Difference between molars and premolars
The main difference between molar teeth and premolars is their location on the jaw.
Premolars are located closer to the front of the dentition, and molars are slightly moved inward. Their quantity also varies. There are always two premolars on each side of the upper and lower jaws. There can be either two or three molars. Still others are also called “wisdom teeth.” They grow later than others and often appear only at 20-25 years of age. This process is often accompanied by malaise and fever. However, not all people on earth have third ones. A certain genetic predisposition can cause the absence of wisdom teeth in the oral cavity.
Chewing surface of the tooth
The chewing surface of the tooth is the surface of the tooth facing the teeth of the opposite row (directed upward for the lower teeth, and downward for the lower teeth). The chewing surface is also called occlusal, or closure, since it is it that is involved in the formation of occlusion, or the closure of the upper and lower dentition. Its shape and compliance of the chewing surface of the teeth of the upper row with the chewing surface of the teeth of the lower row is important for complete chewing and grinding of food.
The chewing surface in the proper sense is present in large and small molars ( molars and premolars ), since they perform the main function of chewing and grinding food. In incisors and canines, the cutting edge is directed towards the teeth of the opposite row, which is usually quite narrow. The cutting edge is used to bite off food. In canines, this edge is usually narrowed and pointed to one degree or another, and is partially involved in tearing tough pieces of food (for example, meat fibers). In predators, fangs are the main teeth with which they bite off (tear off) pieces when eating prey. In humans, due to the fact that his ancestors were omnivores, that is, they could eat both animal and plant foods, as well as the transition to a diet consisting of food that was mainly heat-treated, the size of the fangs is smaller than that of predators, and their function is mainly to participate, along with the incisors, in biting off food.
In total, the crown of the tooth has several surfaces:
- Chewing surface
- The vestibular surface is the surface directed towards the vestibule of the mouth. In the front teeth it is also called the labial surface, since it is directed towards the lips, and in the rear teeth it is called the buccal surface, since it is directed towards the mucous membrane of the cheeks.
- The lingual surface is the surface opposite to the vestibular one, and facing the actual oral cavity and tongue. It is also called oral (from oris - Latin mouth).
- The contact surface, or approximal, is the surface directed towards adjacent teeth. The approximal surfaces facing towards the center of the dentition (forward) are called mesial surfaces of the teeth. In the case of the front teeth (incisors), these surfaces are called median. The approximal surfaces directed backwards towards the posterior teeth are called distal.
The shape of the chewing surface of teeth is individual and varies depending on the anatomy of a particular person. Typically, the chewing surface of premolars consists of 3-4 cusps, molars - of 4-5 cusps. In practice, in specific patients, there is often a deviation in the number of teeth in the direction of either increasing or decreasing their number. However, molars with a chewing surface consisting of 7 or more cusps are extremely rare.
Copying the chewing surface of teeth as accurately as possible is one of the most difficult tasks in dental prosthetics facing the dentist and dental technician. It is necessary to take into account all the nuances of the individual characteristics of the chewing surface so that the manufactured prosthesis or crown performs its function as fully as possible, and so that the achieved result meets all the requirements in terms of aesthetics. Even a small error in the restoration of the chewing surface of the lateral teeth can lead to the fact that chewing food will be incomplete or difficult, and the patient will experience unpleasant sensations of incomplete closure of the dental arches and discomfort. A precisely executed and reproduced chewing surface of the teeth makes artificial crowns as aesthetically pleasing and natural as possible, and the process of chewing food is carried out in the most complete and physiological manner.
come back
Features of the structure of molars
Molars have a characteristic structure. On the upper jaw they have three roots and four canals. The lower jaw has two roots and three canals. Moreover, the number of canals also differs depending on the location of the individual tooth. Thus, the first of them often have one more channel than the next two.
The main characteristic feature of this type of teeth is the area of their chewing surface. They bear the heaviest load when chewing food particles. The molars themselves also have differences among themselves, which are associated with the structure of the jaw.
Molar Differences
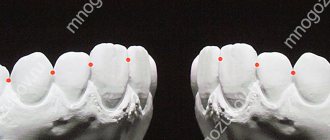
Often the surface of each molar tooth is shaped like a triangle. There is a certain number of tubercles on it, which take an active part in chewing food. The number of such tubercles may vary. Usually there are three, but sometimes there are more.
Such mounds are connected to each other by special ridges. On the upper and lower jaws the structure of these elements is different. In the upper dentition, the apex of the surface triangle is directed towards the tongue. This form is called a trigon. On the lower jaw, the apex of such a triangle is directed towards the cheek, which is called the trigonid. The size of the first and second types of teeth is practically the same.
Occlusal surface
The occlusal surface of natural teeth is the part of the tooth surface from the tops of the cusps to the deepest part of the central fissure. It is characterized by anatomical features that are genetically tailored for function. The occlusal surface has the following elements: the tops of the tubercles, their bases, slopes, ridges, triangular ridges of the slopes of the tubercles and the marginal fossae limiting the so-called occlusal table, central and additional fissures (Fig. 2.19). The internal slopes of the tubercles of the teeth face the central fissure.
The cusps of the teeth are the main element of the occlusal surface. Their location determines the shape of the tooth. Each tubercle has a base, apex and slopes. The top of the tubercle of each tooth is slightly shifted towards the middle of the chewing surface.
Rice. 2.19. Morphology of the occlusal surface of the upper premolar (a) and central incisor (b). a: 1 - apex of the palatine tubercle; 2 - triangular ridge of the internal slope of the tubercle; 3 - central fissure; 4 - marginal fossa; 5 - crest of the tubercle; 6 - apex of the buccal tubercle; 7 - marginal ridge along the periphery of the occlusal surface; 8 - external slope of the tubercle; 9 — base of the tubercle; b: 1 - cutting edge; 2 - dental tubercle; 3 - median roller; 4, 5 — mesial and distal marginal ridges; 6 - pits.
The apices of all tubercles are connected by a marginal ridge, which limits the occlusal surface along the periphery. The largest transverse diameter of the tooth is 2 times the diameter of the occlusal surface (Fig. 2.20). Triangular ridges run from the top of the tooth tubercle to the middle of its chewing surface. The opposing occlusal surfaces slide along these convex ridges—the ridges of the tubercle.
The slopes of the tubercles facing the central fissure are designated as internal, and those located orally and vestibularly as external. In the approximal areas, the tooth has mesial and distal marginal pits. The marginal pits of two adjacent teeth form a pit for the tubercle of the antagonist tooth.
The central fissure separates the buccal and lingual cusps of the teeth. The slopes and ridges of the main tubercles converge in the central and additional fissures.
The occlusal (palatal) surface of the upper incisors and canines on the mesial and distal sides has two marginal ridges, which are connected by a dental tubercle in the lower third of the tooth.
Rice. 2.20. Occlusal surfaces, cusp slopes, “occlusal table” of the upper right premolar. B - external, vestibular; D - distal; M - mesial; H - oral surface of the tooth; 2, 1 - mesial and distal slopes of the buccal tubercle; 4, 3 - mesial and distal slopes of the palatine tubercle; 5, 6, 7, 8 - internal slopes of the tubercles; 9, 10—marginal pits. Between the tops of the tubercles and the center of the tooth there are triangular ridges of the slopes of the tubercles. The internal slopes of tubercles 5, 6, 7, 8, limited by the marginal ridge, are the “occlusal table.”
Between the middle of the cutting edge and this tubercle there is a median palatal ridge, on both sides of which there are grooves. The dental cusp is the most convex part of the tooth and is the site of occlusal contacts.
The buccal tubercles of the lower and palatal upper chewing teeth are called abutment teeth, since they crush food, determine the nature of movements of the lower jaw within the occlusal field, and redistribute chewing forces so that the main chewing load is along the axis of the tooth.
The lingual cusps of the lower and buccal cusps of the upper chewing teeth are called non-supporting, “protective”. In central occlusion they have easy contact with antagonists or, according to some authors, do not have such contact. These tubercles carry out the function of separating food, create sliding surfaces on their slopes for antagonists, and when chewing, protect the tongue and cheeks from getting between the teeth.
Point (not planar) multiple, uniform contacts of antagonizing teeth are the most favorable form of occlusion for the chewing function, which should be created when modeling the occlusal surface (Fig. 2.21). In this case, it is possible to process food of any consistency, chewing pressure is distributed along the axis of the teeth, the load on the periodontium is minimal, small point contacts reduce abrasion of the chewing planes. The contact of the cusps and fissures according to the “pestle in mortar” principle creates stability of the lower jaw in the position of central occlusion and does not interfere with the movement of the lower jaw within the occlusal field.
Rice. 2.21. Point occlusal contacts of the cusps and fissures of the teeth of the upper and lower jaws. The circles are the supporting buccal cusps of the lower teeth and the corresponding contacts with the teeth of the upper jaw; black dots are the supporting palatal cusps of the upper teeth and corresponding contacts with the teeth of the lower jaw.
Rice. 2.22. Three options for the relationship between tubercles and fossae in the position of central occlusion. a - “free central occlusion”: the tops of the tubercles are in contact with the bottom of the pits, free spaces around the tubercles, axial loads on the periodontium are indicated by arrows; b - point contacts of the slopes of the tubercles: horizontal loads on the periodontium are possible, the tops of the tubercles are not subject to abrasion: 1, 2, 3 - classes of the occlusal surface; c - “lingualized occlusion” (used for prosthetics on implants). Rice. 2.23. Trajectories of the main movements of the lower jaw [according to R. Marxkors, 1993]. a - “occlusal compass” on the upper first molars; b - “occlusal compasses” on the teeth of the lower jaw - a mirror image of those on the teeth of the upper jaw. The black line is the path of forward movement; blue - the path of the labor movement; green - the path of balancing movement; red dots—central occlusion.
There are two ways to model occlusal contacts in the position of central occlusion (Fig. 2.22): three-point contacts of the slopes of the supporting tubercles and contact of the tops of the tubercles with fissures and marginal fossae. The second method is easier to implement; it eliminates the horizontal load that occurs between the internal slopes of the supporting tubercles, but its use increases the risk of excessive abrasion of the tops of the tubercles.
If we designate the path of movement of each supporting tubercle in the corresponding fossa or fissure of the opposing tooth from the central position to the anterior occlusion position, to the working and balancing sides, we will obtain the trajectory of the main movements of the lower jaw, the so-called occlusal compass (Fig. 2.23). On the teeth of the upper jaw, the path of anterior movement of the cusps of the lower teeth is directed forward, and on the teeth of the lower jaw - backward. The movement of the supporting tubercle to the working side is perpendicular to the path of the forward movement, and the movement of the supporting tubercle to the balancing side is directed at an angle of -45° to the path of the forward movement. Consequently, the cusps of each tooth should be so located that during lateral movements of the lower jaw they pass “in the span” between the cusps of opposing teeth and so that there are no occlusal obstacles on the working and balancing sides.
If the occlusal surface of the teeth is lost (absence of teeth), when restoring it, an occlusal plane is used, passing through 3 points: the contact of the lower central incisors (incisal point) and the tops of the distal buccal cusps of the second lower molars. This plane is parallel to the Camper horizontal and is used to install the model of the lower jaw into the articulator according to the average data (using, for example, a balancer) (Fig. 2.24).
Rice. 2.24. The occlusal plane between the incisal point and the distobuccal cusps of the second molars.
V.A.Khvatova Clinical gnathology
Source: https://medbe.ru
Possible damage to small molars
Carious lesions of primary and molar teeth in children are observed quite often. This is due to the bumpiness of their surface, which can trap food particles and bacteria. Since children at an early age do not always actively and correctly brush their teeth, these residues can lead to damage to the enamel and deeper spread of caries.
Depending on the degree of damage, caries can penetrate either exclusively into the enamel, or into dentin or even cement. In the latter case, we are talking about deep caries, which often requires serious treatment or even tooth extraction.
Another variant of damage is a change in tissue structure, which may be associated with metabolic disorders in the human body or other diseases. Such a disease can also be the result of poor nutrition or constant diets, in which the body does not receive enough nutrients.
At any age, a person can experience excessive tooth wear, which leads to the destruction of enamel and can cause other serious damage. Teeth can wear down in different situations, such as:
- if a person has bad habits of grinding his teeth, etc.;
- in case of improper or insufficient nutrition;
- in the presence of diseases of the endocrine system;
- due to a genetic predisposition to enamel depletion.
All of these lesions can be the result of both an incorrect lifestyle and various diseases or heredity. Regardless of the reasons, it is necessary to begin treatment of emerging injuries immediately so as not to aggravate the process.
The reason for the formation of a lump on the gum
There are two groups of reasons that lead to the appearance of a hard white lump on the gum. This formation itself is a tubercle, which may consist of inflamed tissue or be filled with pus. The tubercle may hurt constantly or when you press on it. Often it does not hurt at all and is not noticed immediately. Such a lump indicates one of many diagnoses. But let's return to the reasons.
The first group is infectious causes. Like most oral diseases, a hard lump on the gum is caused by poor hygiene. The problem is caused by irregular and poor-quality teeth cleaning, as well as tartar and gum inflammation left without treatment. Tooth decay can also cause a lump to appear. The spread of caries into the root canals will cause deep damage to the internal structures of the jaw.
The second group is injuries. For example, a complex tooth extraction may have been carried out inattentively. This often injures the gums. Also, pieces of tooth could remain in the jaw. Errors during implantation are another reason for the formation of a lump on the gum. Any incorrectly completed dental treatment is very dangerous, as consequences will certainly appear over time.
Even braces can cause a bump. It is also possible that the patient may have genetic disorders that could lead to the appearance of a lump on the gum on the inside or on the outside. Such a lump can also be a benign or malignant tumor. As you can see, there are many reasons - so it is necessary to undergo an inspection as soon as possible, because the consequences of all these violations will be quite serious.
Replacement of primary molars with permanent permanent molars
Molars are the first permanent teeth to appear in a child's mouth. This begins around the age of five. Growth begins with the first molar tooth, which appears in a free space in the depths of the jaw, closer to the milk one that has not yet fallen out.
The second molar usually grows in at the age of 12-13 years. It also takes up free space and does not replace a baby tooth. The latter, or “wisdom teeth,” may take up to 25 years to grow or may not appear at all.
As for dairy products, they begin to fall out from the age of 9. In their place, permanent teeth grow, which occurs at approximately 10-12 years of age. Usually these are the last molars, the growth of which must wait to fill the adult dentition (not counting “wisdom teeth”).
Is it possible to loosen baby molars?
The process of tooth loss always begins with softening of its root. This occurs as the jaw grows, freeing up more space for a permanent tooth. Thus, while the baby tooth is still in the hole, the molar is already beginning to take its correct place.
In this regard, dentists categorically do not recommend deliberately loosening baby molars. If they fall out prematurely, jaw growth may be stunted. As a result, there will not be enough space for permanent teeth, and they will begin to grow crookedly, getting out of the general dentition.
Signs of imminent appearance of molars
The first signs that molars are about to appear are noticeable even before the baby teeth fall out. These include the following:
- widening of the jaw, which can be seen when gaps appear between other baby teeth;
- the appearance of sufficient free space behind the outer lateral milk teeth;
- swelling of the gums.
In this case, the temperature does not necessarily have to rise or the child’s well-being deteriorates, as was the case with the growth of baby teeth. This is why the appearance of the first molars often goes unnoticed.
Helping your child replace teeth
The process of replacing teeth often takes place without pain or discomfort. The roots of baby teeth dissolve on their own, and the dental crown falls out freely. However, there are a number of recommendations that should be followed during this period.
The main one is systematic rinsing of teeth for disinfection purposes. This is necessary in order to avoid bacteria from entering the hole that will form at the site of the falling tooth. In addition, the sharp edges of a crown that has separated from the gum may cause minor damage to soft tissue. To prevent them from becoming inflamed, it is important to exclude any infection.
If your child experiences any pain during the tooth replacement stage, you should immediately consult a doctor. Under no circumstances should pain be eliminated using improvised methods.
Molars and prevention of their loss
Molars are stronger than baby teeth. However, they need proper care to prevent their loss, because new ones will not grow in place of a lost tooth.
Prevention of molar tooth loss involves proper oral hygiene. It includes systematic brushing of teeth, use of dental floss and mouthwash. In addition, you should carefully monitor the condition of your teeth and consult a doctor if even minor damage is detected.
Proper balanced nutrition is also mandatory. Especially in childhood and adolescence, you need to ensure that your body gets enough calcium and vitamin D.
Maxillary premolars
The crown of the premolars on the upper dentition has a prismatic shape. The buccal and palatal bones often have a convex surface. The first and second premolars in the row also have their differences.
First premolar
The difference between the first premolar of the upper jaw is the predominance of the vestibular surface over the palatal surface. Its contact surfaces are rectangular in shape. The buccal tubercle has two distinct slopes. The root of such a tooth often has a bifurcation.
Second premolar
In such a tooth, the buccal surface usually predominates over the palatal surface, which is more rounded. In most cases, this premolar tooth has a single cone-shaped root. However, there are also cases when it has a split.