Composition and properties of PCC
The product consists of two components: powder and liquid.
The powder is converted zinc oxide with the addition of magnesium oxide. The liquid consists of a 37% water-based solution of polyacrylic acid.
Properties:
- ensuring a chemical relationship with tooth tissue;
- the formation of a strong bond with the metal, especially if it has been sandblasted;
- carboxylate has low toxicity to the pulp.
The finished working solution has the appearance of a paste-like consistency, with a smooth and shiny surface.
Carboxylate cements have their advantages and disadvantages:
| Advantages | Flaws |
| According to biological characteristics, they are highly compatible with dental tissues | Has the property of dissolving in the mouth over time |
| They do not allow acids to pass through, which are formed during the hardening of the filling. | |
| Are not an irritant to the pulp | Insufficient strength |
| Good adhesion to hard tooth surfaces |
Zinc polycarboxylate cements
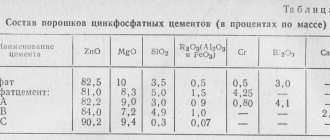
Curing reaction Zinc-polycarboxylate cements were introduced into dental practice in the late 60s, after a Manchester dentist had the bright idea of replacing phosphoric acid with one of the new polymeric acids, namely polyacrylic acid. These materials quickly gained popularity in dentistry as they were the first cements to adhere to enamel and dentin. The mechanism of adhesive interaction of these cements is the same as that of glass ionomer cements. Release form These cements are available in the form of a white powder and a clear viscous liquid. The components of the powder are zinc and magnesium oxides, and the liquid is a 30-40% aqueous solution of polyacrylic acid. Powder The composition of the powder is the same as that of zinc phosphate cements, containing zinc oxide and approximately 10% magnesium oxide or sometimes tin oxide. In addition, the powder may contain other additives such as silicon, aluminum or bismuth salts. The powder is fired at high temperatures to control the rate of the hardening reaction, and then ground to the desired particle size. Some brands also contain stannous fluoride to give the cement its positive fluoride-releasing property. The powder may contain pigments to provide different color shades. Liquid The liquid is usually a copolymer of polyacrylic acid with other unsaturated carboxylic acids such as itaconic and maleic. The molecular weight of the copolymer is in the range of 30,000 - 50,000. In modern compositions, the acid is dried at temperatures below zero degrees, then added to the powder; the liquid component of the cement in this case is distilled water. This method was developed to make it easier to achieve the exact ratio between the components, which was previously difficult to do due to the high viscosity of the liquid. The pH level was adjusted by adding sodium hydroxide, and tartaric acid was added to the material composition to control the hardening or curing reaction. The primary curing reaction of these cements is the reaction between zinc oxide and an ionized copolymer of acrylic and itaconic acid. After mixing the powder and liquid, the acid attacks the powder and causes it to release zinc ions. This is followed by cross-linking (in the form of bridging links in the polysalt matrix), just as occurs with glass ionomer cements, except that in this case, zinc provides more cross-linking than calcium and aluminum, as shown in Fig. . 3.6.1. The result of the reaction is a strengthened structure in which unreacted powder particles are held together by a zinc polyacrylate matrix.
Rice.
3.6.1. Formation of cross-links by zinc ions between the carboxyl groups of the polymer chains of polyacrylic acid Properties Working time and hardening time Compared to zinc phosphate cements, the hardening reaction proceeds quickly: mixing must be carried out within 30-40 seconds to allow sufficient working time. The viscosity of these cements does not increase as quickly as that of zinc phosphate cements. After a couple of minutes of mixing the components, the viscosity of zinc-polycarboxylate cement is less than the viscosity of zinc-phosphate cement after the same time, although at the initial moment the viscosity of polycarboxylate cement is higher. In addition, fresh mixed zinc-polycarboxylate cement has the property of pseudo-plasticity, which is expressed in the liquefaction of the mixture under the influence of shear forces during additional mixing. This means that although the material seems too thick, when placed in the mouth and applied pressure, its fluidity is quite adequate. This property of cement is not always taken into account by dentists, who, as a rule, tend to prepare a more liquid mixture by reducing the powder-liquid ratio, mistakenly assuming that this will give the cement increased fluidity; however, by doing this, the doctor significantly worsens the properties of the hardened cement. In general, the higher the powder-liquid ratio or the higher the molecular weight of the copolymer, the shorter the working time will be. For the use of cement as a fixing material, a powder-liquid ratio of 1.5:1 by weight is recommended, which provides a working time at room temperature within 2.5-3.5 minutes, and a hardening time at 37°C within 6- 9 minutes. As with zinc phosphate cements, the working time of polycarboxylate materials can be increased by using a chilled glass plate or powder stored in a refrigerator. Storing liquids in the refrigerator is not recommended, since they contain polyacrylic acid, which, when cooled, turns into a gel-like state due to the formation of hydrogen bonds. Increased working time is especially useful when using zinc-polycarboxylate cements as a base or lining for fillings, when the powder-liquid ratio of the cement mixture is higher. However, the too short working time of zinc polycarboxylate cements is a problem with these materials. In recent developments, this drawback has been eliminated by introducing an optimal amount of tartaric acid into the cement composition. Tartaric acid improves the quality of cement, lengthening its working time, while the hardening time remains almost unchanged. Biocompatibility Clinical observations have shown that upon contact with hard dental tissues or soft tissues of the oral cavity, zinc-polycarboxylate cements, despite the low pH level (in the range of 3-4), do not cause such a pronounced reaction as is observed with zinc-phosphate cements. This may be due to the rapid rise in pH to a neutral level during cement hardening and the limited ability of the polyacid to penetrate dentin. Research has shown that zinc polycarboxylate cements have some antibacterial properties, suggesting that this cement will provide a more reliable barrier to bacterial penetration than zinc phosphate cements. In addition, this higher protective ability of zinc polycarboxylate cements against bacteria is enhanced by their adhesive properties. It is likely that these factors are more likely to be the reason for the lack of reaction of the pulp to polycarboxylate cement than the more neutral pH level and increased molecular weight of the acid compared to zinc phosphate cements, at the same time, these same factors can lead to a decrease in the strength of the cement. Often, tin fluoride is added to cements, which releases fluoride and gives the material anti-carious properties against adjacent areas of enamel and dentin. Mechanical properties The compressive strength of fully hardened cement, prepared in a fixing consistency, is in the range of 55-85 MPa. It depends on the powder-liquid ratio and is slightly lower than that of zinc phosphate cements. The tensile strength is slightly higher, about 8-12 MPa. The elastic modulus is about 4-6 GPa, which is almost half the elastic modulus of zinc phosphate cement. As mentioned earlier, zinc polycarboxylate cements harden quite quickly, and this is reflected in the total time during which they reach their maximum strength; in 1 hour the strength of the cement reaches 80% of its final strength. Laboratory tests show that long-term storage of cement in water does not adversely affect its mechanical properties. Solubility As measurements have shown, the solubility of zinc-polycarboxylate cements in water is 0.1-0.6% by weight; the presence of tin fluoride in the cement slightly increases this figure. Like zinc phosphate cements, these cements are susceptible to acid attack, although clinical observations indicate that this property is not affected to a very serious extent, and cements of this type give good results in the clinic. Various types of failures in clinical practice are usually associated with errors in the preparation of the material, and most often due to a low powder-liquid ratio, when the doctor thus seeks to increase the working time of the cement. Adhesion Zinc-polycarboxylate cements differ from zinc-phosphate and zinc-oxide-eugenol cements in their ability to chemically adhere to enamel and dentin. The mechanism of this adhesive bond is the same as that of glass ionomer cements. The quality of the connection is such that it is maintained under in vivo conditions and exceeds the cohesive strength of cement, but is limited by the insufficient tensile strength of cement, which does not exceed 7-8 MPa. It is quite possible to obtain a bond of zinc polycarboxylate cement to metal surfaces, especially when dealing with cast metal prostheses. In this connection, there is again an adhesion mechanism of chemical ionic interaction with the metal surface. The adhesion of cement to gold alloys is very low and the bond usually fails at the interface due to the highly inert nature of the surface of gold alloys. Typically, improvement in bonding, although slight, can be achieved by pre-sandblasting or other abrasive treatment of the alloy surface to create a bond through mechanical adhesion. When combined with non-precious alloys, cement gives the best joint strength (when testing adhesive strength in these joints, an increase in the amount of cohesive destruction was noted), and this is probably due to the presence of an oxide layer on the surface of the alloys, which supplies the necessary metal ions. The strength of the joints is not particularly high due to the low cohesive strength of the zinc-polycarboxylate cements themselves. Application Zinc-polycarboxylate cements can be used for fixing metal-ceramic or all-ceramic prostheses on a reinforced frame, as well as for fixing orthodontic appliances.
Cements have the following advantages: • Bonds to both enamel and dentin and some cast metal restorations.
• Possess a mild irritant effect. The strength, solubility and film thickness for fixation are comparable to zinc phosphate cement.
• Have an antibacterial effect.
At the same time, cements also have disadvantages, including the following:
• The properties of cement greatly depend on the method of working with it. Short working time and long curing time.
• It is necessary to follow a procedure for working with the material to ensure an adhesive bond.
• Limited time to remove excess cement and difficulty in removing it
If removal of excess material is started too early and the material is still in an uncured elastic state, the marginal seal may be compromised, while if this procedure is delayed for a long time, it will be very difficult to remove excess cement due to its strong bond. with tooth enamel.
In general, despite the ability of this group of cements to release fluoride, most dentists prefer to use zinc phosphate or glass ionomer cements.
They believe that there is no big difference between these materials, which is confirmed by laboratory studies, and if there is, it is generally accepted that working with zinc phosphate and glass ionomer cements is much easier than with zinc polycarboxylate. Clinical significance Zinc-polycarboxylate cements have adhesion to enamel and dentin, and this is their advantage compared to zinc-phosphate cements. However, these cements are not as widely used as other water-based cements. Traditional glass ionomer and polymer-modified glass ionomer luting cements Although many of the properties of glass ionomer luting cements, and in particular the fluoride release and adhesion to enamel and dentin, are the same as those of a restorative material, some of the requirements for them are different. For example, since the gap between the restoration and the tooth tissue ranges from 20-50 microns, it is very important that the luting cement has the properties of forming a thin film. To achieve this, the glass powder particles must be smaller in size than in fillers for filling materials. Since changing the particle size of glass powder affects the performance and curing time of cement. The powder and liquid compositions of luting cements must be different from the corresponding compositions of filling cements in order to obtain optimal properties of the luting material. This also means that it is unacceptable to use glass ionomer filling cement for fixation, changing its rheological properties by reducing the powder-liquid ratio. Extended working time provides greater fluidity of the material and improves the quality of fixation of the crown or other prosthesis. However, as soon as the material begins to harden, its viscosity increases and accordingly it stops flowing. Thus, it is extremely important that the mixing of cement and cementation of the crown is completed within 2 to 2.5 minutes, since after this time the material becomes rigid and the film thickness increases. The choice of a material with short or long working time depends on the preference of the clinician and his experience with glass ionomer cements. Some newly developed modifications of glass ionomer cements are believed to not require a protective surface coating due to their faster curing rates. The solubility of cement, measured after 7 minutes by the amount of components transferred into the aqueous solution, decreased from approximately 2% for conventional glass ionomer cements to 1% for water-mixed cements. This figure could reach even lower values for cements based on maleic acid. Although it is still advisable to use cement protection in the initial period, because the problem of acid erosion for these materials remains relevant. In any case, these materials require some time to fully cure completely. It is best to use cements specifically designed for fixation, because... Changing the powder-liquid ratio of glass ionomer filling material to change working time, curing time and film thickness can only degrade its properties. With various modifications of cements for fixation, not only their performance characteristics change, but also their physical and mechanical properties. Table 3.6.2 shows the properties of two grades of luting cements. As can be seen from the mechanical properties, Aqua-Cem (Dentsply Ltd) has lower stiffness (which probably explains the higher diametric and flexural strengths for this cement), but it also has lower compressive strength and creep increases. Ketac-Cem (ESPE 3M) is more fragile than Aqua-Cem. In both cases, the materials have little crack resistance, and they need reliable support on the surrounding tissue. Clinically, Ketac-Cem has been observed to be easier to remove from soft tissue than Aqua-Cem. Possibly, since the first cement becomes brittle immediately after it is applied. Relatively recently, fixation materials based on polymer-modified glass ionomer cements have appeared. They have the full range of advantages already discussed in relation to filling and lining cements of this class. Low solubility and high adhesion to enamel and dentin of these materials provide high-quality and long-lasting tightness when fixing fixed dentures. The main difference between these cements and cements intended for fillings and linings is that they have an additional chemical curing mechanism (in the absence of light irradiation, in the dark), because It is not always possible to cure the fixing material with light. The following are examples of commercially available materials: Product Manufacturer PROTECHCEM IvoclarHVivadent, Schaan, Liechtenstein RelyXHLUTING CEMENT ZM Dental, St. Paul, USA FUJI PLUS GC International Corp, Tokyo, Japan These cements are recommended for use with cast metal crowns, bridges and inlays, metal-ceramic and all-ceramic crowns with a reinforced frame. Early in the use of glass ionomer cements for luting, there were several reports of increased tooth sensitivity after denture placement. However, there is now evidence that the number of such cases does not exceed the number of patients whose prostheses were fixed with zinc phosphate cement. Otherwise, there was no significant difference in the fixation of crowns and bridges with these cements. There are few publications in the literature on the results of the clinical use of polymer-modified glass ionomer cements for luting. There have been reports of hygroscopic expansion of these materials, which on the one hand can help reduce the gap around fillings of class V cavities, and on the other hand can lead to the destruction of all-ceramic crowns. The problem becomes even more serious when these materials are used to restore a badly damaged tooth crown, i.e. creating a stump for an artificial crown. Metal posts with poor mechanical retention can be permanently reinforced with polymer-modified glass ionomer cements. However, clinicians should be aware that if this pin later needs to be removed, it will be very difficult to do so. Clinical significance Glass ionomer luting cements have proven to be a reliable alternative to zinc phosphate cement, especially for all-ceramic prostheses. There is an opinion that the use of polymer-modified glass ionomer cements for fixation of all-ceramic restorations has some contraindications, at least until the time when more positive results of clinical observations of fixation of fixed prostheses with these materials appear. Fundamentals of Dental Materials Science Richard van Noort
Published by Konstantin Mokanov
Method of application
The material is used for fixing different types of inlays and crowns, small-sized prostheses - bridges, and orthodontic devices. Used for filling children's teeth, as well as for temporary fillings.
To mix polycarboxylate cement mortar, use a clean piece of glass and a spatula.
Just before mixing, drop the required amount of liquid base from a bottle with a dropper onto the glass. To prevent the liquid from evaporating, the bottle must be closed immediately. Then add the powder and quickly mix for about 30 seconds.
The powder must be added in portions, first dividing into two equal parts. First, one share is combined and mixed with the liquid for 15 seconds. Then add the second one and continue mixing until smooth (in the same time as the first).
The best ratio of powder to liquid is considered to be 0.4:0.2, respectively.
If the temperature in the room exceeds 22°C, then the dose of powder should be reduced or a little more liquid component should be added.
From the start of mixing, the prepared composition must be used within 1-2 minutes. An indicator can be the glossy and shiny surface of the prepared pasta.
The cement hardening time is 5-10 minutes. With more liquid, curing takes longer.
The rate of hardening depends on:
- correctly selected proportion of powder to liquid;
- reaction susceptibility of zinc oxide;
- particle size and the presence of additional impurities;
- polyacrylic acid content.
After 10-12 hours, the material completely hardens. Food can be taken no earlier than 4 hours after mouth treatment.
Filling tooth canals on video:
Materials for filling and restoring teeth
Types of composites
Classified:
- according to the characteristics of hardening (chemical, light, double);
- physical condition (diluted powder, paste, liquid);
- concentration and size of particles filling the composition;
- degree of transparency;
- purpose of use (universal, for lateral (chewing), anterior (frontal) teeth).
Macrofilled, microfilled, mixed (hybrid), and nanocomposites are known.
Particles of macrofilled composites have a size of 1-100 microns, the filler occupies up to 87% of the weight of the material. The advantages are high strength, but they are characterized by roughness, low level of aesthetics, changeable color, and the possibility of secondary caries formation. They are used in adding tooth stumps for crowns and working with loaded cavities of classes I and II.
The size of the elements of microfilled composites is 0.007 - 0.4 microns. The weight of the filler is up to 79% of the total mass of the material with high aesthetics. Main disadvantages: fragility. It is used for the reconstruction of anterior teeth that do not experience significant load, and cosmetic operations for contouring the treated teeth.
The particles of hybrid type composites have a size of 0.04 - 4 microns, the filler occupies up to 87% of the weight of the material. Macrohybrids consist of elements measuring 0.04 - 3 microns. Solutions of this group are characterized by stable color, high strength, easy polishability, and aesthetic qualities. Designed for working with front teeth (group A), filling lateral teeth (group B). Microhybrids are suitable for creating fillings on all types of teeth and working with any cavities, that is, they are completely universal.
Nanocomposites differ in particle size from 20 to 75 nm. The weight of the filler is 78.5% of the total mass. The particles are produced through industrial synthesis rather than grinding. The advantages are durability, color stability, and external beauty. Used to make fillings on all teeth and in any cavities.
A material that combines the technology of producing glass ionomers and composites is a compomer. Consists of acrylic resin, strontium fluoride, strontium-fluorine-silicon glass, polyacrylic acid, stabilizers and polymerization initiators. It is characterized by excellent biocompatibility, good adhesion, but low strength and poor aesthetics. Due to their physical properties, they are mainly used when working with milk and non-stressed teeth, as well as as insulating spacers.
Popular brands and manufacturers
The brands and manufacturers presented in the table have proven themselves well:
| Name | Manufacturer |
| "Belokor" | VladMiVa |
| "Belokor" | Rainbow-R |
| "Carbofaine" | Spofa Dental |
| Polycarboxylate cement | Stoma |
| Polycarboxylate cement | Medpolymer |
| Polycarboxylate cement with potassium nitrate | Medpolymer |
| Adhesor Carbofine | Spofa Dental |
| Aqualox | Voko |
| Carboxylatzement Bayer | Bayer |
| Cimex | DentAmerica |
| Durelon Powder | ESPE |
| PolyCarb | PSP Dental |
| PR Scell Polycarboxylate | Pierre Holland |
| Selfast | Septodont |
| Carboxylatzement Bayer | Bayer |