the growth zones to remain open, which can subsequently cause gigantism. Also, an increase in the size of osteochondral exostoses can continue after the closure of growth plates in women as a result of hormonal changes.
Symptoms
The clinical picture depends on the form of the disease, location, size, shape of exostoses, and the degree of their influence on surrounding tissues. Single neoplasms are usually immobile and their growth is slow. Therefore, in most cases they are asymptomatic and there is no pain. The condition of the skin with solitary exostoses is usually not changed.
But in some cases, there is active growth and acquisition of large osteochondromas. They can mechanically compress blood vessels, nerves, and joints passing near them and provoke the development of reactive bursitis and myositis. This is accompanied by the appearance of pain of varying severity, swelling, redness of the tissues, and sometimes a feeling of numbness. If joint exostosis is present, the range of motion may be limited.
What symptoms exostosis will have depends largely on its location. With multiple exostoses, often the first signs of the disease are stunted growth, valgus deformity of the knee joints and clubhandedness. Fractures of the osteochondroma pedicle may also occur.
Surgical removal of exostosis on the gums
The operation is performed by a dental surgeon. In many cases, local anesthesia is sufficient for pain relief. It is possible to use deep sedation or anesthesia, especially if there are many osteophytes and they are large.
Amputation of bone growths is carried out in stages:
- local or general anesthesia:
- antiseptic treatment of the oral cavity;
- gum incision to access the correction area;
- amputation of a lump with a chisel or laser;
- grinding with a drill until the bone is smooth;
- repeated antisepsis;
- suturing and bandaging.
The operation time depends on the clinical case. It can range from 40 minutes to 2 hours. When using local anesthesia, the patient can go home immediately after the bleeding stops.
Exostosis of the knee joint
It may be caused by the formation of a growth at the end of the tibia and or femur. Exostosis of the tibia provokes severe deformation of the knee joint and is easily detected with the naked eye. Upon palpation, it is possible to detect a dense but painless formation under the skin, which can be either smooth or rough. Reaching large sizes, it provokes pain in the knee when walking (especially often in women who tend to wear high-heeled shoes). In this case, exostosis of the joint tends to injure the adjacent soft tissues, which provokes the development of tendonitis (inflammation of the tendons) and bursitis (inflammation of the synovial bursa).
Damage to the femur in the early stages of development is asymptomatic. But when the tumor reaches a large size, pain in the thigh and dysfunction of the affected limb may occur. Often there are many areas of deformation up to the covering of its entire surface. Since the femur is located deep in the soft tissues, it is difficult to detect exostoses during palpation.
Exostosis of the calcaneus (calcaneal spur)
This is a well-known type of osteochondroma. The growth can take on different shapes, which determines the characteristics of the symptoms that arise. With a spherical or mushroom-shaped neoplasm, after it reaches a size of 3-4 cm, pain appears when walking and the inability to fully step on the foot. Since the growth is located in an area that is constantly subject to friction from shoes, the skin in its projection gradually becomes coarser and thickens. A characteristic symptom is an increase in pain in the morning and a gradual decrease in its severity during the day. In the evening, swelling of the lower extremities is often observed.
Spinal exostosis
The lesion can occur at any level, but the thoracic region is most often affected. The neoplasm is located in the area of the arches or processes of the vertebrae. It can grow towards the vertebral or spinal canal or in an anterior direction. The first option is more dangerous, since it is capable of mechanically compressing the spinal cord and the nerve roots extending from it. This provokes the development of the so-called radicular syndrome with sharp, severe pain, radiating in accordance with the level of damage to the body part, impaired sensitivity and mobility.
Exostoses of the ribs
The formation of growths on the ribs is more often observed with curvatures of the spine, which also lead to deformation of the chest. Their growth causes fixation of the pathological position of the chest and limitation of the vital volume of the lungs. As a result, respiratory function disorders may occur, which provokes the appearance of signs of hypoxia (oxygen starvation). To a greater extent, the lack of oxygen affects the brain, which can be accompanied by dizziness, headaches and other disorders. The heart, liver, spleen, and other internal organs are also sensitive to changes in the gas composition of the blood.
Exostosis of the humerus
The humerus is one of the most common sites of osteochondroma. During its formation, the following may be observed:
- dull pain in the shoulder area that occurs when moving the arm with a large amplitude;
- a feeling of stiffness in movements, present mainly in the morning, until you manage to warm up;
- limited mobility of the upper limb in the shoulder;
- dystrophy of the muscles of the shoulder and forearm, which in difficult cases can be seen with the naked eye.
Complications
Cartilaginous exostosis in children has a dangerous negative impact on the condition of the growth plates, which can result in shortening of the lower leg, thigh, forearm, shoulder, etc. This can also cause curvature of the arms and legs, increase the risk of fractures and cause disability.
Patients with severe forms of the disease feel inferior, which negatively affects their mental and emotional state.
The most dangerous complication of osteochondroma is its malignancy, i.e. transformation into a malignant tumor - chondrosarcoma. The highest risk of malignancy is with multiple exostoses. In this case, growths localized in the pelvic bones are more likely to undergo malignancy. Less commonly, exostoses of the ribs, scapula, and spine turn into malignant neoplasms. Single osteochondromas transform into a malignant tumor in no more than 1% of cases.
Atypical growth can be observed in any part of the exostosis: the cartilaginous cap, at the base or in the middle part.
General information
Osteochondroma of bone (synonymous with osteochondral exostosis) is a benign exophytic osteochondral formation, which is located on the outer surface of the bone and consists of a bone base, covered on top with cartilaginous tissue (the so-called cartilaginous cap). It is one of the most common skeletal tumors, accounting for about 20% of all human bone tumors and almost 40% of the totality of benign tumors ( chondroma , osteoma , osteoblastoma , chondroblastoma , osteoid osteoma , etc.).
Morphologically, osteochondroma is a spongy bone with a cortical layer, which is covered with articular-like cartilage, the thickness of which does not exceed 1 cm, and can be attached to the bone with a pedicle or a wide base; the cartilaginous covering of the subchondral endplate is not separated from the underlying bone (Fig. below). In this case, there is a violation of the processes of resorption, remodeling of physiological regeneration of bone tissue, which characterizes pycnodysostosis .
This type of tumor is most common in children and young people (up to 20 years) in whom epiphyseal bone growth has not yet been completed. The focus of osteochondroma can occur anywhere in the skeleton, however, in most cases it is localized in long tubular bones (femur, humerus, tibia), affecting their metaphyseal sections, and the favorite localization is the upper part of the tibia or the lower part of the femur. The approximate incidence of tumors in various bones of the skeleton is: in the femoral part of the leg about 30%; shin bones 15-20%; in the humerus 10-20%. The remaining bones of the skeleton (scapula, collarbone, spine, ribs, pelvic bones, etc.) are affected much less frequently.
Exostoses are quite common in dentistry. Most often, ecostoses in the oral cavity are localized in the area of the alveolar process from the buccal surface or the body of the jaw in the form of tubercles, blunt ridges and protrusions. Exostosis of the gums occurs more often after tooth extraction, trauma, or due to age-related changes in the alveolar ridge. Exostoses of the mandibular bone are most often located on the lingual side in the area of premolars and much less often in the area of molars, incisors and canines. They manifest themselves in the form of a tubercle or ridge, a process, and if they are large in size, they may require not only their removal, but also restoration of the gums (Fig. below).
Osteochondral exostosis in children at the beginning of development is located on the side of the metaphysis near the epiphyseal-cartilaginous plate, and exostosis in older children is located closer to the diaphysis and based on the distance of the exostosis from the epiphysis of the bone, one can judge the timing of its appearance. The growth of most exostoses continues, as a rule, until the onset of synostosis of the epiphysis with the metaphysis (until the end of skeletal growth). ICD-10 code: D16 (benign neoplasms of bones and articular cartilage).
This osteochondral formation can be either solitary (single) or generalized in the form of multiple exostoses. Solitary osteochondromas can have a narrow or wide base, and with multiple lesions, all bone metaphyses are involved in the pathological process in the form of an ovoid/spherical formation, the sizes of which vary widely (from 2 to 12 cm or more), sometimes reaching a large size. This type of tumor is more common in males, and there are cases of family predisposition to the appearance and development of multiple exostoses. At the same time, multiple exostotic osteochondrodysplasia is inherited in an autosomal dominant manner and manifests itself in patients under 20 years of age.
Due to the effect of the tumor on the growth zones of long bones, exostosis can lead to significant shortening of the segments of the lower/upper limb, curvature of the arms/legs, fractures of the extremities and cause early disability of the patient, and the constant experience of one’s inferiority negatively affects the mental and emotional state of patients.
The most dangerous complication of osteochondroma of the bone is the potential for its malignant transformation, usually into chondrosarcoma. At the same time, atypical growth can manifest itself both in the area of the cartilaginous cap of the exostosis tumor, and in the middle part or at the base of the tumor.
Malignancy of exostoses is more common (72%) in patients with multiple forms of exostotic chondrodysplasia, and the prevailing localization of exostoses with atypical growth is predominantly the pelvic bones, less often the ribs, scapula, and spine.
Diagnostics
Diagnosis of bone exostoses is not difficult. If these symptoms occur, you should consult an orthopedist. Based on the patient’s complaints, medical history and examination results, the doctor can already assume the presence of a neoplasm.
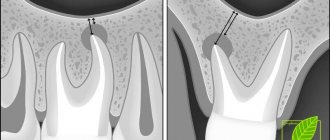
To clarify its size and other features, radiography is prescribed. It is carried out in 2 projections. Osteochondroma on x-rays is visualized as a shadow with smooth, clear contours and a pedicle or wide base connected to the bone. If there is no calcification in the cartilaginous layer, it will not be visible on x-ray.
To obtain additional data, the following may be assigned:
- CT scan, which makes it possible to detect the presence of bone marrow contents in exostosis and trace its connection with the medullary canal of the affected bone;
- MRI, which provides accurate data on the thickness of the cartilage cap and thereby clarifies the nature of the neoplasm (malignant tumors are characterized by a thickness of the cartilage tissue covering them of more than 2 cm).
If there is a suspicion of the development of oncology, patients are advised to undergo a biopsy - taking a fragment of exostosis for histological examination. In this way, benign osteochondroma is differentiated from malignant neoplasms.
If exostoses are detected in childhood and adolescence, it is imperative to conduct a full endocrine examination and determine the content of all significant hormones in the blood.
Diagnosis of exostosis after tooth extraction or injury
In order to make a correct diagnosis, CELT dentists:
- listen to the patient’s complaints and collect anamnesis;
- conduct a dental examination;
- The patient is prescribed an x-ray.
Examination reveals the presence of a dense formation that is not fused to the soft tissues. The mucous membrane over it is thinned and can be damaged by the sharp edges of the destroyed units. The x-ray image clearly shows a protrusion with clear boundaries. Jaw osteophytes must be differentiated from bone tumors of benign or malignant etiology.
Treatment of exostoses
When diagnosing exostosis, treatment is prescribed only when symptoms appear. Otherwise, dynamic monitoring of the tumor is sufficient. If the tumor bothers the patient, depending on its type, the nature of the manifestation of osteochondroma, conservative treatment is selected or surgical intervention is prescribed. But the main method of treating exostosis is surgery.
Conservative, i.e., non-surgical, therapy is indicated mainly for exostosis of the calcaneus and rib, but only in the early stages of development. First of all, the use of special orthopedic insoles, made individually, and the replacement of regular shoes with models with offset edges are prescribed. This helps eliminate mechanical pressure on the tumor, reducing the load on the Achilles tendon and calcaneal tubercle.
If severe pain and inflammation occur, drug therapy is prescribed, including:
- NSAIDs in the form of topical agents (Nimid, Dolaren, Ketoprofen, Voltaren);
- drug blockades with the introduction of a mixture of anesthetics and corticosteroids (performed for severe pain that cannot be eliminated by other means).
Courses of physiotherapeutic procedures are also indicated. Shock wave therapy (SWT) is the most effective. It involves the impact of infrasonic acoustic waves on the affected area. The mechanism of action of the method is based on the cavitation effect that occurs at the interface between media. The acoustic resistance of soft tissue is less than that of bone. Therefore, sound waves penetrate through them and affect bones and cartilage. This provokes an improvement in blood supply, restoration of normal cartilage tissue and bones, and a reduction in the size of tumors.
Additionally, we may recommend:
- electrophoresis with the introduction of anesthetics;
- ultrasound therapy;
- laser therapy;
- Ural Federal District;
- magnetotherapy.
Surgery to remove exostosis
Surgical intervention is indicated for:
- large size of osteochondroma and the presence of persistent pain;
- development of complications (tendinitis, bursitis, vascular, neurological disorders, etc.);
- bone deformations as a result of the growth of exostosis;
- fracture of the base leg;
- malignancy of the tumor.
For children with bone exostosis, surgery is prescribed only in extreme cases. As a rule, it is carried out only if the testimony remains after reaching adulthood.
But if there are contraindications, surgery is not performed. This:
- purulent-inflammatory processes in the area of the upcoming intervention;
- exacerbation of chronic diseases;
- decompensated form of diabetes mellitus;
- acute infectious diseases.
Treatment of exostosis with surgery involves its complete excision with capture of the cartilaginous cap. There are several methods for removing osteochondral growth. A specific one is selected based on the location of the osteochondroma and its size. Usually preference is given to marginal resection of the growth, i.e., its removal within healthy tissue. Only in some cases is it necessary to resort to corrective osteotomy with concomitant resection of osteochondroma, but the cost of removing exostosis in this way is higher, since the operation also corrects bone deformation.
After surgery, complete recovery is observed in 98% of cases. Therefore, almost everyone who has once removed an exostosis forgets about it forever.
Marginal resection is a relatively simple type of surgery. Its essence is to expose the affected bone and remove the entire neoplasm in the front of healthy tissue along with the surrounding capsule using a sharp chisel, drill, oscillating saw or bur. After removal of the pathological formation, curettage of the maternal bone is performed using cutters and bur. In some cases, the extent of resection can be large and create the need for bone grafting using autografts or special implants. It is important to remove the entire cartilaginous cap and neoplasm, otherwise a relapse may develop.
Carrying out a corrective osteotomy involves cutting the mother's bone using an osteotome and removing the osteochondroma. After this, the bone fragments are fixed in the desired position using special plates, screws or knitting needles.
Removal of exostoses in the oral cavity: features
If you have developed exostosis of the jaw, treatment comes down to the only correct method - its elimination.
During surgery, all excess bone or cartilage protrusions are removed and the surface of the oral cavity is smoothed. As a rule, general anesthesia is not required for the procedure. Local enough so that the patient does not feel the slightest discomfort. There may be several reasons why exostosis may form on the gum, tooth surface or palate:
- Individual characteristics in the structure of the jaw;
- Heredity;
- Consequences of injuries, bruises and falls.
Sometimes exostosis appears after tooth extraction - the photos clearly demonstrate the clinical picture: the bone tissue on the surface of the alveoli does not smooth out, thereby provoking the growth of the tumor.
Removal of osteochondral exostoses is not always a mandatory measure. However, it still has a number of indications.
- Large size of bone growths and excessive rate of their increase.
- Discomfort and pain due to the pressure of formations on the jaw.
- Formation of cosmetic defects.
- Planned prosthetics.
Rehabilitation
After removal of the exostosis, the patient remains in the hospital for 3 days, the sutures are removed on days 7-10. Performing marginal resection does not require any serious restrictions even in the early postoperative period. The patient can completely return to his usual lifestyle after the stitches are removed, and forget about exostosis immediately after the operation.
When performing a corrective osteotomy, complete bone fusion occurs after 6 weeks, but full recovery may require up to 3 months. At this time, it is important to strictly follow all the doctor’s recommendations and not to overload the operated part of the body. All patients who have undergone osteotomy are prescribed drug therapy, exercise therapy, and often physical therapy. The duration of rehabilitation in such cases depends on the type of surgical intervention performed and the individual characteristics of the patient.
Thus, osteochondroma is a very common type of tumor. At the same time, statistics on the frequency of its occurrence are not entirely objective, since exostoses often do not appear throughout a person’s life, and therefore are not diagnosed. However, if the formed formation bothers the patient, causes him pain, or reduces the quality of life, you should not hesitate to contact an orthopedist. A specialist will be able to assess the degree of danger of the tumor and, if necessary, remove it using the most gentle method possible.
Clinical manifestations of jaw exostoses
As a rule, they develop practically asymptomatically and unnoticeably for the patient, and are often diagnosed during the preparation and orthopedic treatment. Signs of exostosis after tooth extraction:
- Painful symptoms of aching nature (occurs if there is pressure on the nerve endings in the dental canals);
- A convex growth with a bumpy or smooth surface without pathological changes in the color of the mucous membrane above it;
- Impaired functioning of the jaw bone, inability to fully open the mouth (occurs if the joint is affected).