Indications
Indications for removal of the submandibular salivary gland are:
- chronic sialadenitis (inflammation);
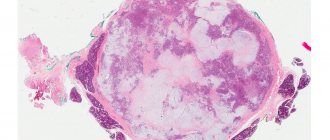
- benign or malignant tumors;
- multiple cystosis;
- salivary stone disease;
- severe injury to the gland;
- complete blockage of the salivary ducts with the impossibility of restoring their patency.
Depending on the diagnosis, various tests are prescribed before the operation - ultrasound, computed tomography or magnetic resonance imaging, chest x-ray. In the case of a tumor, a biopsy is also necessary to determine the nature of the formation. Salivary stone disease is examined using contrast sialography.
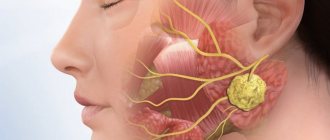
Submandibular gland
Removing the pancreas is an important surgical procedure. It is one of the two largest salivary glands in the human body, the other being the parotid gland. The most common reason for gland removal is due to recurrent infections and/or blockages that cause swelling (chronic sialolithiasis). Another reason is the presence of an abnormal mass contained in the gland (benign or malignant).
The pancreas and inflammation of the glandular ducts are the causes of swelling and, as a result, pain and discomfort. When a blockage occurs, backflow occurs, causing saliva to accumulate behind the occlusion. When this happens, the salivary glands swell in size. Over time (for example, between meals), the body resumes saliva production, and the saliva is compressed back and forth until the next meal, which activates the gland and produces more saliva, leading to the development of edema.
Initial (surgical) treatment is as follows:
Apply hot compresses to the widened area of the mouth two to three times a day. After applying the warm compress, give a very gentle (orthogonal) massage to the swollen areas.
Mix dry and sour candies. These sweets stimulate saliva production.
Increase your water intake to two liters per day. Try to avoid caffeine as it acts as a diuretic and can dehydrate the body.
The gland may or may not become infected. If there is inflammation, your doctor will prescribe an antibiotic, usually over a 3-week period. Use the antibiotic as directed and complete the full program even if symptoms subside.
Over the course of 3-4 weeks, the gland slowly returns to its normal shape. If the above precautions do not help, surgical removal is the next step.
If there is an abnormal mass, it may not change in size or even disappear. Unlike a blockage, swelling due to a mass does not change with food intake. Most masses grown in the submandibular gland are caused by benign tumors such as aphthoma or Warthin's tumor. These tumors are usually painless and move easily when palpated. Even if they are benign, tumors must be removed because they will not heal themselves and will continue to grow over time, causing facial distortion. Usually after decades, these benign tumors can also develop into cancer (carcinoma in pleural adenoma).
Unfortunately, some masses can be cancerous and include mucoepidermoid carcinoma, basal cell carcinoma, and metastases from skin cancer (squamous cell carcinoma is the most common). If there is pain, numbness over the chin or teeth, tongue or mouth, or facial paralysis, the likelihood that the mass is cancerous increases.
Typically, submandibular mass testing involves a CT scan as well as a fine needle aspiration (FNA) of the mass itself. Obtaining an FNA is useful in determining the extent of surgical removal. If malignancy is detected, a more extensive surgical procedure is required, including complete removal of the gland as well as surrounding lymph nodes (lymphatic clearance).
A common concern patients have regarding surgery is whether it will affect their saliva production. The answer is NO.
Sialolithotomy
In cases where there is a stone in the submandibular gland duct, an option you can try before removing the entire gland is a procedure called saliototomy. In fact, only the stone itself can be removed. If the stone is located near the mouth, this procedure can be performed at a local anesthesia clinic.
If the stone is more than 1.5 cm from the canal opening, the procedure must be performed in the operating room under general anesthesia. In this case, a small catheter is usually left in place to prevent scar tissue from closing the lumen and is removed after about 5 days.
Dangers of this process include infection and bleeding. A rare risk of this process is the development of scar tissue in the canal, which leads to recurrent swelling of the gland. There is also a small risk of numbness in the mouth.
Removal of submandibular glands
In cases where saliototomy cannot be used as an option or where a true mass exists, the entire gland should be removed. This is achieved by reducing approximately 3 cm below the body of the mandible to a length of approximately 4-5 cm. Anatomically, the omentum is prepared by carefully ligating the large vessels and preventing damage to the nerves. The defect is detected and it is ligated. The incision is closed with a plastic suture. The whole process takes about 1-2 hours.
Depending on how the surgery goes and how healthy the patient is, he may leave the clinic the same day or the next day. Surgical drains are usually removed within 24 hours and sutures 5-7 days after surgery. Pain after surgery is minimal, and in most cases people do not even need painkillers. Patients can eat as they please, but any exercise or heavy lifting is prohibited for the first 1-2 weeks after surgery.
Surgical risks include bleeding and infection. However, rare risks of subnuclear ablation include permanent lip paralysis, permanent tongue paralysis, and numbness in the lower part of the mouth.
Why is this happening? Because the nerves that go to the rim, tongue and larynx pass through the subeye and are at risk of injury.
Sometimes there may be temporary damage to the nerves and their function may return over time (weeks or months), but in some cases it may never return. The use of radio wave diathermy for vascular ligation and basal nerve conduction monitoring with a neurostimulator significantly reduces intraoperative and postoperative risk.
Endoscopic salnioscopy
Pancreatic endoscopy is performed by introspection, resulting in minimal (if any) incisions in the mouth or throat.
If you have problems with the submaxillary gland, please contact our clinic to schedule an appointment.
Preparation for the operation and features of its implementation
Preoperative preparation includes:
- laboratory tests;
- abolition of blood-thinning medications (at least a week before the procedure);
- changing your diet three days before surgery - excluding alcohol, spicy and rough foods, hot drinks.
- Smoking is also prohibited before surgery.
Removal of the submandibular salivary gland is a complex and specific operation, since its anatomical location near the nerve and choroid plexuses, muscles and other organs is associated with risks of serious complications. Such a procedure can only be performed by experienced specialists - dental surgeons or maxillofacial surgeons.
In the case of a malignant tumor, especially when it grows beyond the gland, the organ is removed along with the affected tissue of nearby muscles and lymph nodes. In other cases, only gland tissue is removed.
Surgery to remove the submandibular salivary gland can be performed in several ways:
- The traditional method is surgical excision of tissue with removal of the pathological gland. This type of operation does not require specific equipment, which explains its lower cost and speed of implementation. Postoperative wounds are quite large; the time for suture removal varies from 1 to 3 weeks.
- A microsurgical endoscopic operation that does not require large tissue intersections - all actions are carried out using manipulators, and observation is carried out using a probe that transmits an image to the screen. The great advantage of this type of operation is the targeted effect, due to which in case of salivary stone disease, benign tumors and cystosis of the gland, there is no need for its complete removal - only a small area of it is excised. After the operation, small marks remain, the stitches are removed after a few days. The disadvantage of this method is its high cost.
Prognosis of salivary gland cancer
Here are statistics based on various sources for general guidance. The term “5-year survival” refers to the number of clinical trial participants who were alive 5 years after treatment.
Salivary gland cancer is a rare disease, accounting for approximately 1% of the total number of malignant tumors. Most salivary gland tumors are benign.
There are 3 main and largest salivary glands and hundreds of small and insignificant ones. Cancer usually develops in the largest gland, the parotid gland, which accounts for 80% of cases. 2 out of 10 cases of salivary gland cancer occur in the submandibular and sublingual glands. Less than 1 in 10 cases develop in the minor salivary glands.
There are many different types of salivary gland cancer, the most common of which is mucoepidermoid carcinoma, accounting for 25-35% of all cases.
Summary statistics
As with many types of oncology, the prognosis of salivary gland cancer is determined by the stage of the disease, the degree of malignancy and the type of cancer.
In general, for all types and stages of salivary gland cancer, 75% of women and 60% of men have a 10-year survival rate after diagnosis.
Outlook by type of salivary gland cancer
There are many different types of this type of cancer, some of them very rare. This creates difficulties for analysis and conclusions because they are based on results from a small number of people.
There is a 5-year survival rate for the following types of disease:
- In adenoid cystic carcinoma - in 78% of patients.
- With mucoepidermoid carcinoma - in 80%. If the tumor has a high degree of malignancy - in 20-40% of patients.
- In acinar cell carcinoma – in 80-90%.
- For adenocarcinoma and mixed tumors – in 50%.
- For squamous cell carcinoma – 25%.
Perspectives on the stages of cancer of the major salivary glands. For the early stages, the prospects are generally quite good.
- At the first stage, 90% of patients have a 10-year survival rate.
- At the second stage, 75% of patients have a 5-year survival rate, 70% have a 10-year survival rate.
- At the third stage, 70% have a 5-year survival rate, 50% have a 10-year survival rate.
- At the fourth stage - the worst prognosis. 40% have a 5-year survival rate, 30% have a 10-year survival rate.
Statistics for malignant tumors of the minor salivary glands
This is a very rare type of oncology, accounting for 1%. Accordingly, it is more difficult to find statistics here, and the numbers are less reliable. On average, 50-60% have a 10-year survival rate.
- At stage 1, 80% have a 5-year survival rate.
- At stage 2 – 70% have a 5-year survival rate.
- At stage 3 – 60% have a 5-year survival rate.
- At stage 4, 30% have a 5-year survival rate.
It is important to remember that there are no statistical data based on which one can assume events for each specific case. The rate at which the same disease develops varies from person to person. Many factors determine treatment and prognosis for salivary gland cancer. Only the attending physician can give the most optimal option.
After treatment for salivary gland cancer, a full course of rehabilitation helps to achieve maximum effect.
Performing surgery to remove the salivary gland
With the traditional method of surgery, the patient assumes a lying position with his head thrown back and to the side. The operation involves local infiltration anesthesia. Several parallel incisions are made in the submandibular area, the tissue is lifted, and the capsule of the salivary gland is discovered, which is opened, and the gland tissue is extremely carefully removed and removed. When a malignant tumor grows together with nearby tissues, the latter are also removed. After this, stitches are applied.
During endoscopic surgery, both local and general anesthesia can be used. Through small punctures in the tissue, manipulators and a video probe are inserted, which projects all the actions performed on the screen. When the manipulators reach the gland, small incisions are made with their help, through which pathological tissue is removed. The endoscopes are then removed and sutures are placed at the puncture sites.
Postoperative care of the surgical site includes:
- hygiene - no water or dirt should get into the wounds;
- special diet - the diet will consist of semi-liquid warm food, no hot or cold drinks, no alcohol;
- smoking ban;
- special treatment - it is recommended to regularly treat the seams with antiseptics, and the oral cavity after each meal should be rinsed with a mixture of antiseptic and water.
If all the recommendations of the attending physician are followed, complete wound healing occurs within a few months.
Contraindications for sialectomy
The impossibility of adequate removal of the salivary gland is observed in case of malignancy of the tumor, deep involvement of nearby soft tissues, lymph nodes, and bones. Your veterinarian may suggest alternative treatment with anticancer drugs and radiation therapy.
Both methods show a high degree of effectiveness, but are detrimental to the health of the body. The operability of neoplasms is first determined, and only after that non-invasive treatment of cats and dogs (chemotherapy, radiation) is considered as the main method of eliminating the tumor process.
Types of surgical operations
When problems with the functioning of the gland are detected, the doctor’s main task is to preserve the glandular tissue.
There are the following types of operation:
- endoscopy is the most gentle operation, which is prescribed in the presence of a stone-like stone in the lumen and narrowing of the duct;
- resection, prescribed for the purpose of excision of a cyst, a tumor-like formation of a small volume;
- extirpation is an intervention necessary to remove a malignant neoplasm along with nearby lymph nodes, part of the facial nerve, skin (sometimes with bone tissue).
The features of the intervention differ depending on the location of the affected area.
Removal of the submandibular gland
The organ is removed through external access, cutting the skin in the chin area.
After excision, the wound is sutured. To reduce swelling and prevent the accumulation of pathological fluid, a drainage tube is inserted into the incision, through which the exudate comes out. The drainage is removed after 2-3 days.
If the reason for removal is the presence of a tumor-like neoplasm, the excised biological material is sent for histological examination. This will determine the nature of the growth and the presence of malignant cells in it.
The duration of the operation to remove only the affected organ is up to 40 minutes. If excision of nearby tissues or lymph nodes is required, the time increases to 2-3 hours.
Extirpation on video:
Excision of the parotid gland
It is removed by first making an incision on the cover in the ear fold. If a tumor is present, a superficial parotidectomy is indicated. The facial nerve and its branches are preserved if the formation does not involve them in the lesion and is located higher.
In other cases, when nerve branches are involved in the lesion, extirpation is prescribed, during which the lymphatic mesh is removed and the underlying tissue is excised.
The duration of the operation is approximately an hour. The wound is sutured, and a drainage tube is inserted into the incision to remove exudate.
Sublingual extirpation
In this case, the sublingual gland is removed through the mouth. The duration of the operation is up to 30 minutes. Indications for extirpation are small adenoma or cyst.
If the tumor has reached a significant size, a second access is created through the skin under the chin. In such cases, complete excision of the organ is required.
Preparation and performance of the operation
Surgical intervention associated with removal requires preparatory measures.
To identify concomitant diseases that may become an obstacle to surgical intervention, the following studies are prescribed:
- blood tests;
- X-ray diagnostics
- Ultrasound.
Your doctor may require you to stop taking certain medications 7 days before surgery, such as nonsteroidal anti-inflammatory drugs, blood thinners, and antiplatelet drugs.
Before performing an intervention on a large gland, general anesthesia is used to avoid pain. When removing small ones, local anesthesia is used. The operation is performed on an outpatient basis. After the intervention, you will need to stay in the hospital for another 1-2 days.
On the previous day, it is necessary to finish a large meal and do a cleansing enema. Alcohol and smoking are excluded no later than 2 weeks before surgery. Immediately before the intervention, it is forbidden to drink or eat.
Next, an operation is performed depending on the area of pathological changes and the characteristics of the development of the primary disease.
The price for removing a gland can range from 40 to 95 thousand rubles, depending on the severity of the pathology and the location of the organ.
How the operation to remove an adenoma of the submandibular salivary gland is performed - video:
Surgical technique
Sialectomy is performed after a control x-ray examination in a veterinary clinic. In the image, the doctor can see the location of the stone or the degree of tissue damage during the tumor process. Diagnosis of cystic formations is based on examination of the oral cavity, palpation and puncture of the cyst.
Removal of the salivary gland during obstruction of its ducts is indicated if the stone is difficult to remove. Or in cases where the root cause of stone formation cannot be eliminated.
Tumor growths are removed en bloc to minimize the risk of recurrence of the tumor.
Retention cysts also involve removal of the underlying salivary glands. To eliminate the cyst, marsupialization is recommended. The swelling cavity is dissected, and the walls are sutured to nearby tissues. A closed pathological cavity is turned into an open pocket.