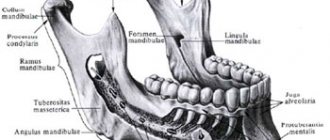
Anatomical structure of the tooth
Anatomy distinguishes three elements of tooth structure:
Tooth root
- This is an invisible “part” that is hidden in the jaw. A tooth can have from one to three roots, depending on its functions. However, there are known cases when one tooth had up to 5 roots. The root is attached to the alveolus (tooth socket), tightly surrounded by connective tissue.
Tooth neck
- This is the transitional part of the tooth from the root to the crown. It is also covered by the mucous membrane of the gums and connected to the bone substance of the alveoli.
Crown of the tooth
– this is the visible part, in fact, what we call a tooth.
The shape of teeth depends on the functions they perform. Nature has provided for all stages of chewing here.
A man takes a bite of food. The front teeth come into play. They feature a thin edge and cut off pieces of food. Such teeth are called incisors. Then the pieces are sent to the pointed outer teeth. The fangs tear them into smaller pieces. Premolars and molars - large lateral teeth - complete the process - chewing food, grinding it, so that the food ground into porridge is sent into the esophagus.
Why do the necks of the teeth become exposed?
Exposure of the neck of the tooth, the causes and treatment of which are closely related, can cause the patient to have:
- Atrophic gingivitis. Inflammation and swelling of the gums occurs, bleeding occurs, as a result of which the volume of tissue decreases and the neck of the teeth is exposed.
- Periodontitis. In the space between the teeth, the accumulation of pathogenic microorganisms, plaque, and the formation of tartar begins. Next, the soft tissue and ligaments that support the tooth are destroyed. There is a gradual resorption of bone tissue and subsidence of the gums, as a result of which the part of the tooth that should be under the gum is exposed.
- Caries of the cervical zone. When a tooth is damaged by caries, bacteria begin to multiply in the upper part of the crown and the gum tissue is destroyed.
- Improper oral hygiene. Carrying out poor hygiene measures or too intense movements with a toothbrush can cause microtrauma to the gums, the proliferation of bacteria, which results in the development of gum disease, and then the neck of the tooth is exposed.
- Anatomical features of the bite. With crowded teeth, short frenulum or small vestibule of the oral cavity.
- Age-related changes in tissue. This occurs mainly in older people.
- Bruxism. Grinding of teeth and clenching them tightly leads to exposure of the cervix.
- Diseases of the gastrointestinal tract. The altered acidity of saliva, which in most cases is present in gastrointestinal diseases, destroys the enamel. In addition, bacteria begin to multiply in the mouth, pathological processes occur in the soft tissues, as a result of which the neck becomes bare.
Considering the reason why the neck of the tooth is exposed, the disease develops at different rates and different consequences arise.
Symptoms
When the dental neck becomes exposed, it is visible to the naked eye. Especially if the problem concerns the front teeth. The hidden part of the tooth differs from the enamel in yellow. In addition to these signs, you can suspect that the cervix is exposed based on the following symptoms:
- Spicy, sour, cold and hot foods cause pain in all teeth at once.
- Brushing your teeth is an unpleasant experience.
- The gums become swollen, swollen, and inflamed.
- When passing along the gingival margin, the presence of unevenness (steps) is felt.
- The fragility of teeth increases.
- The roots are affected by caries.
- Visual elongation of the tooth, as the edge of the gum has shifted. Visually, it seems that the gap between the teeth has increased.
- The inflammatory process causes the appearance of a periodontal pocket in which pus will accumulate.
- The appearance of a putrid odor in their mouth.
- A weakened tooth is not securely fixed in the gum, increasing the risk of tooth loss.
The structure of the periodontium –
As we said above, the periodontium is located between the cementum of the tooth root on one side and the compact lamina of the alveoli on the other side. It consists of loose fibrous connective tissue (FCT), the main component of which is mature type I collagen fibers. Moreover, in people under 25 years of age, in addition to mature collagen, fibers of immature collagen (procollagen) can also be found in the periodontium. Between the bundles of collagen fibers there is an intercellular substance with blood and lymphatic vessels, as well as nerve fibers.
There are no mature elastic fibers in the periodontium, and there are only a small number of immature elastic fibers (oxytalan), which are located along the walls of blood vessels. At the same time, the collagen fibers themselves are rigid and incapable of stretching - so how is the physiological mobility of the tooth formed? The fact is that collagen fibers in the periodontium have a shock-absorbing effect due to their spiral bends. These bends straighten during chewing load on the tooth, and when it stops, they curl again. Thanks to such bends, the tooth has physiological mobility.
Periodontal fibers (histological specimen) –
The cellular composition of the periodontium is represented primarily by fibroblasts, cementoblasts and osteoblasts, which are involved in the construction of collagen, cement and bone tissue, respectively. In addition, Malasse epithelial cells were found in the periodontium, which can be a source of the formation of cysts and tumors. We will talk about the full composition of cellular elements below.
Types of periodontal fibers:
Collagen fibers passing nearby intertwine with each other, forming strong bundles with a diameter of 0.2 mm (such bundles are called periodontal ligaments or ligaments). There are several alternative classifications of periodontal fibers, and below we present two of them. According to the classification of I.P. Gayvoron periodontal fibers can be divided into 3 types (Fig. 2) –
- dental-gingival fibers,
- dentoalveolar fibers,
- interdental fibers.
1) Complex of dental-gingival fibers - bundles of these fibers begin from the cementum of the tooth root in the area of the bottom of the gingival pocket, and then they spread fan-shaped, weaving into the soft tissue of the gums around the neck of the tooth (marginal edge of the gums). This type of fiber ensures a tight fit of the gum to the neck of the tooth. Below you can see that the dentogingival fibers have a variety of directions and form a three-dimensional network in the gum tissue. The structure of these fibers is quite thin and not too powerful.
2) Dento-alveolar fibers (horizontal and oblique) - these fibers begin just below the fibers of the previous group. They are located in the periodontal gap between the cementum of the tooth root on one side and the compact lamina of the alveoli on the other side. Dento-alveolar fibers are usually divided into horizontal and oblique. Horizontal fibers are quite small in number, and they go in a horizontal direction from the surface of the tooth root - to the apices of the interalveolar septa (Fig. 5).
Almost the entire surface of the roots is covered with oblique dento-alveolar fibers, and it is predominantly this type of fiber that holds the tooth in the alveolus and also performs a support-shock-absorbing function. At one end these fibers are attached to the cementum of the root, and at the other to the wall of the alveoli. Due to the oblique direction of the fibers, the tooth is suspended inside the alveolus and, thus, chewing pressure is not directly transmitted from the tooth to the bone tissue of the alveolus. In general, the arrangement of bundles of dento-alveolar fibers in the lateral sections of the periodontal fissure looks like a hammock mesh (Fig. 5-6).
In the middle third of the periodontal fissure (in young people under 25 years of age) there is a dense intermediate plexus of immature collagen fibers - the so-called “Sikcher plexus”. The fibers of this plexus have a very high regenerative potential. They are of great importance for the regeneration of periodontal structures, for example, this can be important when planning orthodontic treatment. But it must be taken into account that the Sickher plexus disappears in people over 25 years of age. A number of researchers have put forward a logical explanation for the need for the presence of immature collagen in the periodontium.
The fact is that part of the periodontal fibers begins to form from the side of the cement of the tooth root, and the other part - from the side of the bone plate of the alveoli. According to a number of authors, periodontal fibers are not a single formation, and when both parts of the fibers reach the middle of the periodontal fissure, they are connected through immature collagen fibers. By the way, this theory is confirmed by the clinical observations of the author of the article, who has repeatedly carried out replantation of teeth completely removed from the socket. At the same time, fragments of periodontal fibers were preserved on the side of the socket and the root of the tooth, thanks to which the periodontium regenerated perfectly in young patients (24stoma.ru).
3) Transseptal (interdental) fibers - these fibers go from the neck of one tooth to the neck of another, and for this purpose the fibers pass over the tops of the interalveolar septa. Those. they form a “ligament” that goes from the cementum of the root of one tooth (on the side of the contact surface) to the cementum of the root on the contact surface of the adjacent tooth. These periodontal fibers perform the function of maintaining the continuity of the dentition, as well as redistributing the chewing load along the dentition.
Alternative classification of periodontal fibers –
There are several alternative classifications of periodontal fibers. These classifications may include the following division of fibers into groups:
- Circular (free) fibers - they start from the neck of the tooth, fan out, ending in the soft tissues of the gingival margin.
- Fibers of the alveolar ridge - they connect the neck of the tooth with the crest of the alveolar bone (in Fig. 4 they are called dentocomb fibers).
- Horizontal fibers are a small group of fibers that are located immediately under the fibers of the alveolar ridge (at the very entrance to the periodontal space). These fibers run horizontally, forming, together with the transseptal fibers, the circular ligament of the tooth.
- Oblique fibers are the most numerous group of fibers that connect the tooth root with the compact lamina of the alveoli (in the previous classification they were called dento-alveolar).
- Apical fibers - they diverge perpendicular to the dento-alveolar fibers from the apices of the roots to the bottom of the alveoli.
- Transseptal fibers - they run horizontally from the neck of one tooth to the neck of another, connecting adjacent teeth to each other.
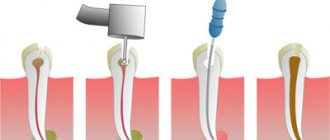
Types and symptoms of apical periodontitis
Depending on how the inflammatory process proceeds, two types of disease are distinguished: acute apical periodontitis and chronic apical periodontitis. The second is always a consequence of the first: if acute inflammation is not cured in time, then it has every chance of becoming chronic.
The symptoms of acute apical periodontitis of pulpal origin are difficult to miss - they can cause the patient many unpleasant moments. The acute period is usually accompanied by the following conditions:
- nagging pain in the area of the affected tooth, which intensifies over time, becomes pulsating, and can radiate to other parts of the face;
- swelling of soft tissues, enlarged lymph nodes;
- rise in temperature;
- headache.
The duration of acute apical periodontitis ranges from 2 days to 2 weeks. In the absence of appropriate treatment, two options are possible: either the disease will progress, involving more and more tissue, or it will enter a chronic stage. The clinic of chronic apical periodontitis looks like this:
- pain in the affected area is mild or absent altogether, and can also occur when pressing or biting;
- slight tissue swelling may be observed;
- Possible bad breath;
- the diseased tooth is sensitive to temperature influences.
The chronic course of the disease may be accompanied by acute periods. With exacerbation of chronic apical periodontitis, the same symptoms are observed as in the acute form.