High-quality restoration of contact chewing surfaces is the key to proper load on the teeth
When our teeth hurt or decay, all we want is to get rid of pain and discomfort, and also to protect them from removal. How the dentist will act in this case does not even matter to many patients. The main thing is that the work is done efficiently. But when it comes to the treatment and restoration of dental contact points, it is good to understand at least a little about the terminology and restoration methods that doctors use to carry out this incomprehensible procedure.
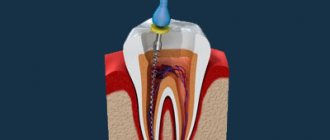
Checking the quality of work
After completing the anatomically correct contouring of the tooth, the marginal fit in the area of the gum wall is checked using floss, and the edges of the filling are probed.
It should be visually noticeable that the teeth are in contact with each other. The dental floss should pass with little effort into the interdental crevices.
When the thread passes without effort or visualization of the gap between them, they indicate poor-quality restoration of the contact point.
When the client talks about food getting between the teeth, and there are also problems with the movement of dental floss, then the tooth restoration needs to be redone.
The video provides additional information on the topic of the article.
Let's understand the terminology: what is a tooth contact point?
For many people, it is a mystery what the contact point between the teeth is. Let's figure it out.
Our teeth are located in the mouth in such a way that their lateral surfaces touch each other and thereby create a continuous arch, which is a single whole and forms a beautiful smile. This is provided that the person does not have any pathologies of the maxillofacial system or there are no missing units.
On a note! The contact point is easy to detect if you pay attention to the interdental spaces - they have a triangular shape in the gingival region, and the tip or apex of the triangle is directly facing the point of contact of the teeth.
If you open your mouth and look at its contents in the mirror, you will see that each tooth has a vestibular, i.e. on the external, visible side, in addition to the most frontal coronal part, there is a cutting edge, a neck and two contact (they are also called “proximal”) surfaces on each side, i.e. these are vertical areas facing neighbors. In those places or points (as a rule, these are the convex parts of the lateral surfaces of the crowns) where the tooth comes into contact with neighboring units, a contact point is formed. Incisors, canines, premolars always have two adjacent contacts on both sides (medial and distal) and only the outer molars in the row have only one such contact point (we are talking about sevens or eights, i.e. wisdom teeth, if you have any There is).
It is important to understand that there are several contact surfaces - lateral (one or two), as well as chewing ones. But it is the contact point that is called the lateral surface in the area of the apex of the crown of a living tooth.
Types of contact points
Experts distinguish only two types, characterized by the peculiarities of the fit of the two proximal surfaces of neighboring units.
The first one is point. This type of contact is typical for children who have recently erupted teeth and for young adults. The crowns themselves in the area of contact have an almost ideal round or spherical shape, so they interact with each other only pointwise.
The second is planar. This type is typical for mature and elderly people, because... Over the course of life, the enamel gradually wears out and wears out, and the coronal part in the lateral areas gradually becomes flat as a result of friction and physiological mobility of the units. As a result, the lateral surfaces of neighboring teeth are no longer limited to point interaction, but have quite pronounced proximal areas or points.
Why are contact points needed?
The functions of dental contact points cannot be underestimated, because the health of the oral cavity as a whole, the condition of the maxillofacial system, and the aesthetics of a smile depend on their correct structure and location.
So, let's take a closer look at what having an anatomically correct contact point gives:
- the teeth are able to lean on each other and provide each other with support,
- each unit occupies its designated place in the row and is protected from loosening and displacement,
- in the presence of a contact point, a correct redistribution of the chewing load occurs: when a load is applied to the tooth during chewing, its coronal part is deformed due to a reduction in height and expansion in different directions. As the crown expands, the load is transferred throughout the row through the contact surfaces,
- The gingival papillae that fill the interdental spaces remain protected from food particles and injury.
If you have caries or, due to various circumstances, damage to the contact point occurs, then any irritant can cause the development of an inflammatory process on the gingival papillae. The same food debris that gets into the interdental spaces can injure the delicate mucous membrane and provoke a disease such as gingivitis. If the problem is not given attention, gum inflammation will be complicated by periodontitis, mobility, displacement, loosening and even tooth loss.
Also, if the anatomically correct contact of the lateral surfaces of the teeth is disrupted, one of them may eventually receive excessive occlusal load or pressure during chewing food and quickly begin to collapse. A characteristic sign indicating functional overload is vertical cracks in the enamel. The same traumatic occlusal load on the maxillofacial apparatus is characteristic of people who have had part of their teeth removed or lost, but are in no hurry to restore them, get prosthetics, or do implantation.
Contact point in dentistry: what is it, why are matrix systems installed between teeth?
Disturbances of the contact point between proximal surfaces represent a serious problem for oral health. Pieces of food get stuck in the interdental space, which serve as a breeding ground for bacteria.
Caries develops on teeth adjacent to each other, and problems with gums and periodontium arise. Contact restoration is carried out using matrix systems.
Dentists use several methods to reconstruct the proximal area: the sandwich technique, the Berlotti technique, and the use of a ductile composite.
Concept and functions of a contact point
What is a contact point? This is the point of contact between two teeth located next to each other in the jaw. The approximal surface is divided into three parts: chewing, median and gingival. The contact is located in the area of the chewing and middle parts. On the lower jaw it is on the central line, and on the upper jaw it has a buccal deviation.
Functions of the contact area:
- prevents food particles from getting stuck;
- ensures row integrity;
- evenly distributes the chewing load;
- protects the interdental papilla from injury;
- prevents deformation of the jaw bone.
Types of matrices and fixation systems
In order to qualitatively and professionally reconstruct the proximal surface, matrices are used in dentistry. They are needed to prevent the filling mass from leaving a limited area, help restore the proximal wall and protect the interdental papilla.
The table shows the classification of types of matrix systems:
| Basis for classification | Types of matrices | |||
| By shape | Flat | Anatomically sculpted | Contour | |
| Ribbons | Stripes | Ring | Sectional | |
| By material | Polymer | Metal | Combined | |
| Lavsan | Polyester | Titanium | Steel | Metal-polyester |
Types of matrix holders:
- spring – used for perforated matrices;
- sectional system “3M” with spring rings;
- with built-in retainers for restoration of premolars and molars.
Installation is carried out using a plugger, a trowel and other tools. Wedges are used to create interdental space. They come in plastic and wood.
Materials and methods for restoring a contact point
To reconstruct the contact, the dentist uses one of several treatment methods:
- Sandwich technique. The filling is applied in two layers - glass ionomer cement is used for dentin, and a composite is used for enamel. The technology is suitable for treating areas at the root, filling deep carious cavities and pulpless areas.
- Tough composite. It is used using active and passive technology. Active is used in narrow spaces. The filling material is applied to the walls in a thin layer and cured with light, then a composite is applied, which under pressure fills the area limited by the matrix. Passive technology involves the application of a composite and its polymerization.
- Berlotti method. After polymerization of the adhesive material, a chemically hardened composite is introduced into the pulp chamber. The remaining cavity is filled with a light-curing composite and polymerized.
Restoration quality control
After contact is restored, the dentist checks the quality of the work. He removes the remaining filling material, examines the interdental space and introduces dental floss. It is considered a good indicator if the floss passes between the teeth with little effort.
The restoration is subject to correction if a large gap is visible between the proximal surfaces, and the thread enters without additional obstacles. Repeated contact point reconstruction is required if the patient continues to complain of food entrapment.
Source: https://AzbukaZubov.com/protez/implant/matrichnye-sistemy-v-stomatologii.html
Why do contact surfaces fail?
Most often, the integrity of contact points and their anatomically correct location are violated due to the occurrence of a carious process in the adjacent areas and interdental spaces, which develops here due to inaccessibility and poor or insufficient oral hygiene. As mentioned above, the smallest pieces of food easily get into the spaces between teeth and get stuck; it is not always possible to clean them out on your own, and sometimes it is easy to notice. Moreover, the carious process in these areas can be difficult to identify independently, so it can remain unnoticed for a long time and progress, affecting several units at once. How to avoid this? Undergo preventive examinations in a timely manner. This should be done at least once every six months for adults, and 3-4 times a year for children.
Doctors, when faced with such defects, must not only take care of removing carious lesions and stopping the inflammatory process, but also begin restoring the contact point of the teeth during filling and prosthetics.
Basically, in their medical practice, dentists are faced with defects of class II and III caries according to the system developed back in 1986 by Black. The second class includes caries of the contact surfaces of molars and premolars, the third class includes the carious process on the lateral surfaces of the canines and incisors without disturbing the cutting edge. Class IV defects are also less common in practice, when not only the contact surface of the fangs and incisors is damaged, but also the cutting edge is destroyed.
Therapy services in dentistry Ilatan in Moscow
Tooth decay is the word we hear most often in the dentist's office. It is so familiar that it often does not cause any fear. They say, put a seal, and that’s the end of it. And few people know that caries is a rather complex disease, with its own characteristics and consequences.
Types of caries
According to the depth of the lesion and localization - the place of formation, the following types are distinguished, they are also stages of caries: superficial, medium and deep; cervical, fissure (in natural anatomical depressions), interdental, secondary.
This information is very useful for everyone to know, especially for those who do not like dentists with frequent visits. Without knowing the basics, you can easily confuse the onset of caries development with ordinary plaque and seriously trigger the disease.
Knowledge about this type of caries, such as secondary caries, that is, formed in a tooth that has already been treated and filled, will force you to approach the choice of a clinic more carefully, because secondary caries is, as a rule, the result of not entirely conscientious work by a doctor.
It is with the appearance of a white or dark spot on the enamel of teeth that caries begins. If you see a doctor right away, you can get by with minor casualties. A simple procedure like tooth remineralization will help stop the destructive process. If you don't catch it in time, caries can develop into pulpitis.
Pulpitis and periodontitis
Pulpitis is a complicated type of caries, destruction that has reached the pulp (nerve). Each of us has experienced the symptoms of the disease at least once in our lives: dull pain in attacks that gets worse at night, an acute reaction to cold and hot food. Of course, treatment of pulpitis in Moscow is a complex of more serious measures compared to the treatment of simple caries. The doctor removes the nerve, fills the canals, and restores the tooth.
The most difficult case is periodontitis. The nerve disintegrates, the tooth becomes mobile, the pain is sharp and unbearable, the temperature may rise, and even a cyst may form. To avoid an abscess, immediate medical attention, often surgical, is required. Treatment of periodontitis is often multi-stage with mandatory radiography, removal of the decayed nerve, cleaning and filling of canals, restoration and even prosthetics of the tooth.
- How to effectively treat periodontitis and pulpitis in dentistry Ilatan
Signs of destruction of contact points
Visually, the destruction of the lateral surfaces of the teeth or the presence of a carious process on them may remain unnoticed until a large cavity or black “hole” forms on the side of the crown. However, it is better if the problem is identified much earlier. To avoid missing it, pay attention to the following signs:
- painful sensations when eating food, temperature changes,
- food easily penetrates the interdental spaces and gets firmly stuck there,
- discoloration on the lateral parts of the crown: this sign can be detected quite easily if the front incisors and canines are damaged. The enamel stops shining, may acquire a white chalky tint, turn yellow or brownish,
- gingival papillae are inflamed and swollen,
- Bleeding gums began to bother me.
Methods for diagnosing the problem
Diagnosing a carious lesion in the area of the lateral surface of two teeth in contact with each other can be quite difficult even for an experienced dentist, especially if the units are crowded or closely located. That is why doctors sometimes use not one, but several different methods for diagnosing pathology:
- X-ray: it is always done because... with its help you can determine the depth of the carious lesion and the condition of the tissues surrounding it. In the picture, the carious areas will be black, the tooth itself will be gray, that is, much lighter than the inflamed area,
- digital method: using a special high-resolution video system, the doctor can transfer the image to his computer monitor, where he then comprehensively assesses the situation,
- Electroodontometry or EDI for short: allows you to identify the pathological process at the earliest stages of development. To determine the condition of soft and hard tissues, the doctor uses a special Diagnodent device that produces light pulses, which are then returned or reflected back. Based on the length of the pulse waves, the specialist determines the state of the areas under study. And the wavelengths in healthy and affected areas are completely different,
- transillumination: a special apparatus is also used for this, which literally illuminates all the examined areas. In those areas where the enamel-dentin layer is damaged or demineralized, the light takes on a different shade,
- colorimetry: here the patient is given to rinse his mouth alternately with different liquids. First use a methylene red solution, then use a glucose solution. In damaged areas, the PH level is changed and the acid-base balance is disturbed, so they “give” themselves a bright range of shades (yellow-red),
- vital staining: this procedure can be carried out only immediately after professional oral hygiene, then it will be most effective. The doctor applies methylene blue dye to the patient's enamel. The composition is kept for about 5 minutes, after which it is washed off with plain water. The result is painting in bright colors the areas where the carious process takes place.
Important! Before dental treatment or during a preventative examination, an experienced doctor will advise you to undergo professional oral hygiene - do not refuse this useful procedure. The procedure will help remove soft bacterial and hard plaque, which can serve as an obstacle to the correct diagnosis of various dental diseases and especially the diagnosis of caries in the proximal areas.
It is mandatory for doctors to conduct a visual examination using modern instruments. For example, endoscopes with bright LED lighting that transmit the resulting image to a monitor screen. In this case, the lateral areas of the teeth should be subjected to a comprehensive assessment, not only from the vestibular side, but also from the lingual, buccal, and occlusal side. A study is also carried out using a probe - thus, hidden carious lesions are detected against the background of bleeding of periodontal tissue.
Diagnostics
Diagnostics is the first stage in any qualified treatment and correct diagnosis. Often a simple visual examination is not enough, so the most effective methods are used:
- radiography and videography. Now this is the most popular diagnostic method, which makes it possible to identify the extent of damage and other invisible problems;
- electrical odontometry (EDI);
- diagnostic models;
- trans illumination method. When using this diagnostic method, the beams of the device with transmitted light reveal damaged tissue, changing color.
The electroodontic diagnostic method is similar to the previous one, but more accurate. Allows you to detect tissue damage and inflammation. Pulsed light waves examine the tooth and display the results on the monitor.
The main complaints of patients: swelling of the gums, pain, bleeding, painful reaction when exposed to hot or cold food (drinks).
Nowadays, special systems have been invented with the help of which dentists can detect even hidden caries. They display an image of the tooth on a computer screen. The “color” method of examination is also effective: vital staining and colorometric test. But this method requires professional cleaning to remove plaque. After treating the teeth with the necessary solution, the areas affected by caries are painted.
Tools used for restorations
Restoring a tooth that has a damaged contact point is not an easy task for a dentist from a technical point of view. Standard caries treatment and fillings are not enough here. In order to restore the complex anatomy of the contact surface, it is necessary to use a set of special tools and devices, the main of which are matrices and wedges. Let's look at them in more detail.
Matrices
What is a matrix? This is a device that performs a kind of protective or restrictive function and helps to apply filling material for restorations in the required quantity. Using a matrix, a specialist models the surface and contact point, avoiding excessive layering of material. This limiter also does not allow it to go beyond the anatomical contour of a particular tooth. The device also protects the gingival papilla during manipulations.
Modern matrices for modeling surfaces can be made of plastic, metal or metal-plastic, can have different lengths (short, medium, long) and shapes - straight, contour or conical, perforated (flat and curved) for molars and premolars, volumetric. There are separation, protective or contouring (for modeling) models.
To firmly fix the device, the doctor uses matrix holders designed for this purpose: rings and clamps, couplings and clamps.
Wedges
Wedges perfectly complement the matrices. They have several main goals:
- protect the gingival papilla and the adjacent tooth from damage during manipulations and contact with filling material,
- separate the unit being restored from its neighbor,
- increase interdental space for high-quality subsequent procedures,
- allow for a higher degree of fixation of the matrix,
- allows you to recreate a triangular hole in the gingival area during the restoration process.
Wedges are made of wood and plastic, just like the matrices have different lengths and widths. When installed, they adapt to the anatomical features of the tooth.
Experts consider the most optimal option to use wooden wedges made from maple, because They are hypoallergenic, do not injure the mucous membranes and, in addition, perfectly absorb excess moisture. However, plastic is more flexible and pliable than wood, so when the patient’s teeth are very closely spaced and crowded, doctors prefer to use plastic wedges.
To facilitate work with proximal surfaces and for reliable and complete polymerization of filling materials in such difficult-to-reach areas, doctors also use the latest generation equipment. For example, a light-conducting cone that helps ensure polymerization of the composite. Tools and light-conducting attachments with built-in light sensors - with their help you can easily see the deepest cavities.
Medical Internet conferences
Relevance. Despite advances in the treatment of approximal caries, this disease still occupies a leading position [1]. Caries of contact surfaces of teeth is one of the main problems of modern domestic therapeutic dentistry. The greatest difficulty is filling cavities of class II according to Black and creating a contact point. This is due to difficult access, the location of the carious cavity, often in the subgingival area, thereby requiring certain skills from the doctor, the availability of special tools and materials, making restoration quite labor-intensive.
Goal: search for the most successful methodology and materials for restoring the contact point.
Tasks:
1. determine the role of the contact point in the normal functioning of the dental system;
2. emphasize the importance of hygiene of contact surfaces of teeth and conduct a sociological survey on the topic “Interdental hygiene products”;
3. study the tools and materials used to restore the contact point;
4. analyze the basic methods of filling cavities of class II according to Black;
5. restore the contact point on the model using various tools, matrix systems and filling materials.
Materials and methods. A review of scientific articles, dissertations, books and teaching aids, epidemiological studies and statistical data was carried out. A sociological survey was also conducted; practical manipulations were performed to restore cavities of class II according to Black in teeth 2.5 and 2.6 on a model, restore the contact point using metal sectional (TOP BM) and lavsan matrices with an integrated tension device (Blue Lucifix® Molar Matries, Kerr), nanohybrid composite materials "Filtek™ Ultimate" and "Filtek™ Ultimate Flowable" (3M ESPE).
Results and discussion. The contact point is an important anatomical formation, the point of contact of the proximal surfaces of two adjacent teeth. In young patients, the contact point is in most cases point-like, while in older patients it is planar, which is explained by the physiological mobility of teeth and abrasion of hard tissues. On the upper jaw it has a buccal displacement, on the lower jaw it is located along the central line [5].
Role of the contact point:
- Provides a stable position of teeth relative to each other and in the dental arch;
- Promotes uniform distribution of chewing pressure;
- Protects the gingival papilla from damage.
According to WHO epidemiological studies, if in primary and mixed dentition caries is more often determined in class I (the so-called “fissure”), then in permanent dentition - caries of contact surfaces [1].
81.4% of patients aged 16-44 years have carious lesions on the approximal surfaces of teeth in the defect stage and 31.6% in the stain stage. Caries of this localization in 76.4% of cases is the cause of pulpitis or periodontitis [6].
On average, half of all restorations in this area are inadequate and are often accompanied by recurrent caries or inflammation of periodontal tissues [6]. The reason is known: the interdental space is a retention point that cannot be fully hygienized when using only a toothbrush and toothpaste. One of the main ways to prevent caries, including approximal caries, is proper oral hygiene. In order to remove soft plaque from the interdental spaces, interdental oral hygiene items are used: toothpicks, flosses, super-flosses, monotuft brushes, brushes and irrigators [1].
Among people who do not work in the field of dentistry and who are not students of the dental faculty, I conducted a sociological survey on the topic “Interdental hygiene items.” The age of the target audience is from 18 to 30 years. Of the 166 respondents, everyone is familiar with this concept. Of these, 37% received information from the media, 23% from parents, 17% from a dentist, 12% from friends, and the remaining 11% from various sources (Table 1).
Tab.1
Only 90% use these hygiene items: toothpicks - 40%; flossing - 8%; irrigator - 2%; the remaining 50% prefer the combined use of toothpicks, floss and brushes (Table 2).
Tab.2
To the question: “How often do you use them?” the following answers were received: “every day” - 46% answered; “1-2 times a week” - 36%; “once a month” - 7%; “very rarely” - 11%. The data obtained once again confirm the fact of the low level of prevention of contact caries.
Restoring the contact point is an important stage in the quality treatment of class II carious cavities according to Black. When recreating the complex anatomy of the contact area, interproximal spaces, embrasures, occlusal surface and marginal ridge, it is impossible to do without various accessories.
Tools for restoring a contact point can be conditionally divided into 2 groups: the main ones are matrices and matrix systems, matrix holders and elastic metal rings, wedges; additional - light-conducting attachments and special tools for forming filling material in the gingival area [2; 12-15].
The matrix serves as a boundary for the filling material and prevents its excessive layering beyond the anatomical contour of the tooth; conditions are provided for its condensation, as well as protection of the periodontal papilla from the pressure of the material. Currently, there are a huge number of matrices and fixing devices on the market [2]. Requirements for matrices:
• do not create obstacles during the formation of the filling;
• withstand pressure when applying filling material;
• do not deform under the influence of the wedge and fixing devices;
• protect the gingival margin from filling material;
• be located as close as possible to the adjacent tooth to create a dense contact point;
• have an optimal thickness of 50 microns.
In their practice, dentists are faced with various clinical cases of approximal caries, requiring an individual approach, both in the selection of matrix systems, filling materials, and in the choice of methods for restoring the contact point.
There are several ways to restore a contact point.
1. Sandwich technique:
• closed sandwich - “closed sandwich” - the contact point is created from a composite material, and the cavity is filled with glass ionomer cement to the enamel-dentin border.
• open sandwich – “open sandwich” - GIC restores part of the cavity up to the contact point, the rest with a composite. This technique is preferred in the following clinical situations:
– presence of a deep carious cavity;
– unsatisfactory oral hygiene;
– reduced caries resistance of the patient;
– presence of concomitant diseases, especially endocrinopathies [9].
2. Using a flowable composite as an adaptive layer:
• Passive technique (no pressure) - a flowable composite in a layer of up to 1.5 mm is applied to all walls of the cavity to the edge of the enamel, light-curing. First, the gingival wall is restored layer by layer with a composite of regular or packable consistency. The main cavity is filled layer by layer up to the tubercles. The supporting cusps (on the upper teeth - palatal, on the lower teeth - buccal) are restored more powerful, round, only fissures of the first order are restored. The guide cusps (on the upper teeth - buccal, on the lower teeth - lingual) are restored more sharp, with pronounced fissures of the first and second order [3].
• Active technique - used when there is a narrow gap between the gingival wall and the matrix. The first portion of the flowable composite with a layer of up to 1.5 mm is applied to all walls of the cavity to the edge of the enamel, with the exception of the gingival wall, and is light-cured. The second portion of the flowable composite is applied to the gingival wall and does not polymerize; A small portion of the composite of normal or packable consistency is applied on top and distributed with a plugger along the gingival and lateral walls. A flowable composite under pressure fills the narrow space between the tooth and the matrix, then the cavity is restored as usual [3].
To achieve tight interdental contact, in addition to wedging the teeth, it is necessary to hold the matrix in the desired position during polymerization of the composite.
3. Bertolotti technique. After polymerization of the adhesive, a chemical-curing composite is introduced into the cavity to 2/3 of its volume. The shrinkage of this composite will be directed towards the pulp and towards the soft tissues in the area of the gingival wall, because these areas have a higher temperature. Without waiting for the material to harden, the remaining third of the cavity is filled with a light-curing composite and polymerized [2].
4. Camus technique - a small amount of composite is polymerized at the tip of a trowel and placed into a cavity filled with uncured composite. While the doctor presses this piece against the matrix in the direction of the adjacent tooth, the assistant photopolymerizes the entire material [2].
Based on our own observations, it should be noted that dentists in their practice more often use: contour matrices - sectional metal and lavsan with a fixing device; wedges - wooden and light-conducting; elastic metal rings. And the most popular, in turn, are “active” and “passive” methods for restoring the contact point using a fluid composite as an adaptive layer [11; 16-19]. Therefore, the emphasis will be placed on them in the practical part.
Clinical picture: teeth 2.5, 2.6 - average caries class II according to Black (medial surface).
Materials used:
1) contour matrices - metal sectional (TOP BM) and lavsan with an integrated tension device (Blue Lucifix® Molar Matries, Kerr);
2) wedges - wooden and light-conducting (TOP BM);
3) chlorhexidine bigluconate 2% (TehnoDent);
4) gel for etching enamel and dentin “Travex-37” (Omega-Dent);
5) V generation adhesive system “Adper™ Single Bond 2” (3M ESPE);
6) nanohybrid composite material “Filtek™ Ultimate” and “Filtek™ Ultimate Flowable” (3M ESPE) [7].
Tactics:
1. Preparation of a carious cavity (Fig. 1, 2).
Fig.1 Fig.2
There are several types of access when preparing class II cavities:
⁻ occlusal approach with violation of the marginal ridge (used for extensive carious lesions);
⁻ occlusal approach with preservation of the marginal ridge (used only if the carious cavity is localized in the equator region or slightly lower);
⁻ buccal or lingual access with preservation of the marginal ridge (used when a small carious cavity is detected, localized in the equator or below);
⁻ direct access if the adjacent tooth is missing or preparation can be carried out directly through the carious cavity in the adjacent tooth [10].
According to the literature, the most common are iatrogenic damage to the adjacent tooth during surgical interventions on proximal lesions. Black also noted that when opening and performing mechanical treatment of class II cavities with rotating instruments, there is a danger of damaging the intact surface of the adjacent tooth. To avoid this complication, foreign authors recommend carrying out the so-called “preliminary wedging”. Before the final excavation of the dentin and after applying the rubber dam, a wooden wedge is inserted into the interdental space, and when the treatment is completed, the wedges are removed and returned to their place after installing the matrix [10].
2. Isolation of the working field. This stage was not carried out, since the restoration was carried out on the model.
3. Selection of matrices (Fig. 3,4).
Fig.3 Fig.4
4. Introduction of the contour matrix, its fixation and wedging of the teeth.
Tooth 2.5 - to restore the contact point on the medial side, a sectional metal matrix for premolars was introduced and fixed with a wooden wedge. It was not possible to completely insert the wedge, since the teeth in the plaster model do not have physiological mobility (Fig. 5).
Tooth 2.6 - a contour lavsan matrix with an integrated tension device is installed (Fig. 6). Additionally, it can be fixed with a light-conducting wedge.
Fig.5 Fig.6
5. Medical treatment of the cavity with 2% chlorhexidine bigluconate.
6. Adaptation of the matrix to the adjacent tooth.
7. Etching and application of adhesive system.
Etching enamel - 30 seconds, dentin - 15 seconds. Wash off for 30 seconds. Dry the cavity with a small sponge to avoid overdrying the dentin [7].
Then we apply 2 layers of the Adper™ Single Bond 2 adhesive system. Gently blow with a soft stream of air for 5 seconds. Photopolymerize for 10 seconds [7].
8. Applying an adaptive layer and creating a gingival wall.
Tooth 2.5 - application of the “active” method of restoring the contact point: the first portion of the fluid composite “Filtek™ Ultimate Flowable” (A2 Shade) in a layer of up to 1.5 mm is applied to the bottom and walls, except for the gingival one, and is light-cured. The second - on the gingival wall, does not polymerize (Fig. 7). A small portion of the “Filtek™ Ultimate” composite (A2 Body Shade) is added on top and distributed with a plugger along the gingival and lateral walls (Fig. 8), and photopolymerized.
Fig.7 Fig.8
Tooth 2.6 is a “passive” method of restoring a contact point: a fluid-flowing composite is applied to the bottom and walls of the cavity up to 1.5 mm thick and polymerized (Fig. 9). Then the gingival wall is restored layer by layer using a conventional composite; a contact point is formed (Fig. 10).
Fig.9 Fig.10
Important: in both cases, during polymerization, the matrix is “pressed” by the tool towards the adjacent tooth for the best adaptation of the material (Fig. 11, 12).
Fig.11 Fig.12
9. Layer-by-layer restoration with composite.
The “layered” restoration technique involves the combined use of light-curing adhesives of the 5th generation, “traditional” hybrid, liquid and condensed composites. In this case, the materials are combined in such a way as to make maximum use of all their properties [4]. A special feature of this technique is that if it is performed well, microleakage in the restoration is reduced to a minimum [8].
10. Removing the wedge and matrix from the interdental space.
11. Final polymerization.
12. Final contouring of the restoration.
13. Checking the edge fit and quality of the contact point.
Using floss, we check the formed contact point: the floss is inserted with difficulty, and a “click” is heard when it is removed from the interdental space.
Conclusions:
1. Contact point is an important anatomical formation that ensures a stable position of the teeth relative to each other and in the dental arch; promotes uniform distribution of chewing pressure and protects the gingival papilla from damage.
2. A sociological survey conducted on the topic “Interdental hygiene items” showed that only 60% of respondents adhere to adequate interdental hygiene, and the issue of preventing contact caries still remains relevant.
3. Despite such a variety of tools and materials existing on the market for restoring a contact point, the most popular are:
• contour matrices (sectional metal; lavsan with a fixing device);
• wedges (wooden and light-conducting);
• GIC (if it is impossible to isolate the working field; poor oral hygiene; low caries resistance or general somatic pathology);
• fluid-flowing composites and composites of regular or packable consistency.
4. “Active” and “passive” methods for recreating a contact point using a flowable composite as an adaptive layer are the most common.
5. When restoring the contact point in teeth 2.5, 2.6, the above materials and techniques were used. When properly selected and installed correctly, they really help achieve excellent results in a variety of clinical situations.
What types of matrices are better for modeling contact points?
It is impossible to answer this question unambiguously, because... the matrix must be selected based on many different factors. Depending on the clinical situation, the amount of work (macro- or micro-restoration is required), the stage of the procedure, the shape of the tooth and the anatomical features of the maxillofacial system, the doctor chooses one or another type of auxiliary instrument.
In the late eighties and nineties, doctors in their practice used cutout matrices to model contact points. But this device has shown its inconsistency over the years and is almost never used today, because such a matrix did not provide sufficient protection of the tooth neck and subgingival space from penetration of the composite there. And this situation often later became the cause of the development of chronic gingivitis. Today, this type of matrix is rarely used and only on the condition that the neck of the tooth is first coated with sealant.
In medical practice, there are also known methods according to which doctors completely refused to use auxiliary tools, namely, did not use wedges and matrices, or even rubber dams or rubber dams in their work. For example, the modeling method with sawing of contact surfaces implied the application of a composite material with a transition to the proximal surfaces. After this, the teeth in contact with each other were separated using an abrasive strip that resembled a hacksaw. This method also showed its inconsistency.
Today, some doctors prefer to use volumetric matrix modeling, because... they most accurately allow you to recreate the shape and anatomy of natural contact points.
Material and types of restoration
The following materials are most often used for restoration in dental practice:
- amalgam masses;
- chemically curing and photo-curing composite;
- combination of a composite with compomer or glass ionomer substances.
These are the main filling materials used when working with second class cavities. To reduce shrinkage within the filling, it is possible to fix ceramic inlays of different sizes. In this case, various techniques are used.
Sandwich technique
The filling is applied in two layers. The main part of the cavity is restored with glass ionomers. The contact point itself is made of composite or alloys.
The use of the open sandwich technique (involves the use of fluorine-releasing materials) is applicable in the following cases:
- the cavity damaged by caries is very deep;
- the patient neglects oral hygiene procedures;
- The patient’s resistance to caries is extremely low;
- disruptions in the patient's hormonal system.
Using a malleable composite
The filling is created in two ways:
- A passive technique in which pressure is not used. The flowable composite is applied in a layer of about a millimeter to all walls of the prepared tooth up to the very edge of the enamel, then it is light-cured.
The gingival wall is restored layer by layer. In this case, the supporting cusps (palatal or buccal) during restoration come out more powerful and rounded, and the guide cusps (buccal or lingual) are made sharper. - Active method used when the gap between the wall at the gum and the matrix is quite narrow. First, the viscous composite is applied, as in the previous case, and light-cured.
Next, another portion of the same substance, a little more than a millimeter thick, is applied to the gum wall. It is not polymerized; a little material is applied on top and distributed on all sides.The pressure forces the flowing polymer to fill the small void between the matrix and the tooth, then treatment proceeds according to the standard scheme.
Bertolotti technique
A chemically curing composite is placed into the restored area on two-thirds of the reconstructed surface, after photopolymerization of the material at the restoration site.
The shrinkage of this material goes to where the temperature is higher (pulp and gum area). The remaining void is filled with a photocurable substance.
Camus technology
Camus and colleagues suggest curing a little of the composite first. This piece is then inserted into the cavity filled with uncured filling material.
The doctor presses the already polymerized piece, directing it to the adjacent incisor or molar , and his assistant is engaged in the polymerization of the entire filling material.
What service life can you expect when placing an anchor pin in a tooth, and what factors can shorten the service life of the product.
In this publication, we will discuss the pros and cons of restoring a tooth with a fiberglass post.
Here https://www.vash-dentist.ru/krasota-i-uxod/narashhivanie/hudozhestvennoy-restavratsii-zubov.html you will find objective reviews about artistic dental restoration.
Preparation for the contact surface restoration procedure
First, the doctor carries out professional hygiene and antiseptic treatment of the oral cavity, puts the patient under anesthesia, and installs a rubber dam. Next, the specialist selects the necessary types of wedges and wedges two adjacent units. The wedge is always inserted from the tongue side, and the second end after installation should become noticeable from the vestibular side. After installing the wedge, you need to wait about 5-10 minutes so that the interdental space becomes clearly visible and nothing interferes with high-quality work.
Then the doctor opens and disinfects the carious cavity and removes the affected tissue. It is especially important to remove damaged tissue in the gingival area, because If this procedure is not carried out carefully enough, then there may subsequently be a risk of developing recurrent caries. Often in such cases, it is necessary to treat not just one, but several adjacent teeth, whose contact surfaces are in contact, for caries.
Next, depending on the clinical picture and indications, the doctor selects and fixes the matrix system, conditions the prepared cavity using special gels and applies an adhesive composition, after which he selects a technique for restoring or restoring both the tooth itself and its contact point with the neighboring unit.
What are the ways to restore contact cavities of teeth?
Answered by Ryzhov Artyom Vyacheslavovich orthopedist, surgeon, implantologist
If previously, in the treatment of dental caries and its complications, it was enough only to replace the defect of hard tissues with the help of filling material (silicophosphate, silicate cements, amalgams), now the tasks facing the doctor have become more complicated. For example, during treatment, it is no longer enough to just replace the defect and restore the anatomical shape of the tooth. It is also necessary to prevent the development of complications (recurrent caries, etc.), restore and sometimes improve the aesthetic parameters of the tooth, restore the functional value of the tooth and its biomechanical characteristics.
Features of restoration of chewing teeth
When carrying out aesthetic restoration of lateral teeth, the most important task is to restore their anatomical shape. This is due to the fact that dental tissues and tissues surrounding the tooth constitute a very complex biomechanical structure that ensures the perception, distribution and absorption of cyclic chewing load. A tooth is a mobile, dynamic structural system that deforms when a load occurs and completely returns to its original state after the load is removed. The form of deformation of the tooth crown is a decrease in height and an increase in diameter. It is believed that it is through the expansion of the crown that the chewing load is distributed in the dentition to adjacent teeth.
Defects in dental tissues disrupt the integrity of the biomechanical structure, interrupting the paths for absorbing chewing load, and are stress concentrators. Subsequently, as a result of cyclically repeated loads, local fatigue of dental tissues occurs and microcracks are formed in places of excess stress, which, merging with each other, form fractures of the tooth structures.
Typically, patients with a fracture of the tooth wall or a chipped restoration say that the “breakage” occurred as a result of a slight chewing load. This is true, because the fatigue of dental tissues and restoration material formed in the area of excess stress over a long period, and a slight chewing load, which provoked the fracture or chip itself, was only the “last straw” (Radlinsky S.V., 2006).
Therefore, a restoration that is incorrectly performed from an anatomical point of view can lead to the development of various kinds of complications (chips of the restoration, chipping of the tooth crown, etc.).
Restoring a contact point
In his practical work when treating chewing teeth, the doctor most often encounters class II defects according to Black. The most difficult problem is the restoration of the contact point. Let us recall that it is necessary to recreate the following elements: 1) the contact slope of the marginal ridge; 2) the actual contact point; 3) a triangular-shaped hole in the gingival area, which is formed using wedges (wooden, plastic, etc.). The actual contact point is created by using matrices (metal, plastic, etc.) and various matrix systems. In this case, the thickness of the matrices used should be taken into account. It should be noted that if the width of the natural contact point is about 10 microns, then metal matrices have an average thickness of about 35-40 microns, and plastic ones - 50 microns. Therefore, it is important to select the right matrices depending on the specific clinical situation and be sure to wedge the teeth, especially when restoring mesio-occlusal-distal cavities, when it is necessary to use matrices on both sides of the tooth.
To facilitate the restoration of the contact point, proximal faces, and for deeper and more complete polymerization of the composite material, special devices and tools have been developed [2]:
1. Light-conducting cone - Light Tip (Denbur), which has 4 main sizes, is made of plastic and is placed on the light guide of the polymerization lamp. The use of a cone allows for deeper polymerization of the composite material in difficult-to-reach areas - the gingival wall, in places where the filling material adheres to the matrix. In addition, the light cone can be used to press the filling material against the inner surface of the matrix and thereby form the approximal surface of the tooth.
2. The Contact-Pro 2 tool (CEJ Dental) allows you to create interproximal contact points on the mesial and distal surfaces of molars and premolars. The tool is a handle with double-sided working structures made of light-conducting material. The working part is installed at the bottom of the tooth cavity. Ergonomically positioned light cones placed at the ends of the instrument provide light to the deepest areas of the cavity.
3. The Optra Contact tool (Ivoclar Vivadent) allows you to create a contact point from a composite material with a spacer on the inside of the matrix.
4. The LM-MultiHolder system (LMInstruments) consists of attachments of various shapes, which are made of transparent plastic and are light-conducting.
5. To restore the contact point, in our work we most often use the incrementation technique, aimed at reducing the polymerization shrinkage of the composite. Its essence is as follows. First, the matrix system is installed and the teeth are wedged. Then, after conditioning and application of the adhesive, a composite with increased fluidity is applied to the bottom and walls of the cavity and is photopolymerized. The second portion of the composite with increased fluidity is applied to the gingival wall and lateral edges of the cavity; photopolymerization of this portion is not carried out. At this time, a pea is formed from the composite material outside the oral cavity, which in size corresponds to the diameter of the cavity in the area of the contact surface. Polymerization of the pea is also carried out outside the cavity, for example on a sheet of notepad. Next, a finished pea made of the composite is introduced onto the contact surface, which is photopolymerized together with the composite of increased fluidity. Then the cavity around this pea is filled. In this case, a marginal ridge approximately 1.5-2 mm thick is formed. Thus, the class II cavity is transferred to the class I cavity.
As a result of filling using the incremental method, shrinkage of the composite on the contact surface occurs outside the tooth. Next, you can remove the fixing ring of the matrix system for better access to modeling the occlusal surface of the tooth. During restoration, opaque shades are used mainly, and enamel colors are used only at the final stage.
Clinical example
Patient T., 24 years old, came to the clinic for oral sanitation.
After the examination, a diagnosis was made: tooth 25 had chronic fibrous pulpitis, tooth 24 had caries (Fig. 1).
After infiltration anesthesia Ubistesini Forte 1.5 ml, cleansing the surface of the teeth from pellicles with Clint paste (VOCO), the color of future restorations was determined. First, a rubber dam was applied, the failed restoration of tooth 25 was removed, and endodontic treatment was performed (Fig. 2). After establishing the matrix system, a base lining made of glass ionomer cement “Ionofil Molyar” (VOCO, Germany) was applied, and the tooth crown was restored from the nanohybrid composite material “Grandio” (Fig. 3). We would like to note that the Grandio nanohybrid composite does not have a number of disadvantages inherent in most composite materials. The material adapts well to the cavity even without the use of a high-flow composite, and also does not stick to instruments, which ensures comfortable work. In addition, “Grandio” has good handling characteristics: it is easily introduced into the cavity, is perfectly modeled, is well polished, and has the highest color fastness, which is achieved due to the hydrophobic properties of the monomer: restorations from “Grandio” do not change color for a long time under the influence of food dyes (tea, coffee, red wine, etc.), as well as cigarette smoke.
Materials for restorations
To recreate contact surfaces, doctors use different materials: hybrids, nanocomposites and composites of increased fluidity, compomers, glass ionomers, amalgam. A combination of composite and GIC is often used.
Flowable composites are characterized by a high degree of wear resistance, are well suited for surface modeling and can be polished, are elastic, easy to mix and conveniently applied using special dispensers.
As for compomers, they contain fluorine, which helps strengthen and regenerate hard tissues. This material is very resistant to moisture and has a high degree of adhesion.