Corrective osteotomies of the knee joint are used
- as an independent method of treating degenerative-dystrophic pathologies of large joints, for some infectious diseases of bones and congenital pathologies;
- as part of one of the stages of complex treatment of arthrosis of various etiologies, at the final stage of which the joint is replaced with an endoprosthesis.
What is corrective osteotomy of the knee joint?
This is a surgical intervention in which, through surgical manipulation of the tibia or femur, the effect of shifting the circular axis of load distribution on the lower limb and giving it a more physiological position is achieved.
The operation corrective osteotomy found its rebirth in the early 2000s; until that time, knee arthroplasty . Recently, the point of view has triumphed that while the patient is relatively young (up to 60 years), the regenerative features of his body are relatively great, and irreversible changes have not yet occurred in the knee itself, leading to its almost complete immobility and wear of the working surfaces over a large area, corrective osteotomy will allow a person to preserve his own joint with a minimal amount of surgical access. At the same time, in the postoperative period, complete restoration of knee function is possible while maintaining all types of physical activity and without reducing ability to work.
Contraindications to high valgus osteotomy of the tibia:
- body mass index over 35
- knee instability
- extension contracture more than 15 degrees
- flexion contracture (more than 60 degrees)
- severe arthrosis of the patellofemoral joint
With proper patient selection, the effectiveness of high valgus osteotomy of the tibia is extremely high. The 10 year survival rate is 92%. Corrective osteotomy may be complemented by procedures aimed at restoring articular cartilage in the medial compartment of the knee joint.
According to a study by Schallberger in 2010, which retrospectively analyzed the long-term results of treatment of medial knee arthrosis using high valgus osteotomy, the 5-year survival rate was 98%, 10-year 92%, 15-year 71%. In total, total arthroplasty was required in the long term in 24% of cases. Patient satisfaction was 80%, the average VAS score was 0, and radiologically there was an almost complete absence of arthrosis progression.
Knee Surg Sports Traumatol Arthrosc. 2011 Jan;19(1):122-7. doi:10.1007/s00167-010-1256-4. Epub 2010 Sep 7.
High tibial valgus osteotomy in unicompartmental medial osteoarthritis of the knee: a retrospective follow-up study over 13-21 years.
Schallberger A1, Jacobi M, Wahl P, Maestretti G, Jakob RP.
So, if your knees are not aligned and your legs are shaped like a wheel, you are physically active, and your knee pain is associated with primary medial arthrosis, a high valgus tibial osteotomy is your choice.
What types of damage are treated?
With gonarthrosis, there is an uneven distribution of load on the articular surfaces. Most often there are two types of such distribution:
- varus deformity of the limbs (legs - “wheel”) is the most common type of pathology in which the internal surfaces of the joint are affected;
- valgus knees (X-shaped) - when the outer surfaces of the joints are worn out.
The operation is performed only if the articular surfaces are damaged unevenly, on only one side of the knee. In the case of total damage (as in rheumatoid arthritis), the intervention in question is completely useless and absolutely contraindicated.
The essence of the operation and the result
The main goal of the intervention is to distribute pressure and friction evenly across the knee joint, reducing this impact on the most affected areas by loading those that are more preserved and functional.
As a result, the axis of the load on the limb is shifted, giving it a more physiological position, and, as a result, a more balanced distribution of the load (and let us remember, when walking it is about four body weights on one knee, when running - about eight), and reducing pressure on the “sick” area of the joint surface.
Advantages of the method
- Relatively low invasiveness of the intervention. Surgical access is achieved by making an incision of only about one centimeter;
- follows from the previous one. This manipulation does not always require anesthesia, and in the vast majority of cases it is performed using regional, spinal or epidural (less often) anesthesia;
- as a result of the manipulation, the patient is discharged from the clinic with his knee completely preserved, and, subject to a number of conditions, a complete restoration of its functions is possible;
- the duration of the operation is about one and a half hours, it is well studied, with many years of experience;
- length of hospital stay is about three days;
- the time to return to the full range of activity of the limb is about two months.
Orthognathic surgery. Osteotomy of the upper and lower jaw. Genioplasty.
In the 21st century, modern orthodontics has enormous potential for solving the problems of malocclusion, which are associated with the incorrect location of the skeletal structure of the upper and lower jaws. Malocclusion can be either congenital or acquired as a result of injuries.
By the age of 16-20, such a jaw anomaly becomes more pronounced, which creates a certain discomfort, both psychological and aesthetic. People become unsure of themselves, and their self-esteem begins to decline. But this is not only a matter of aesthetics; such a pathology contributes to the development of a number of joint diseases, tooth loss, respiratory dysfunction, etc. All problems associated with eliminating such facial disharmony, returning normal occlusion (bite) and facial aesthetics can be solved by orthognathic surgery .
At the Federal State Budgetary Institution Scientific and Clinical Center of Otorhinolaryngology, Federal Medical and Biological Agency of Russia, orthognathic operations are performed by employees of the scientific and clinical department of maxillofacial surgery. Our Center employs some of the best specialists in Russia in the field of orthognathic surgery - Ph.D. Senyuk A.N., Lyashev I.N., Mokhirev M.A. Nazaryan D.N. , who apply not only the most modern world techniques, but also use their own developments.
“We often have to correct the mistakes of doctors who, with insufficient experience working with such patients, or in the pursuit of profit, corrected malocclusion, which ultimately led to severe complications and patient dissatisfaction with the final result of treatment,” says the head of the department of maxillofacial medicine. Facial and Reconstructive Surgery, Ph.D. Nazaryan D.N.
In their practice, our specialists carry out complex treatment, which includes orthopedic and orthodontic interventions, to achieve functional and aesthetic goals. Only an experienced specialist can determine that braces and orthodontic wires will not be able to relieve a patient with a skeletal jaw deformity from a protruding chin or a “ gummy smile ”, but on the contrary, they can lead to tooth dislocation and the development of the temporomandibular joint. We take a comprehensive approach to solving such problems, the essence of which lies in preliminary stage-by-stage preparation and preliminary 3D planning. Computed tomography, photography, plaster and STL models allow us to perform a complete preoperative analysis and simulated surgery. Orthognathic surgery allows you to move one or both of the patient's jaws back and forth, up and down. The treatment procedure takes place according to a pre-planned scheme, which involves moving the jaws, chin, soft tissues, eliminating dentoalveolar compensation, and aligning the dentition in relation to the main bone.
Orthognathic surgery is performed with maxillary osteotomy , where intraoral bone incisions are made above the teeth and below both eye sockets, allowing the upper jaw, including the palate and upper row of teeth, to be repositioned. This movement is positioned using a pre-made special splint, which will reliably guarantee its correct position of the lower jaw in relation to the soft tissues.
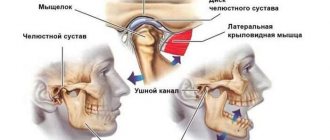
A mandibular osteotomy involves making bone cuts behind the molars, along the jaw, and downward so that the mandible can move as a single unit. As a result of this manipulation, the lower jaw, with the help of a titanium plate, smoothly moves to a new location.
The genioplasty operation is aimed at leveling the midline of the patient’s face, during which the chin part of the lower jaw is cut off and moved in the correct, harmonious direction.
All orthognathic operations are performed using intraoral access and do not have external incisions or scars. Such operations, in order to avoid relapses associated with continued jaw growth, can be performed on patients over 18 years of age, since it is believed that by this age the growth of a person’s jaws is completed. Orthognathic operations are performed under general anesthesia and, depending on the planning of the treatment requiring correction, can last from one to six hours.
In our Center, using specially made titanium plates, specialists fix all detachable parts of the jaw. After surgery, the following temporary symptoms are possible: postoperative swelling, bruising in the lips and cheeks, difficulty communicating in the first week after surgery, limited oral hygiene, numbness in the operated area, and a feeling of nasal congestion. In order to minimize risks and complications after surgery, the patient should follow the doctor's recommendations during the recovery period. After surgery, patients are recommended to eat semi-liquid food; there are no special dietary restrictions.
Thanks to Andrey Nikolaevich Senyuk in Russia, orthognathic surgery began to be carried out entirely using intraoral approaches, using preliminary preoperative planning in such a way that a precisely planned result in advance is achieved, coinciding with the final one both in terms of aesthetics and occlusion. It was he who organized the first international conference of orthofacial surgery in Russia.
Many years of experience in orthognathic surgery and deep knowledge of the problem will allow our highly qualified specialists to work wonders, as noted by the patients themselves), restoring self-confidence to patients and leading a fulfilling lifestyle. The surgical team of the department, headed by Doctor of Medical Sciences, Professor Karayan A.S., develops an individual treatment program for each patient, and attention and warmth from the treating staff are guaranteed to everyone!
Clinical cases
Example 1
| Diagnosis: combined deformation of the jaws, asymmetrical deformation horizontally. Planned: osteotomy of the jaws according to Le_Fort 1 and sagittal of the lower jaw. |
| On the 7th day: |
Other examples:
| BEFORE | AFTER |
Which is preferable: knee replacement or corrective osteotomy?
This question can be encountered in discussions both among patients and in the professional community. Although, objectively, the question of choosing between these manipulations can only be decided if there are contraindications to surgery using the corrective osteotomy method .
In all other circumstances, there are usually two options:
- corrective osteotomy of bones cannot have an alternative in the form of endoprosthetics, since it is aimed at solving completely different problems and is prescribed for other indications;
corrective osteotomy cannot be replaced with prosthetics, since it is only a stage in the strategy of therapeutic measures, the final of which will be knee replacement.
Indications for surgery
- age – up to 60 years. At a young age, tissue regeneration, and therefore rehabilitation, occurs faster and more reliably. In old age, the operation of choice is complete joint replacement with an endoprosthesis;
- no signs of obesity. Excess weight will negate all the positive effects of the operation very quickly, and the relief will be short-lived. A vicious circle is started: excess body weight, as a result, increased load on the knee, resulting in a recurrent course of arthrosis;
- rachitic changes in bone tissue. Provides both a reduction in wear on the surfaces of the knee joints and the correction of cosmetic defects;
- deforming arthrosis, gonarthrosis. Together with other recommendations, this is the main and main indication;
- improperly consolidated fractures of the lower extremities and shortening of one of the lower extremities - the principle is the same. Redistribution of the load followed by automatic alignment of the limbs;
- osteomyelitis. When treating this pathology, the infected area of the bone is excised and replaced with an autoimplant. Thus, the focus of the purulent process is removed, and due to autoimplantation of bone tissue, regeneration processes are accelerated.
In what cases will osteotomy not help?
The effectiveness of treatment depends on the age, gender and body weight of the patient. Unsatisfactory results of the operation may be due to the patient's advanced age, significant bone damage and destruction of hyaline cartilage.
Conditions in which intervention is inappropriate:
- rheumatoid arthritis;
- osteoporosis;
- extra-articular pathologies;
- lack of blood supply to the lower limb;
- impaired bone growth;
- absence of meniscus;
- severe obesity (BMI: 40 and above).
If the indications are not properly assessed, osteotomy can accelerate degeneration of the knee joint. Before treatment, doctors conduct laboratory tests, take photographs of the lower limb along its length and prescribe additional diagnostic procedures.
The purpose of corrective osteotomy of the knee joint
There may be several ultimate goals set by an orthopedist when prescribing surgical treatment, and they depend on the strategic objective:
- can be used as a long-term complex therapy for arthrosis - as an intermediate link in a chain of sequential changes in treatment tactics, from conservative and physical treatment to radical joint replacement;
- used as an independent and main method of treatment for incorrectly consolidated fractures, to eliminate congenital and acquired cosmetic defects of the lower extremities, in the presence of ankylosis and false joints.
Life after treatment
The prognosis is determined by the initial diagnosis, the chosen surgical treatment technique, the surgeon’s qualifications, the patient’s age and other criteria. According to the G. A. Ilizarov Medical Center, positive results were noted in 95% of patients after the intervention. For 10 years after bone grafting, there is no pain or other symptoms of gonarthrosis. Young people who have undergone osteotomy return to a full life after rehabilitation. Subsequent replacement arthroplasty is facilitated.
The long-term results of the correction are difficult to predict. Patients are advised to regularly visit an orthopedist and undergo examinations to monitor the condition of the joint. Osteotomy as an independent treatment method does not completely eliminate arthrosis, but only slows down the development of degenerative processes. In some patients, relapse occurs as early as 4 years after the intervention.
How is the operation performed?
The meaning of the surgical intervention is that an incision is made on the bone on the side of the greatest damage to the joint, a hole of the required shape. After this, the required amount of one’s own bone or cartilaginous substance is placed into this hole, due to which the limb is, as it were, retracted to the side, deviated along the axis of the body in the direction opposite to the pathological process.
Osteotomy with metal structure
Next, the area of the bone where the incision was made with the bone autoimplant placed there is fixed with a titanium plate using screws . Then the access is sutured, and the limb is immobilized using a splint or splint. There is no need to apply plaster.
Types of surgical techniques
- by type of access - open and closed. There are situations when open access, despite being more invasive (when the bone surface is exposed and the incision width is 10–12 centimeters), is preferable. The need for this type of intervention is due to the increased risk of damage to nerves and blood vessels during surgery;
- by level of implementation of interventions. Depending on the location of the pathological process and the goal, excision is performed on the femur or tibia. On the latter, in turn, high and low tibial osteotomies are performed;
- according to the method of excision of bone tissue - wedge-shaped, transverse, straight, oblique, spherical;
- by the nature of the correction - opening, closing.
Knee osteotomy: visual representation of the procedure.
Lengthening osteotomy
The intervention is performed to equalize the lengths of the lower limbs in order to return the person to normal mobility, without signs of lameness. The simplest way to lengthen one of the legs is an osteotomy based on the principle of oblique cutting of the bone. To compensate for the existing shortening, a procedure involving stepwise cutting of the femoral diaphysis is sometimes recommended, but it is technically much more complicated. Lengthening surgery is always combined with compression-distraction osteosynthesis (installation of transosseous traction devices on the limb).
Rehabilitation
Rehabilitation measures after corrective osteotomy of the knee joint using plates with angular stability usually last no more than four weeks. There are often cases when the period of rehabilitation measures can increase significantly. This is due to the individual characteristics of the patient, but the largest share in such cases is due to ignoring the recommendations of the attending physician and non-compliance with the conditions and timing of the postoperative period. If you strictly follow the rehabilitation plan, the chance of developing complications or delaying the healing process is minimal.
The patient begins to perform the first sets of physical therapy exercises while still in the hospital (the inpatient treatment phase takes from three days to a week). In the postoperative period after corrective osteotomy of the knee joint, rehabilitation measures are aimed primarily at restoring blood circulation and maintaining full trophism of the limb. At this time, exercises for bending and extending the leg at the knee, massages of the feet and hips, symptomatic, restorative, antibacterial therapy and anticoagulants, cold on the leg are indicated. The patient walks on crutches (about three months); putting weight on the operated limb is absolutely contraindicated.
The main role in rehabilitation belongs to physical therapy. The load on the joint should be gradually increased. The number of exercise therapy exercises and their duration increase; at later stages, exercise classes on an exercise bike and swimming are prescribed. During the recovery period, physiotherapeutic procedures are required.
The entire period of rehabilitation and full restoration of performance takes from six months to a year.
Recovery period
Consolidation of the osteotomized area occurs no earlier than after 4 months, so the rehabilitation regimen prescribed by the doctor must be carefully followed during this entire time. Complete healing of the fracture, since the physiology of each individual organism is unique, is observed in patients at different times. But on average, the bone heals within 4-6 months.
Throughout the entire postoperative period, you should strictly adhere to the orthopedic regimen: dosed bed rest, walking on crutches without relying on the problematic leg, a ban on certain types of movements and body positions, exercise therapy, etc. Let us emphasize that an integral measure for successful recovery is physiotherapy. Without it, it is impossible to fully restore the balance of the muscles responsible for the functioning of the musculoskeletal system. Physiotherapy and massage procedures are also prescribed for a speedy recovery.
To relieve postoperative pain and inflammation, the patient is prescribed medications from the NSAID series. A specially selected course of antibiotic treatment is required to prevent infection. Among the medications, calcium and vitamin D preparations, stimulants of repair processes, B vitamins, and antiplatelet agents are also recommended.
Only after complete consolidation has been confirmed by x-ray is it possible to walk, fully relying on the limb. Premature axial loading leads to complications, which are often eliminated solely by reoperation.