The presence in the jaw row of an element that has passed the stage of formation, but has not yet taken its proper place, as a rule, is a reason to visit the dental clinic. In most cases, an unerupted tooth does not cause physical inconvenience, but an aesthetic problem arises in the form of an edentulous area that confuses interlocutors and causes psychological discomfort. In addition, if an unerupted tooth is left “as is,” the risk of suppuration and subsequent health problems increases. The solution to the problem is orthodontic teeth traction.
What is an impacted tooth?
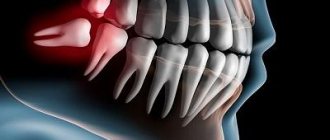
Retention is an abnormality in tooth eruption, in which the tooth erupts partially or remains completely in the tissues of the jaw.
An impacted tooth is a tooth that has failed to erupt and “sleeps” in the gum or even in the jaw bone. There are cases when only part of the tooth crown erupts and is visible, and the rest of the tooth is covered by the gum - such teeth are called semi-impacted.
Most often, impacted canines and wisdom teeth are found - the notorious eights, but there are cases of impaction of the central and lateral incisors, and the first - a little more often.
Symptoms
If the molar has partially erupted, the symptoms are expressed in constant injury to the tissues adjacent to it. The mucous membrane becomes hyperemic and edematous. The surrounding tissues become inflamed, and the patient develops pericoronitis or gingivitis. A partially impacted tooth is almost always removed. The pathology can also be asymptomatic. It is discovered by chance during examination. An objective sign is the absence of a unit in the arc. If the unit is immersed in the tissue, this is determined by the protrusion of the gum, and upon palpation its parts or contours are diagnosed.
The patient may notice displacement of the units when pressure is applied to them by the pathological molar. In such a situation, resorption of the roots occurs, the patient feels pain and discomfort when opening the mouth and chewing. In such a situation, caries and periodontitis, as well as pulpitis, often develop. Irritation of nerve endings and fibers leads to pain, paresthesia, and trigeminal neuralgia. If the wisdom tooth lies horizontally in the gum, the patient feels full. In this case, cysts with suppuration, periostitis, pericystic osteomyelitis, abscess or purulent sinusitis are formed. Inflammatory processes are accompanied by fever and general ailments.
What are the types of tooth impaction?
There are two types of retention - partial, in which part of the tooth is visible from the gums, and complete - in which the tooth is completely located under the gum tissue and/or jaw bone.
Such teeth can also be positioned differently, both being in “their” place in the dentition and occupying an incorrect position outside the dentition.
- Vertical
- Horizontally.
- At an angle to the jaw
If a tooth does not erupt in the right place beyond the border of the dentition, they speak of tooth dystopia.
There are even reverse retentions, when the tooth lies “upside down,” that is, upside down with its roots.
There may be only one impacted tooth in the dentition, or two impacted teeth may be located symmetrically. This problem concerns both milk and permanent teeth.
When is tooth root removal required?
Dentists prefer to resort to such radical methods as rarely as possible and try to keep the dentition “alive.” Even if a small fragment remains, the possibility of prosthetics using the preserved base is first considered. In some cases, extraction cannot be done without.
Indications:
- The patient is diagnosed with periodontitis in the later stages, when the root part is severely loosened;
- serious injury (fracture);
- a cystic neoplasm has been discovered that cannot be eliminated in isolation;
- a piece of the crown broke off, extending deep into the gum tissue;
- solid particles remained after poor-quality doctor intervention.
How is a tooth root removed in dentistry in children? Is this necessary? Milk units normally fall out on their own. They are indicated to be pulled out in cases of deep carious lesions, fractures, loosening and subgingival caries.
What happens if you leave
Some people can walk for several years with their teeth completely destroyed. This is very harmful, because the remaining root part rots and is a source of foul odor from the mouth. In addition, this is a hotbed of numerous infections, because the roots accumulate pathogenic microorganisms and food particles. Dense plaque and tartar form on the fragments. As a result, soft tissues become inflamed.
The body will constantly fight the source of the problem; the immune system will direct a significant part of its resources to the fight. Sooner or later, a severe inflammatory process develops; in the most severe cases, the maxillary sinuses become infected, osteomyelitis develops, and fractures and other injuries are possible.
Patients mistakenly believe that over time the root will come out on its own, so dental intervention is not necessary. The root part does not fall out, over time it will become overgrown, and the doctor will have to cut the gum for high-quality extraction. In this case, the rehabilitation period may be delayed.
What complications do impacted teeth cause and why do they need to be “extracted”?
It is difficult for the patient to immediately understand what danger “hidden” teeth can pose, but it is really serious.
Semi-retinated teeth cause inflammation of the “hood” with which they are covered and adjacent tissues, and this provokes purulent inflammation.
Fully impacted teeth that lie in the jaw can behave like a foreign body; they put pressure on neighboring teeth, causing their displacement and a number of other problems.
In this case, the patient experiences pain and fever in case of inflammation, a feeling of pressure and discomfort in the jaw, neuralgia or numbness of part of the face.
If we list the diseases that can result from impacted teeth, it will become clear that this is a real “time bomb” that can detonate at any moment.
What diseases can be caused by an impacted tooth:
- periodontal cyst,
- caries of neighboring teeth and their roots,
- pulpitis,
- pericoronitis,
- periostitis,
- periodontitis,
- purulent lymphadenitis,
- inflammation of the trigeminal nerve,
- odontogenic sinusitis,
- abscess,
- phlegmon,
- resorption (resorption) of the roots of adjacent teeth,
- bad habits: mouth breathing, infantile swallowing, inserting the tongue into a dental defect,
- problems with biting food,
- malocclusion, displacement of interdental contacts, crowding of teeth.
Possible problems
Pulling may be accompanied by difficulties, which are corrected as treatment progresses:
- Locks or buttons come off, so they are attached with special care to avoid repeated procedures.
- Rotating the crown by more than 90 requires accurate calculation of the trajectory of movement. Otherwise, the tooth may push against the roots of neighboring units.
- At the beginning of displacement, ankylosis may appear - fusion of the impacted tooth with the jaw bone. They can be separated surgically only with partial ankylosis. To prevent this problem from arising, carefully study the diagnostic results.
- When the pulling process is accelerated, resorption (absorption) of the root, surrounding connective and bone tissue is possible. Therefore, the traction force and the speed of movement are controlled by the orthodontist, who calculates the optimal treatment time.
How are impacted teeth diagnosed?
Impacted teeth are often “found” by accident during an X-ray diagnosis for another dental reason. If a patient asks about orthodontic treatment and is missing some teeth, or has symptoms that may be caused precisely by the presence of hidden impacted teeth, then a special diagnosis is carried out.
The problem of impacted teeth is solved by two specialized dentists - an orthodontist and a surgeon, so the patient will have to undergo diagnostics by an orthodontist and diagnostics by a surgeon. Most of the diagnostic procedures will be general, and the key is x-ray diagnostics, and it is preferable to do CT - computed tomography (3D diagnostics). Unlike an orthopantomogram (OPTG), it shows the spatial location of the impacted tooth in the jaw and relative to other teeth, which is very important for the surgical stage of traction - exposing its crown, because allows the surgeon to choose the optimal “approach”.
Indications and contraindications
The grounds, the presence of which is considered as a reason for carrying out the procedure, include:
- Genetic defects that appear during the development of the jaw apparatus;
- Premature loss of milk units;
- Long-term vitamin deficiency, as well as unnatural development of the jaw;
- Somatic weakening, poor-quality prosthetics and other factors.
The limitation for traction is the lack of free space in the jaw row, associated with displacement of neighboring units or damage. In addition, forced traction of an element around which there are no other teeth is considered inappropriate.
What to do if an impacted tooth is found?
There are 3 solutions to the problem of an impacted tooth:
- Orthodontic traction and placement in the dentition. This is often done with impacted teeth that are located in the smile zone - canines and incisors, provided that there is a place for them in the dentition and the tooth itself is healthy.
- Removal is a common fate for impacted eights, especially if the patient is undergoing orthodontic treatment. Very often, wisdom teeth erupt partially – this provokes inflammation and complications. Even a completely impacted (“hidden”) tooth serves as a potential source of caries, tooth displacement, and instability of orthodontic treatment. There are many reasons - there is only one verdict: it is better to delete it. Other indications for the removal of different types of impacted teeth are cysts, signs of inflammation, lack of space in the dentition, destruction of the neck of the tooth, caries.
- Preservation and surveillance. It is justified when the patient has no problems with the place in the dentition or bite, orthodontic treatment is not required, the tooth does not provoke complications and its absence does not spoil the aesthetics of the smile. Such teeth are observed; in case of the slightest problem, they are recommended to be removed.
How to pull out and place an impacted tooth in the dentition?
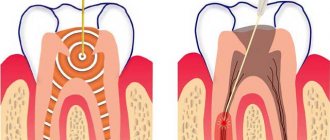
In some cases, if the root of an impacted tooth has not yet formed and there is an obstacle to its eruption, then removing such an obstacle is enough for the tooth to come out of the gums and take its place in the dentition. If the tooth root is already formed, this method will not help.
To “get” and move a fully formed impacted tooth into the dentition, treatment is carried out in 3 stages. Here we present the “classical” scheme, because in individual cases there may be deviations from this scheme.
- Preparatory orthodontic stage - you need to prepare a place in the dentition to which the orthodontist will move the extracted tooth. To do this, a braces system is installed, which aligns the teeth in the dentition and frees up the necessary space.
- The surgical stage is the image of the crown of an impacted tooth, on which a bracket or button is installed to transmit force from an arch or elastic element.
- The main orthodontic stage, during which the impacted tooth is pulled out and placed in its “rightful” place in the dentition.
Braces design
At first glance, braces look quite simple, but in fact the design is a complex mechanism. All its components are involved in the gradual movement of units of the dentition. In this case, the teeth can move in any direction, as well as around their axis, without changing the original inclination of the root. Braces act as delicately as possible, preventing injury to soft tissues and the tongue. As a result, a person becomes the owner of not only a beautiful smile, but also a healthy body as a whole.
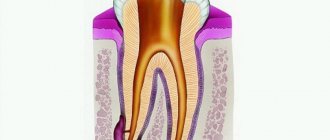
Many patients are surprised how they manage to dislodge a tooth, because it sits tightly in hard, bone tissue. In fact, the connection between the tooth and the jaw joint is not very strong. The tooth is held in its socket by the surrounding fibers, which constantly stretch and compress. Under pressure, the tooth can only move as far as the fibers allow. In this case, on one side the tissues will gradually shrink, and on the other they will begin to stretch. New bone tissue will begin to form in the freed space.
The designs themselves consist of many elements: locks, ligatures, arcs. The staples are attached to the surface of the enamel using a special dental glue, the excess of which is removed after installation. The arc is inserted into special holes in the locks (grooves) and held in place with ligatures (small rubber bands). Also very popular are non-ligature models, in which the arch is secured with clip-on locks.
How is surgery performed to expose the crown of an impacted tooth?
- As a preliminary stage, preparation for the operation is carried out. The patient undergoes professional hygiene and sanitation to reduce the amount of infection in the oral cavity and speed up postoperative healing.
- The operation to expose an impacted tooth is performed under local infiltration anesthesia and is considered a fairly serious surgical intervention.
The operation to expose the crown of an impacted tooth and install an orthodontic element on it can be carried out according to 2 schemes:
I Delayed bracket installation.
- The mucous membrane in the projection of the crown of the impacted tooth is excised, the entire crown of the tooth is exposed, and a special tampon is installed in the wound.
- After 2-3 days, a button or bracket is installed on the crown of the exposed tooth, which is tied to the orthodontic arch and traction begins.
II Bracket installation during surgery
- The dentist-surgeon peels off a small mucoperiosteal flap and exposes part of the crown of the impacted tooth, onto which the locking element is immediately fixed.
- The bracket is tied to an orthodontic arch or additional devices.
- After installing the orthodontic element, the flap of tissue is placed in place and the wound is sutured.
The disadvantage of this method is that in this case, repeated surgical intervention is possible if the bracket on the tooth comes off.
After surgery, the patient is prescribed antibiotics and antiseptic rinses, if necessary, to speed up healing. Light, non-traumatic food is recommended.
Treatment with Damon braces
Orthodontist O.A. Baranova does not welcome the removal of healthy impacted teeth if diagnostics show that the tooth can be returned to its place by restoring correct dental contacts. During treatment with the help of a brace system, a place will be created for the normal position of the semi-impacted tooth.
To correct the bite, the Damon brace system, which is optimal in quality and cost, was chosen. More aesthetic ceramic braces were installed on the front teeth, which are almost invisible on the teeth.
Braces are installed on the teeth:
After installing braces, the patient visited an orthodontist once every two months to monitor and replace the arches. After normalizing the shape of the dentition, the orthodontist connected additional treatment with orthodontic elastics to create correct contacts between the teeth. Correct contacts are a kind of “calling card” of the completed treatment - it is the correct contacts that give the new bite stability, physiology and comfort for the patient. After removing braces, a retention stage is needed to maintain the results obtained. To do this, a wire retainer is attached to the lower teeth, and a mouth guard is made for the upper teeth, which is worn at night.