Sialadenosis is a non-inflammatory disease of the salivary glands, leading to enlargement and/or disruption of their function. The lesion is dystrophic in nature and is not associated with the appearance of tumors. Structural changes in gland tissue usually appear against the background of other systemic pathologies. Dentists quite often encounter this phenomenon: 1 case out of 10 pathologies of the salivary glands is represented by sialadenosis.
The disease usually occurs in middle-aged people. Since it often accompanies endocrine, allergic, dysmetabolic and other systemic diseases, the approach to treatment should be carried out not only from the dental side.
Types of sialadenoses
Based on the location of pathological changes, the following types of sialadenoses are distinguished:
- interstitial;
- parenchymal;
- ductal
Pathological areas can be located both in the tissues of the gland itself and in the ducts.
There are several stages based on severity:
- First. The salivary glands are of normal size and are faintly palpable.
- Second. There is a slight enlargement of the glands, which is not noticeable during visual inspection, but is palpable.
- Third. Enlargement of the glands, which is noticeable both during visual inspection and palpation.
According to the nature of origin, neurogenic, allergic, endocrine sialadenoses are distinguished, as well as nutritional ones - associated with dietary habits.
Ask a Question
Classification of sialadenoses
According to the state of the salivary gland, sialadenoses are defined as interstitial, parenchymal and ductal (depending on the predominant changes detected using private and special examination methods). This disease has three stages of development:
- initial (I degree), in which the salivary glands are not enlarged and have normal sizes;
- the stage of pronounced clinical changes (II degree) is accompanied by a slight increase in the size of the salivary glands, which is determined by palpation;
- late (III degree) is characterized by an increase in the size of the salivary glands, which is diagnosed both visually and by palpation.
In addition, sialadenoses are divided into endocrine, neurogenic, allergic and associated with nutritional disorders. In order to determine the degree of development of sialadenosis, a specialist assesses the size of the major salivary glands, taking into account examination and palpation data.
Why does sialadenosis occur?
Sialosis can develop against the background of underlying diseases or be caused by certain physiological reasons. For example, pathology occurs in women during pregnancy and lactation. Pathological changes are often provoked by autoimmune diseases - systemic scleroderma, rheumatism, psoriasis, etc., as well as metabolic and endocrine disorders.
Eating disorders that lead to sialosis include strict long-term diets and restrictions, and anorexia. In general, the most common causes are diabetes mellitus, menstrual dysfunction and thyroid dysfunction, chronic pancreatitis and other gastrointestinal pathologies.
The allergic nature of the disease may be associated with drug allergies. In some cases, sialosis of the salivary glands develops after surgery or trauma in the area of the dental system.
Reasons for the development of sialadenoses
Sialadenosis can be caused by both physiological reasons and the pathological condition of the patient, namely:
- pregnancy;
- breastfeeding;
- alcohol abuse;
- endocrine system disorders;
- diabetes mellitus;
- menstrual irregularities (hypermenstrual syndrome);
- prostatitis;
- chronic pancreatitis;
- autoimmune diseases (rheumatoid arthritis, systemic lupus erythematosus, scleroderma, psoriasis, Sjogren's disease, Mikulicz's disease, etc.);
- decreased nutrition due to anorexia nervosa.
Patients may also develop allergic sialadenoses when taking certain medications. Sialadenosis may occur after surgery on the salivary gland or after injury to it. The main and most common cause of sialadenosis in patients who suffer from alcoholism is liver cirrhosis. There are also frequent cases of the development of sialadenoses of unknown origin in patients who do not have any systemic diseases. In this case, the patient undergoes an examination to identify a general disease. The mechanism of development of this pathology in medical practice is not entirely clear. But in medicine there are such factors for the manifestation of this disease as:
- neuropathy, which is accompanied by the destruction of nerve fibers;
- disturbances in the microcirculatory system and lipid oxidation, which leads to damage to cell tissue;
- congenital expansion and violation of the architectonics of the ductal system.
These processes cause functional failure and replacement of glandular tissue with adipose tissue.
Symptoms of the disease
Sialosis most often affects the parotid glands, rarely - the submandibular and sublingual glands. Usually we are talking about a bilateral pathological process. The picture of the disease is nonspecific - painful swelling appears in the area of the affected glands, their increase in the 2nd and 3rd stages. The increase persists over time.
One of the manifestations of the disease is dry mouth. This is due to the fact that salivation during illness may be insufficient.
During the examination, the doctor will determine the characteristic swelling of the soft tissues. Palpation does not cause severe pain; sometimes discomfort or mild pain appears. The nearby lymph nodes are not changed, and there are no restrictions in opening the mouth. During a massage of the salivary gland, clear saliva is released without external features.
It is worth noting that specific symptoms may accompany sialosis, occurring with decreased or increased salivation without an increase in the glands themselves. For example, this is observed with stomatitis, duodenal ulcers, parasitosis, neurasthenia, etc.
Symptoms of sialadenoses
Typically, during the development of sialadenosis, patients experience swelling in the area of the salivary glands, which is not accompanied by pain. The enlargement of the salivary glands persists for a long time; their size does not change when eating. With sialadenosis, salivation is often reduced. When examining the patient, a moderate amount of squamous epithelium is observed in the secretion and a change in the configuration of the face, which is caused by symmetrical swelling of the soft tissues. In this case, the enlarged glands have a dense shape to the touch, with a smooth surface. In turn, the manifestation of parenchymal sialadenosis is accompanied by dilation of the excretory ducts. A relative sign of interstitial sialadenosis is narrowing of the excretory ducts. Ductal sialadenosis is accompanied by a stricture of dilated ducts. Sometimes disturbances in the excretory and secretory functions of the salivary glands occur without their visible increase. These conditions are also classified as sialadenoses as a reaction of the parenchyma to various changes in the body: they are manifested by increased or decreased salivation. An increase in the secretion of the salivary glands (hypersalivation) is associated with diseases such as stomatitis, gastric and duodenal ulcers, helminthiasis and even toxicosis during pregnancy. Reduced secretion (hyposalivation) leads to dry mouth, or more precisely to xerostomia. The symptom of dry mouth is often observed in patients with various diseases of the salivary glands and body systems.
Diagnostic features
Examination of a person with suspected sialadenosis may include the following methods:
- survey, examination, palpation of the glands;
- laboratory tests - general and biochemical blood tests, clinical urine tests, assessment of carbohydrate metabolism (glucose test);
- Ultrasound of the salivary glands and soft tissues is necessary to confirm the non-inflammatory nature of the disease and exclude tumors.
It is important for the doctor to exclude other possible pathologies characterized by enlargement of the salivary glands: inflammatory diseases, infectious diseases, cysts and tumors, the formation of calculi (stones).
Sialography is prescribed to determine dilated or narrowed salivary ducts; it involves the administration of a contrast agent. A radiosialogram may also be required to assess the secretory capacity of the glands. Using a CT scan, the doctor can see a bilateral increase in tissue size and density and rule out malignant and benign formations.
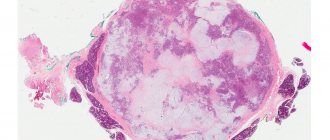
As an additional method, sialometry, cytological studies of secretions (salivary fluid), as well as biochemical studies of saliva can be used. The final diagnosis can be made after aspiration or another type of gland biopsy. Histological study allows us to establish dystrophic changes.
To find out the exact cause of the disease, it is important to assess your overall health. Therefore, the patient often needs to be examined by another specialist: an endocrinologist, gynecologist, urologist, allergist, etc. In some cases, the involvement of a rheumatologist is required.
Diagnosis of sialadenoses
During the examination of a patient with suspected sialadenosis, the doctor conducts a survey, examination and palpation of the salivary glands. After which the patient undergoes clinical and biochemical blood and urine tests to study the parameters of carbohydrate metabolism. In order to exclude the inflammatory and tumor process of changes in the salivary glands, the patient undergoes an ultrasound of the salivary glands. This makes it possible to determine their increase, heterogeneity of the parenchyma, increase or decrease in echogenicity. In addition, an X-ray examination is performed. With sialography, the patient can detect dilation or narrowing of the salivary ducts, slowing down the removal of the radiocontrast drug from the gland. A radiosialogram also reveals a decrease in the secretory ability of the salivary glands. In order to detect a bilateral increase in the volume and density of the gland and thereby exclude tumor lesions, the patient undergoes a computed tomography scan.
In addition, to diagnose sialadenosis, sialometry, cytological examination of duct secretions and biochemical examination of saliva are performed. The diagnosis of sialadenosis is confirmed by aspiration or incisional biopsy of the salivary glands. Histological examination reveals an increase in the acini in the patient, the presence of dystrophic changes in them, and the absence of inflammatory infiltration.
In order to determine the nature of the diseases accompanying sialadenosis, the patient may be referred for consultation to specialists. As part of diagnostic measures, other possible causes of enlargement of the salivary glands are excluded: sialadenitis, mumps, tumors and cysts of the salivary glands, stones of the salivary glands.
Treatment methods
Treatment of sialadenosis is a multi-step process. The main condition is effective therapy for the underlying or concomitant disease, although this will not help solve the problem completely. Symptomatic therapy is possible using novocaine blockades. Physiotherapy will help cope with unpleasant symptoms; electrophoresis, galvanization, magnetic and laser therapy are widely used. The impact is carried out on the area of the cervical nerve tissue in order to improve the conductivity of impulses.
Drug therapy consists of the use of vitamin E, drugs to stimulate salivation, as well as colloidal solutions to correct blood viscosity and improve blood flow in small blood vessels. Surgical treatment may be indicated in the absence of a positive response to conservative therapy. It consists of partial or complete removal of the salivary gland or its duct.
Treatment methods for sialadenosis
Treatment of sialadenosis is quite difficult, since various therapeutic measures aimed at reducing the size of the glands are not always successful. However, for the symptomatic treatment of sialadenosis, methods such as:
- acupuncture;
- courses of novocaine blockades to inhibit the increased tone of the sympathetic nervous system.
Physiotherapy methods are also used in the treatment of sialadenosis, namely:
- novocaine electrophoresis;
- galvanization in the area of the salivary glands and cervical sympathetic ganglia;
- pulsed magnetic therapy;
- laser therapy on the area of the salivary glands;
- galvanic collar;
- infiltration of the subcutaneous base of the parotid glands with weak solutions of novocaine;
- hyperbaric oxygenation.
The treatment method for sialadenosis also includes oral and parenteral medications and vitamin E, as well as intravenous administration of rheopolyglucin and hemodez solutions. In the absence of satisfactory results of conservative therapy, surgical treatment may be indicated. The prognosis and prevention of sialadenosis depend entirely on the underlying disease.