As a result, changes occur in the spine, in the abdominal and back muscles and the shape of the lumbar curve of the spine (hyperlordosis), and all this becomes relaxed. Poor posture and poor muscle tone can also affect spinal mechanics.
The lumbar curve of the spine begins to slowly increase as the pelvis begins to move backward. This posture begins to affect weakened muscles and leads to the accumulation of fatigue in the lower back muscles. A woman may initially experience mildly painful muscle spasms, which may be the first sign of the possibility of persistent lower back pain as her pregnancy progresses. The growing uterus shifts the center of gravity and weakens the abdominal muscles, changes posture and puts excess stress on the back. If the uterus affects the nerves, this can lead to pain. In addition, excess weight during pregnancy increases the stress on muscles and joints, and therefore, by the end of the day, a pregnant woman may feel discomfort.
Experts describe the two most common patterns of low back pain during pregnancy: low back pain, which occurs in the lumbar vertebrae in the lower back, and posterior pelvic pain, which is felt in the back of the pelvis. Some women have symptoms of both types of low back pain.
Lower back pain is similar to the pain a woman experienced before pregnancy. The pain is felt in the lower back and around the spine, approximately at waist level. Women may also experience pain that radiates to the legs. Sitting or standing for a long time can increase the pain and, as a rule, the pain tends to intensify towards the end of the day. Many more women experience posterior pelvic pain, which is felt less than lower back pain. The pain may be located deep inside the buttocks, on one or both buttocks, or in the back of the thighs. Pain may be triggered by activities such as walking, climbing stairs, getting in and out of the bathroom on a low cabinet, turning over in bed, or twisting and lifting heavy objects.
Positions that involve bending the torso, such as sitting in a chair and working at a desk while leaning forward, can worsen posterior pelvic pain. Women with posterior pelvic pain are also more likely to experience pain over the pubic bone.
When lower back pain radiates to the buttocks and thighs, sciatica is often suspected - although sciatica is not very common in pregnant women. True sciatica, which can be caused by a herniated disc or a bulging disc in the lumbar spine, occurs in only 1 percent of pregnant women.
If there is compression and inflammation of the sciatic nerve (disc herniation), then the pain in the legs is more severe than with ordinary lower back pain. The pain can be felt not only in the hip, but also below the knee or even radiate to the foot. There may also be sensory disturbances such as numbness or tingling sensations.
With severe lumbosacral radiculitis, there may be numbness in the groin area, as well as in the genital area. You may also have problems urinating or defecating. If a pregnant woman suspects radiculitis, she should definitely consult her doctor. If symptoms such as loss of sensation in the legs and weakness in one or both legs, or loss of sensation in the groin area and difficulty urinating or defecating, then you should consult a doctor immediately! Such symptoms may be evidence of the development of cauda equina syndrome in the presence of a disc herniation in a pregnant woman, and in such cases emergency surgery is necessary.
Introduction
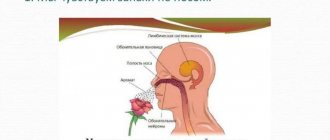
Migraine is a common primary form of headache (TH), which manifests itself in the form of repeated attacks, often accompanied by nausea, vomiting, photo- and phonophobia.
The prevalence of migraine, according to various estimates, ranges from 2.6% to 21.7%, and the average rate is 14.7% [1]. In Russia, the prevalence of migraine reaches 20.8%, which is approximately more than 30 million people [2]. The prevalence of migraine in women is more than 2 times higher than that in men, and the highest prevalence of migraine within the female population occurs during reproductive age [3]. For this reason, issues of tactics for managing patients with migraine during pregnancy are of high relevance. Issues of pregnancy planning, as well as rules for taking medications for pain relief and approaches to preventive treatment of migraine during pregnancy are discussed very often.
2nd trimester screening
Health control is extremely important for the expectant mother. Regular examinations and tests prescribed by the doctor are necessary to ensure that the pregnancy is proceeding normally and the child is developing correctly.
This is the purpose of the second screening during pregnancy. The optimal time for its completion is in the 18th week, the recommended time interval is from the 17th to the 20th week. During screening, a woman will need to undergo blood and urine tests and an ultrasound. Doctors focus on:
- hormonal examinations;
- monitoring the function and condition of the kidneys;
- hemoglobin level in the blood to eliminate the risk of iron deficiency anemia;
- anatomical ultrasound examination of the fetal anatomy.
“In the first trimester, we do an analysis of the level of glucocorticoid hormones,” explains Evgeniy Petreikov. — In the second, we take this hormone again and look at the dynamics. If abnormal glucocorticoid levels are detected, replacement therapy should be prescribed as early as possible to reduce the risk of developmental delays, late miscarriage and premature birth.”
To exclude the risk of developing diabetes mellitus in pregnant women, a glucose tolerance test is performed from the 24th to the 28th week. Even if a woman has no prerequisites for developing the disease, she still needs to be examined. The expectant mother is asked to drink a glucose solution and blood is taken after an hour and two hours. Based on the obtained blood glucose levels, a “sugar curve” is constructed. If it passes above normal values, gestational diabetes mellitus is diagnosed. It requires mandatory monitoring by doctors and the woman herself.
pixabay.com/
The course of migraine during pregnancy
In 50–70% of women during pregnancy, migraine without aura improves [4]. Migraine attacks become mild, extremely rare, and in most patients in this group the migraine completely disappears. Improvement occurs after the first trimester, starting from the 12th–14th week. pregnancy. This is due to the fact that by the beginning of the second trimester, the level of estrogen stabilizes and begins to increase, and its fluctuations stop (Fig. 1). Migraine with aura stops less often during pregnancy, in approximately 40% of patients.
At the same time, if headache persists during this period, it is necessary to carry out differential diagnosis and determine the form of headache. Alarming symptoms during pregnancy are:
the appearance of a new, unusual headache;
a sharp increase in migraine attacks;
the addition of new, unusual symptoms of hypertension, including visual impairment, sensitivity, aphasia, paresis of the limbs;
the appearance of migraine aura in patients with previous migraine without aura;
increased blood pressure during hypertension;
convulsions.
The presence of active migraine during pregnancy does not affect the course of pregnancy itself and the development of the fetus, but increases the risk of preeclampsia and gestational hypertension. Moreover, the persistence of active migraine, especially migraine with aura, during pregnancy increases the risk of acute cerebrovascular accidents (ACVA) by 15–17 times [5]. The prevalence of stroke during pregnancy and the early postpartum period is 34.2 cases per 100,000 births [5].
Stopping attacks
The selection of drug therapy for patients with migraine during pregnancy poses significant difficulties. The severity of migraines can be especially high during the first trimester. Full-blown, unrelieved migraine attacks are often accompanied by nausea, vomiting and lead to unnecessary suffering and dehydration, especially in patients suffering from early toxicosis. Despite the desire to avoid taking medications (especially in early pregnancy) to minimize the risk of fetal developmental disorders, many patients with hypertension begin to take analgesics uncontrollably. Therefore, the importance of preliminary counseling and education of patients on the proper control of hypertension cannot be overemphasized.
Non-pregnant women are recommended to take medications to relieve migraine attacks as early as possible, no later than 1 hour after the onset of the attack. This approach allows you to speed up relief and completely stop a migraine attack in a short time. Pregnancy is the only period in a woman’s life when this recommendation can be temporarily ignored. For patients seeking to minimize drug use, a stepwise approach may be recommended, in which treatment of mild to moderate attacks begins with non-drug methods.
If the patient decides not to use analgesics, control of nausea becomes a priority to avoid dehydration. Patients should avoid strong odors and drink more fluids, such as juices diluted 1:1 with water. Feelings of nausea can also be reduced by eating easily digestible foods, such as crackers, applesauce, bananas, rice, and pasta. Metoclopramide or ondansetron can also be used [6].
Neurostimulation methods play a major role in non-drug approaches to the treatment of migraine. The only device registered in Russia for non-invasive transcutaneous stimulation of the supraorbital nerve - Cefaly (Cefaly®) - is specially designed for the treatment of migraines and can be a good alternative to medications for relieving migraine attacks. Using the Cefaly device at the very beginning of an attack allows you to reduce the intensity of headaches and in some cases completely stop the attack. Thus, the intensity of migraine pain decreases by 4.3 points after 1 hour [7]. Cefaly can also be used in conjunction with pain medications to increase their effectiveness.
Despite the fact that, in general, paracetamol is less effective for relieving an acute attack of migraine than acetylsalicylic acid and nonsteroidal anti-inflammatory drugs (NSAIDs), its safety during pregnancy is higher [6]. Caffeine, which has the ability to enhance the analgesic effect, is an important addition to painkillers. Adding 100 mg of caffeine to the analgesic increases its effect by 1.5 times.
The safety of NSAIDs is controversial [6]. Prescribing NSAIDs in the first trimester may be associated with an increased risk of miscarriage and the development of congenital anomalies. Taking NSAIDs and aspirin in the third trimester can lead to premature closure of the ductus arteriosus
. For these reasons, the use of NSAIDs should be limited to the second trimester. It is especially important to stop taking them after the 32nd week. Taking high doses of aspirin may also increase the risk of bleeding.
Triptans are the most effective analgesics for the relief of migraine attacks. The safety of triptans during pregnancy is assessed through pregnancy registries, where a huge amount of data has now been accumulated for sumatriptan, for example. Despite the prohibition of its use during pregnancy indicated in the official instructions for the use of sumatriptan, there is no evidence of an increased risk of congenital malformations when taken by pregnant women [8]. Patients who took triptans in early pregnancy (without knowing they were pregnant) should be advised that the likelihood of adverse effects of this drug on the fetus is extremely low. Women who experience severe, disabling migraine attacks that cause vomiting may be advised to use triptans during pregnancy. To date, this information has not been included in official recommendations for the treatment of migraine, but the safety of sumatriptan is confirmed by the analysis of a huge number of observations and expert recommendations.
It should be borne in mind that the safety of triptans varies. Sumatriptan, as the most hydrophilic of the triptans, has difficulty penetrating the placental barrier, while other triptans (including eletriptan) are lipophilic.
Prednisolone can only be used as an “ambulance” remedy in the event of a prolonged and severe migraine attack [9]. The use of prednisolone is preferable to dexamethasone, since the latter penetrates the placenta better. Nuchal nerve blocks with lidocaine, bipuvacaine and/or a corticosteroid can be used as an ambulance to relieve severe attacks.
Preventative treatment
The attending physician must promptly identify the group of patients in whom preventive treatment of migraine will be most successful. While most pregnant women begin migraine remission at the end of the first trimester, others experience migraine remission by the 10th–12th week. Frequent attacks may persist, which will most likely indicate the persistence of headache throughout pregnancy. Refusal to treat such patients can lead to malnutrition, dehydration, the development of affective disorders and a significant decrease in quality of life.
Preventive treatment of migraine is necessary in the following cases:
high frequency of attacks (more than 3 days a week);
the presence of severe or prolonged attacks;
significant disability;
dehydration and malnutrition;
poor response to analgesics.
The current frequency of headaches and the effectiveness of the analgesics used should be monitored using a headache diary. For patients who require preventive treatment, it is necessary to select the optimal combination of drug and non-drug approaches.
There are a number of non-drug methods that can effectively manage hypertension during pregnancy and are an important addition to pharmacological methods; when combined, the amount of drugs used during pregnancy and lactation is reduced. Relaxation techniques, cognitive behavioral therapy and biofeedback can be used during pregnancy.
Trigeminal neurostimulation also plays a major role in the preventive treatment of migraine during pregnancy. Regular use of Cefaly daily for 20 minutes, preferably in the evening, leads to a 2-fold reduction in migraine headache attacks in 38% of patients with episodic migraine and 35% of patients with chronic migraine [10, 11]. The high safety of this method (the probability of adverse events is 2–3%) allows it to be used without fear during pregnancy. It is also important that the Cefaly device has a mild sedative effect [12] and is not prohibited for use during pregnancy.
Information about the safety of drugs is collected through clinical trials of their use in the treatment of other diseases, including mood disorders, cardiovascular diseases and epilepsy. The safety of most drugs during pregnancy has not been directly assessed, but accumulated data have allowed these drugs to be assigned a certain safety category. In addition, the choice of drugs for the treatment of migraine in pregnancy may be based on additional information about the safety of a number of drugs that are used in pregnancy to treat hypertension, depression and epilepsy.
If it is necessary to prescribe drug therapy to reduce migraine attacks, it is recommended to start with the use of β-blockers. Due to its widespread use in the treatment of arterial hypertension during pregnancy, propranolol (anaprilin) is considered the drug of first choice for the preventive treatment of migraine [13]. At the same time, taking β-blockers is associated with a risk of hypoglycemia, hypotension, bradycardia and respiratory disorders in the newborn. The drug should also be used with caution in patients with bronchial asthma, a tendency to arterial hypotension and bradycardia. In the absence of propranolol or if there are contraindications to it, metoprolol can be used. It is recommended to gradually reduce the dose of beta-blockers during the last weeks of pregnancy (starting from the 36th week) and discontinue them at least 2-3 days before delivery.
No adverse effects on fetal development have been demonstrated with the use of calcium channel blockers, but insufficient data and the low effectiveness of verapamil do not allow it to be recommended for widespread use for the preventive treatment of migraine during pregnancy [13].
Lisinopril exhibits a teratogenic effect when used in the 2nd and 3rd trimesters and should be discontinued. Candesartan, which has a mechanism of action similar to lisinopril, should also not be used to treat migraine in pregnant women [14].
Despite the high effectiveness of antiepileptic drugs in the treatment of migraines, their use during pregnancy is prohibited. Valproic acid preparations are absolutely contraindicated during conception and pregnancy due to their teratogenic effect (disrupting the development of the fetal neural tube) and blood clotting disorders in the mother and fetus. In addition, data have accumulated on the possible teratogenic effects (development of hypospadias, cleft lip and palate) of topiramate [14].
Gabapentin has low effectiveness in the preventive treatment of migraine; the safety of its use during pregnancy has been poorly studied. Its use should be stopped in the third trimester due to its possible effect on bone development [6].
Tricyclic antidepressants are highly effective in the preventive treatment of migraine. Amitriptyline is relatively safe during this period and is the second choice drug for the preventive treatment of migraine [6, 13, 15].
The use of the serotonin and norepinephrine reuptake inhibitor venlafaxine in the third trimester increases the risk of developing behavioral syndrome of newborns by 3 times. Symptoms are usually mild in severity.
The safety of botulinum toxin type A preparations for the treatment of migraine during pregnancy has not been studied. At the same time, data have accumulated on the absence of teratogenic and embryotoxic effects of botulinum toxin type A in pregnant women who reported using the drug for various indications [16]. At the same time, the use of botulinum toxin for the preventive treatment of migraine during pregnancy is not recommended.
New drugs for the preventive treatment of migraine - antibodies to calcitonin gene-related peptide - erenumab and fremanezumab have not been studied for use in pregnant women and are not recommended for the treatment of migraine.
In addition to the above medications allowed during pregnancy, various vitamins and minerals can be mentioned. In particular, there is evidence of the benefits of magnesium for the preventive treatment of migraine during pregnancy [13, 15]. Pyridoxine (vitamin B6) at a dose of 80 mg/day alone or in combination with other drugs at a dose of 25 mg/day, for example with folic acid, can have a mild preventive effect against migraine.
Table 1 summarizes the safety data of the main groups of drugs used for the preventive treatment of migraine during pregnancy.
Causes of labor pain
According to many years of observations by doctors and data from physiologists, many women experience almost no pain during contractions and pushing, behave quite actively or can even sleep. This cannot be called a phenomenon, since the source of labor pain is based in the cerebral cortex and is often activated by fear or confidence that pain is about to come.
In fact, when psychological factors are eliminated, expectant mothers experience only a pulling sensation in the lumbar region, where the nerve node is located. It innervates all the endings responsible for the female internal organs. Also, unpleasant mild pain appears in the lower abdomen at the moments when contractions occur. The reasons that more than seventy percent of women experience severe pain during labor lie in the structure of the female body, a sedentary lifestyle and prejudice.
Scientists who studied the life of small peoples of the Amazon and the Far North, where signs of civilization are practically invisible, were amazed at the ease with which native women give birth to children. They work physically, quite hard, until the onset of contractions, then retire for a while and return with the child in their arms. There are no signs of suffering on their faces. This happens, according to researchers, due to physical activity and the lack of psychological impact on girls.
In the cultures of such peoples, the process of pregnancy and childbirth is perceived as a taken-for-granted act, to which no special significance is attached. And every girl knows from childhood that, just like her mother, aunts and sisters around her, she will become pregnant and give birth to a baby. Of course, if complications arise, the woman most often dies, but in those cultures death is an absolutely natural phenomenon that is not given much importance.
In civilized countries, girls are taught from childhood, on a subconscious level, from the TV screen and from the pages of books, that pregnancy and childbirth are fraught with many dangers and the process of giving birth to a child is accompanied by enormous pain. Added to this is the sedentary lifestyle of most women, overeating and chronic diseases. All these factors together create the preconditions for a painful birth.
Take the first step
make an appointment with a doctor!