9 months of bearing a baby is a short and at the same time long period during which a woman can be overcome by various kinds of ailments. The peculiarities of the situation impose serious restrictions on the list of drugs designed to eliminate the health problems that have arisen. Homeopathic medicines belong to a relatively safe category of medicines. A popular medicine in this group, which is often used in the treatment of pregnant women, is Viburkol. In what cases can Viburkol suppositories be prescribed during pregnancy?
37th week of pregnancy for baby
At the 37th week of pregnancy, the baby’s height is approximately 48 cm, and his weight is 2,600 g. Externally, the fetus is almost no different from a newborn; all facial features are developed, and cartilaginous tissue is clearly visible. The accumulation of subcutaneous fat at this stage of pregnancy makes the body contours softer and rounder. The baby’s skin gradually smoothes out, it is no longer as pink as in the previous weeks of intrauterine development, and the integument gradually becomes lighter. The baby's body is still abundantly covered with lubricant, but the amount of vellus hair decreases noticeably, vellus hair remains only on the shoulders and back, and in some babies it disappears almost completely.
This week the accumulation of fatty tissue continues. It reaches a maximum of 15% of the child’s total body weight. It is difficult to overestimate the importance of adipose tissue for newborns; it is this tissue that protects the child from overheating or hypothermia, since the baby’s thermoregulation system after birth is not yet sufficiently formed and continues to develop in the first months of the little person’s life.
At this stage, not only the volume of subcutaneous fat increases, but also the muscles and skeleton intensively develop. The child constantly moves his arms and legs. These unique workouts help increase muscle mass. The baby also makes rhythmic breathing movements that strengthen the intercostal muscles and diaphragm, preparing the respiratory organs for childbirth.
Pregnant woman at 37 weeks
As the due date approaches, pregnant women begin to notice the appearance of their precursors, that is, certain signs and changes that occur under the influence of hormones. A woman’s body is preparing to give birth to a child, progesterone gives way to the dominant role of the birth hormone estrogen, and the pregnant woman’s well-being changes.
From the 37th week, expectant mothers may observe the following changes:
- slight loss of body weight;
- reduction in abdominal volume;
- the appearance of training or “false” contractions and an increase in their intensity;
- discharge of mucus from the cervix.
The nature of the stool changes, it becomes weaker, aching pain in the lower back of varying intensity may appear, and the fundus of the uterus descends. The woman notes some signs on her own, others are observed by the gynecologist during a routine examination.
Precursors do not appear in all women. Some expectant mothers notice only some of the symptoms listed above, while others observe signs of impending labor not two or three weeks before the due date, but just a few hours. Both the appearance of precursors at the 37th week and their absence are normal and depend on the individual characteristics of the woman’s body.
This week, the female body is intensively preparing for the birth of a child. If the fetus is positioned correctly, head down, it gradually lowers, goes to the lower part of the uterus, presses it to the body and bends its limbs, intuitively taking the most comfortable position for passing the birth canal. The consequence of fetal movement is prolapse of the uterine fundus. The abdomen lowers, the pressure on the diaphragm decreases significantly, the pregnant woman can breathe easily, and the shortness of breath that plagued her in the previous weeks disappears. The pressure on the stomach also decreases, heartburn, a feeling of heaviness after eating and other unpleasant sensations disappear. Moving your baby can put pressure on your bowels and bladder. A pregnant woman at this stage often experiences the urge to urinate and may suffer from frequent loose stools. The reason for frequent bowel movements is not only the mechanical effect of the uterus on it, but also an increase in the content of estrogen in the body, hormones that promote the excretion of fluid. At the 37th week, the expectant mother can have bowel movements up to 3-4 times a day and at the same time observe significant dilution of the stool.
Treatment for retrochorial hematoma
It is recommended to treat retrochorial hematoma, mainly because only there it is possible to ensure truly complete physical rest and the absence of any stress. No promises to “lie down all the time” at home can be realized - there will always be a bunch of urgent household chores that you want to do - from cleaning to laundry. In addition, the hospital can provide emergency assistance at any time - intravenous administration of hemostatic agents, for example. If it is not possible to go to a hospital, then you should consider the option of a day visit to the clinic or staying with us for a couple of days.
Bed rest is recommended, and in order to restore the outflow of blood, it is advised to lie down with a cushion, for example made from a rolled blanket, under the pelvic area. To prevent congestion in the intestines, it is recommended to follow a diet: exclude legumes, spicy foods; products that strengthen stool or enhance intestinal motility (chocolate, coarse fiber). The intestines overflowing with gases put pressure on the pregnant uterus and increase the tone of the uterus, which increases the threat of miscarriage and increases the size of the hematoma. Also, to reduce the risk of increased uterine tone, you need to limit the consumption of strong tea and coffee.
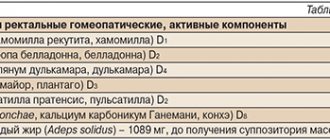
Drug therapy consists of using drugs that improve blood clotting, due to which bleeding stops and the hematoma stops growing (tranexam, dicynon, vikasol). To relieve hypertonicity of the uterus, due to which the hematoma can grow, antispasmodics (no-spa, metacin, suppositories with papaverine) are used. In order to normalize hormonal regulation in the body, metabolic vitamin therapy is used. Progesterone preparations are used. In this case, the scheme and route of administration are selected individually by the doctor; these can be either drugs for intramuscular administration (oil solution of progesterone), or suppositories (Utrozhestan, Iprozhin), tablets (Duphaston) or gel (Crinone). It should be noted that when bloody discharge appears from the genital tract, utrozhestan continues to be administered intravaginally. Its effectiveness is not reduced!
Treatment usually lasts from 2 to 4 weeks, and, if indicated, is repeated at critical times (12–14, 20–24, 28–32, 36–38 weeks). Resorption of the hematoma usually occurs from 2 to 4-5 weeks.
38th week of pregnancy: development of the unborn baby
At the 38th week, the fetus is fully formed, so childbirth at this stage is no longer dangerous for both mother and baby. The weight of the fetus is about 3 kg, but this figure can vary significantly between babies; the weight depends on the individual characteristics of the mother and child, body structure and other factors. The body length of a newborn is approximately 50 cm.
All organs and systems at a period of 38 weeks are characterized by physiological and morphological maturity, they are completely ready for work. At this stage, the baby is preparing for childbirth, making breathing movements and preparing the intercostal muscles for breathing. The lung tissues are washed with amniotic fluid, which helps maintain the required level of surfactant covering the baby's lungs from the inside. All elements of the respiratory system are ready for use. With the first breath after birth, the alveoli begin to transfer oxygen from the air into the blood, gas exchange occurs, and the respiratory and circulatory systems begin to work intensively.
Providing emergency medical care for acute allergic diseases
Ph.D.
A.V. Topolyansky, professor A.L. Vertkin Scientific Center for Children's Health of the Russian Academy of Medical Sciences, Moscow MMA named after I.M. Sechenov MGMSU named after. ON THE. Semashko Station of ambulance and emergency medical care, Moscow National Scientific and Practical Society of Emergency Medical Care, Moscow
P
According to the National Scientific and Practical Society of Emergency Medical Services, over the past 3 years the number of calls for acute allergic diseases in the Russian Federation as a whole has increased by 18%. Moreover, their frequency in different regions ranges from 1 to 5% of all cases of emergency medical team visits.
Main causes and pathogenesis
The pathogenesis of allergic reactions has been studied quite fully today and is described in detail in many domestic and foreign monographs on allergology and clinical immunology. In any case, in the tissue of the shock organ or the “target” organ, which can be the skin, bronchi, gastrointestinal tract, etc., signs of allergic inflammation appear. The central role in the implementation of these immunopathological reactions belongs to class E immunoglobulins
(IgE), the binding of which to the antigen leads to the release of allergy mediators (histamine, serotonin, cytokines, etc.) from mast cells.
Most often, allergic reactions develop when exposed to inhaled allergens in homes, epidermal, pollen, food allergens, medications, parasite antigens, as well as stings and insect bites. Drug allergies most often develop when using analgesics, sulfonamides and antibiotics from the penicillin group, and less often cephalosporins. In addition, the incidence of latex allergy is high.
Clinical picture, classification and diagnostic criteria
From the point of view of providing assistance and assessing the prognosis, acute allergic diseases can be classified as follows (Table 1):
Lungs
– allergic rhinitis (year-round or seasonal), allergic conjunctivitis (year-round or seasonal), urticaria.
Moderate to heavy
– generalized urticaria, angioedema, acute laryngeal stenosis, moderate exacerbation of bronchial asthma, anaphylactic shock.
The greatest concern when providing medical care at the prehospital stage should be caused by prognostically unfavorable cases of development of life-threatening conditions in patients: severe asthma attack (status asthmaticus), anaphylactic shock, Quincke's edema in the larynx, acute laryngeal stenosis.
When analyzing the clinical picture of an allergic reaction, the emergency physician should receive answers to the questions presented in Table 2.
The initial examination should assess for the presence of: stridor, dyspnea, wheezing, dyspnea, or apnea; hypotension or syncope; changes on the skin (urticaria-type rashes, Quincke's edema, hyperemia, itching); gastrointestinal manifestations (nausea, abdominal pain, diarrhea); changes in consciousness. If the patient has stridor, severe shortness of breath, hypotension, arrhythmia, convulsions, loss of consciousness or shock, then this condition is considered life-threatening.
Treatment of acute allergic diseases
In case of acute allergic diseases at the prehospital stage, emergency therapy is based on the following areas:
Stopping further entry of the suspected allergen into the body
. For example, in case of a reaction to a drug administered parenterally or to an insect bite/sting, apply a tourniquet above the injection or sting site for 25 minutes (every 10 minutes, loosen the tourniquet for 1–2 minutes); to the injection or bite site - ice or a heating pad with cold water for 15 minutes; pricking at 5–6 points and infiltrating the injection or bite site with 0.3–0.5 ml of 0.1% epinephrine solution with 4.5 ml of isotonic sodium chloride solution.
Antiallergic therapy (antihistamines or glucocorticosteroids)
.
The administration of antihistamines is indicated for allergic rhinitis, allergic conjunctivitis, and urticaria. Glucocorticoid therapy (GCS) is carried out for anaphylactic shock and angioedema (in the latter case, the drug of choice): prednisolone
(adults - 60-150 mg, children - at the rate of 2 mg per 1 kg of body weight).
For generalized urticaria or when urticaria is combined with Quincke's edema, betamethasone
1-2 ml intramuscularly is highly effective. In case of angioedema, to prevent the effect of histamine on tissues, it is necessary to combine new generation antihistamines (loratadine) with glucocorticoids.
Symptomatic therapy
. With the development of bronchospasm, inhaled administration of b2-agonists and other bronchodilators and anti-inflammatory drugs through a nebulizer is indicated. Correction of arterial hypotension and replenishment of circulating blood volume is carried out by administering saline and colloid solutions (isotonic sodium chloride solution 500–1000 ml, hydroxyethyl starch 500 ml, polyglucin 400 ml). The use of vasopressor amines (dopamine 400 mg per 500 ml of 5% glucose, norepinephrine 0.2 - 2 ml per 500 ml of 5% glucose solution; the dose is titrated until a systolic pressure level of 90 mm Hg is achieved) is possible only after replenishment of the circulating blood volume . For bradycardia, it is possible to administer atropine in a dose of 0.3–0.5 mg subcutaneously (if necessary, the administration is repeated every 10 minutes). In the presence of cyanosis, dyspnea, and dry wheezing, oxygen therapy is also indicated.
Anti-shock measures
(Fig. 1). In case of anaphylactic shock, the patient should be laid down (head lower than legs), head turned to the side (to avoid aspiration of vomit), protract the lower jaw, and remove removable dentures. Epinephrine is administered subcutaneously in a dose of 0.1 - 0.5 ml of a 0.1% solution (drug of choice); if necessary, injections are repeated every 20 minutes for an hour under blood pressure monitoring. In case of unstable hemodynamics with the development of an immediate threat to life, intravenous administration of epinephrine is possible. In this case, 1 ml of 0.1% epinephrine solution is diluted in 100 ml of isotonic sodium chloride solution and administered at an initial rate of 1 mcg/min (1 ml per min). If necessary, the rate can be increased to 2–10 mcg/min. Intravenous administration of epinephrine is carried out under the control of heart rate, respiration, and blood pressure (systolic blood pressure must be maintained at a level of more than 100 mm Hg in adults and > 50 mm Hg in children). Medicines used for allergic diseases of varying severity and their effectiveness are presented in Table 3.
Rice. 1. Treatment algorithm for anaphylactic shock
Clinical pharmacology of drugs used for the treatment of acute allergic diseases.
The method of administration and dosage of antiallergic drugs are presented in Table 4.
Epinephrine
Epinephrine is a direct stimulator of a- and b-adrenergic receptors, which determines all its pharmacodynamic effects. The mechanism of antiallergic action is realized:
The method of administration and dosage of antiallergic drugs are presented in Table 4. Epinephrine is a direct stimulator of - and - adrenergic receptors, which determines all its pharmacodynamic effects. The mechanism of antiallergic action is realized:
• stimulation of a-adrenergic receptors, vasoconstriction of the abdominal organs, skin, mucous membranes, increased blood pressure;
• positive inotropic effect (the strength of heart contractions increases due to stimulation of b1-adrenergic receptors of the heart);
• stimulation of b2-adrenergic receptors of the bronchi (relief of bronchospasm);
• suppression of degranulation of mast cells and basophils (due to stimulation of intracellular cAMP).
When administered parenterally, the drug has a short-term effect (intravenous - 5 minutes, subcutaneously - up to 30 minutes), as it is quickly metabolized in the endings of sympathetic nerves, in the liver and other tissues with the participation of monoamine oxidase (MAO) and catechol-O-methyltransferase (COMT) .
Side effects:
dizziness, tremor, weakness; strong heartbeat, tachycardia, various arrhythmias (including ventricular), the appearance of pain in the heart area; difficulty breathing; increased sweating; excessive increase in blood pressure; urinary retention in men suffering from prostate adenoma; increased blood sugar levels in patients with diabetes. Tissue necrosis has also been described with repeated subcutaneous injection into the same place due to local vasoconstriction.
Contraindications:
arterial hypertension; severe cerebral atherosclerosis or organic brain damage; cardiac ischemia; hyperthyroidism; angle-closure glaucoma; diabetes; prostatic hypertrophy; pregnancy. However, even with these diseases, it is possible to prescribe epinephrine for anaphylactic shock for health reasons and under strict medical supervision.
Glucocorticosteroids
The mechanism of the antiallergic action of glucocorticoids is based on the following effects:
• immunosuppressive property (suppression of growth and differentiation of immune cells - lymphocytes, plasma cells, reduction in antibody production);
• prevention of degranulation of mast cells and the release of allergy mediators from them;
• decreased vascular permeability, increased blood pressure, improved bronchial obstruction.
Prednisolone is used for parenteral administration during emergency treatment at the prehospital stage.
.
For the treatment of bronchial asthma, allergic rhinitis, and allergic conjunctivitis, topical forms of glucocorticosteroids ( fluticasone, budesonide
) have been developed. Side effects of systemic corticosteroids: arterial hypertension, agitation, arrhythmia, ulcerative bleeding. Side effects of topical corticosteroids: hoarseness, disturbance of microflora with further development of mucosal candidiasis, when using high doses - skin atrophy, gynecomastia, weight gain, etc. Contraindications: peptic ulcer of the stomach and duodenum, severe arterial hypertension, renal failure , history of hypersensitivity to glucocorticoids.
Betamethasone
– glucocorticosteroid drug, consists of 2 mg of disodium phosphate and 5 mg of betamethasone dipropionate. Betamethasone disodium phosphate provides rapid onset of effect. Prolonged action is ensured by betamethasone dipropionate. The drug has immunosuppressive, antiallergic, desensitizing and antishock effects. Betamethasone is biotransformed in the liver. The dose of the drug depends on the severity of the disease and the clinical picture of the course. It is used for the treatment of acute allergic diseases in the form of intramuscular injections of 1–2 ml. With a single administration, no significant side effects were noted.
Antihistamines (H1-histamine receptor blockers)
There are several classifications of antihistamines. According to one of them, drugs of the first, second and third generation are distinguished (at the same time, the question of whether different drugs belong to the 2nd or 3rd generation is still debated). Another classification, more popular among clinicians, distinguishes between classic antihistamines, for example, chloropyramine, and new generation drugs (acrivastine, fexofenadine, loratadine, etc.)
It should be noted that classical antihistamines, in contrast to new generation drugs, are characterized by a short duration of action with a relatively rapid onset of clinical effect. Many of them are available in parenteral forms. All this determines the widespread use of classical antihistamines at the present time.
Chloropyramine
– one of the widely used classical antihistamines. It has significant antihistamine activity, peripheral anticholinergic and moderate antispasmodic effects. When taken orally, it is quickly and completely absorbed from the gastrointestinal tract. The maximum concentration in the blood is achieved within the first 2 hours, the therapeutic level of concentration remains for 4–6 hours. Effective in most cases for the treatment of seasonal and year-round allergic rhinitis and conjunctivitis, urticaria, atopic dermatitis, eczema; in parenteral form – for the treatment of acute allergic diseases requiring emergency care. Has a wide range of therapeutic doses used. It does not accumulate in the blood serum, therefore it does not cause an overdose with long-term use. The drug is characterized by a rapid onset of effect and a short duration (including side effects). Can be combined with other H1 blockers to increase the duration of the antiallergic effect. Available in tablets and ampoules for intramuscular and intravenous administration.
New generation antihistamines are devoid of cardiotoxic effects, have a competitive effect on histamine, are not metabolized by the liver (for example, the pharmacokinetics of acrivastine does not change even in patients with impaired liver and kidney function) and do not cause tachyphylaxis.
Akrivastine
– a drug with high antihistamine activity with minimally expressed sedative and anticholinergic effects. A feature of its pharmacokinetics is a low level of metabolism and the absence of accumulation and addiction. Acrivastine is preferred in cases where there is no need for continuous antiallergic treatment. The gelatin capsule is quickly absorbed in the stomach, providing a rapid onset of effect. The drug has a short period of action, which allows the use of a flexible dosage regimen. No cardiotoxic effect. Selectively influencing H1 receptors, it does not irritate the gastric mucosa. There is no effect on H2 receptors.
Loratadine
– a new generation antihistamine over-the-counter.
Indications for use: allergic rhinitis (seasonal and year-round), allergic conjunctivitis, urticaria, generalized urticaria, Quincke's edema, allergic reactions to insect bites, itchy dermatoses (contact allergic dermatitis, chronic eczema).
The drug has no side effects such as drowsiness, dry mouth, headache, dizziness.
Bronchospasmolytics: short-acting b2-agonists and anticholinergics
Berodual is a combined bronchospasmolytic drug containing two bronchodilators: fenoterol (b2-agonist) and ipratropium bromide (anticholinergic). One dose of Berodual contains 0.05 mg of fenoterol and 0.02 mg of ipratropium bromide.
Method of use: using a nebulizer to relieve an attack of suffocation, inhale 10–20 drops of Berodual in 1–4 ml of physiological solution for 5–10 minutes. If there is no improvement, repeat inhalation after 20 minutes.
Salbutamol
– selective agonist of b2- adrenergic receptors. The bronchodilator effect of salbutamol occurs within 4–5 minutes. The effect of the drug gradually increases to its maximum at 40–60 minutes. The half-life is 3–4 hours, duration of action is 4–5 hours.
Directions for use: using a nebulizer; nebulas of 2.5 ml containing 2.5 mg of salbutamol in saline solution. 1–2 nebulas (2.5–5.0 mg) are prescribed for inhalation, undiluted. If there is no improvement, repeat inhalations of 2.5 mg every 20 minutes. In one hour.
Typical errors in the use of drugs in the treatment of acute allergic diseases at the prehospital stage
• Isolated administration of H1-histamine blockers for severe allergic reactions, as well as for broncho-obstructive syndrome, has no independent significance and at the prehospital stage only leads to unjustified loss of time.
• The use of diprazine is also dangerous because it worsens hypotension.
• Late administration of GCS; unreasonable use of small doses of corticosteroids.
• Use of certain drugs not indicated for the treatment of allergic diseases (calcium gluconate, calcium chloride, etc.).
• The presence of unidirectional drugs in the equipment list of ambulance teams is not economically justified.
• Non-use of topical corticosteroids and b2-agonists for allergic laryngeal stenosis and bronchospasm.
Patients with severe allergic diseases must be hospitalized. For mild allergic diseases, the issue of hospitalization is decided on an individual basis in each case.
APPENDIX
Allergic stenosis of the upper respiratory tract in children
Main causes and pathogenesis
Upper respiratory tract obstruction syndrome (croup, acute stenosing laryngotracheitis) in children is one of the common reasons for seeking emergency care. There are acute allergic stenosis of the larynx and stenosis developing against the background of ARVI.
The main reason for the development of allergic stenosis of the upper respiratory tract with a predominant localization of the process in the larynx is the body’s sensitization to food and drug allergens, as well as to allergens of house dust mites (Dermatophagoides pteronyssinus and Dermatophagoides farinae), animals, etc.
Acute allergic stenosis of the upper respiratory tract
more often observed in children with a hereditary predisposition to allergies. The development of croup is often preceded by the appearance of symptoms of skin and respiratory allergies. The occurrence of allergic stenosis of the larynx is also favored by such anatomical features of this organ in children as the softness of the cartilaginous skeleton, a short and narrow vestibule and a high-lying larynx, the presence of a delicate mucous membrane rich in cellular elements and a loose submucosal layer with an abundant vascular network and a large number of mast cells. . These structural features of the mucous and submucous membranes are especially characteristic of the area of the larynx surrounded by dense cricoid cartilage. This area is projected onto the subglottic space, where the most pronounced edema develops in children. Croup most often develops in children aged 6 months to 3 years, and boys suffer from it 3–4 times more often than girls.
The pathogenetic basis of allergic stenosis of the upper respiratory tract is IgE-mediated allergic reactions, causing the development of inflammation in the laryngeal mucosa in the form of edema, hypersecretion of mucus, spasm of the smooth muscles of the upper respiratory tract; In some patients, bronchospasm also occurs. The development of acute stenosing laryngotracheitis may also be associated with exposure to a viral infection, chemical pollutants, and changes in the weather situation.
Clinical picture, classification and diagnostic criteria
Acute laryngeal stenosis causes the development of respiratory failure and disruption of the child’s general condition. There are three degrees of stenosis
depending on the severity of the narrowing of the larynx:
I degree
laryngeal stenosis – compensated stenosis;
II degree
– subcompensated stenosis;
III degree
– decompensated stenosis (Table 5).
Children with allergic laryngeal stenosis are usually found to have heredity burdened by allergic reactions and diseases; they often also have manifestations of atopic dermatitis, food and drug allergies.
This variant of croup is characterized by the sudden development of stenosis “against the background of complete health,” in the absence of catarrhal symptoms, normal body temperature, as well as relatively rapid relief of symptoms of the disease when adequate therapy is prescribed. In a number of children, simultaneously with manifestations of allergic laryngeal stenosis, broncho-obstructive syndrome develops. Acute laryngeal stenosis, developing against the background of an acute respiratory infection, is characterized by a more gradual onset of the disease, the occurrence of stenosis against the background of catarrhal phenomena in the upper respiratory tract, an increase in temperature, the development of symptoms of intoxication, and inflammatory changes in a general blood test.
Laryngeal stenosis must be differentiated from laryngeal diphtheria, foreign body in the respiratory tract, obstructive bronchitis, retropharyngeal abscess, bronchial asthma, whooping cough, pneumonia with manifestations of respiratory failure.
Treatment of acute laryngeal stenosis
Children with acute laryngeal stenosis are subject to mandatory hospitalization. Therapy carried out for acute laryngeal stenosis should be pathogenetic and aimed at restoring air patency of the upper respiratory tract. Treatment is carried out taking into account the severity of laryngeal stenosis, begins with emergency medical services teams on call, and continues along the way to the hospital. The time required to provide prehospital care to a patient should not exceed 60 minutes.
For the treatment of acute laryngeal stenosis in the compensated stage (I degree) at the prehospital stage, inhalations of glucocorticosteroids are used (budesonide through a nebulizer at a dose of 0.25 mg; if nebulizers are ineffective or unavailable, antihistamines are used: intramuscularly (chloropyramine, 2% solution, 0.1 ml in the first year of life) or orally (for children over 12 years old - acrivastine (7 mg, capsule) or loratadine 10 mg (1 tablet or 2 teaspoons of syrup).
Treatment of acute laryngeal stenosis in the stage of incomplete compensation (II degree) begins with inhalation of glucocorticosteroids through a nebulizer at a dose of 0.5 mg. If ineffective, repeat budesonide inhalations in the same dose through a nebulizer with an interval of 20 minutes (maximum 3 times).
In the absence of nebulizers, antihistamines (chloropyramine intramuscularly) and systemic glucocorticosteroids (prednisolone at a rate of 2 mg/kg) are used. If the effect is insufficient, subcutaneous administration of a 0.1% epinephrine solution at the rate of 0.01 mg/kg body weight is additionally prescribed.
III degree laryngeal stenosis occurs with manifestations of respiratory and cardiovascular failure, metabolic disorders, and signs of toxicosis, which necessitates immediate hospitalization. At the prehospital stage, treatment of grade III laryngeal stenosis also begins with inhalation of glucocorticosteroids through a nebulizer at a dose of 1 mg.
If broncho-obstructive syndrome occurs, treatment is carried out with solutions of short-acting b2-agonists (berodual 10-20 drops for children under 6 years old or salbutamol - 1/2-1 nebul for children over 6 years old) through a nebulizer.
Pregnant woman
The body of a pregnant woman continues to actively prepare for the birth of a baby, the content of estrogen rapidly increases, and the level of progesterone decreases significantly. Changes in hormonal levels help soften the tissues of the birth canal and cervix. Throughout pregnancy, the lumen of the cervical canal is closed by a plug of thick mucus, which protects the baby from infection, and the uterine cavity protects against the penetration of microorganisms hazardous to health. In the last weeks of pregnancy, the consistency of the mucus changes, it becomes more liquid and begins to gradually flow out. In some women, the mucus disappears gradually, while in other women in labor it comes off simultaneously. The discharge resembles colorless egg white in its consistency and appearance. Sometimes the mucus is pinkish, brown or yellow. The removal of the plug is painless; the woman may experience a slight feeling of discomfort in the lower abdomen. The removal of the plug may be signaled by more abundant vaginal discharge than during the entire pregnancy.
A woman should carefully monitor the color and volume of discharge, since too much colorless discharge may indicate not only the passage of the plug, but also be one of the symptoms of leakage of amniotic fluid. Indicator pads and amniotests or test strips will help determine the cause of the discharge. The pads are sold in many pharmacies and can be easily used at home. If leakage of amniotic fluid is confirmed, you should immediately consult a doctor.
After the mucus plug comes off, you should avoid visiting the pool and swimming in open water, as the risk of infection for the child increases significantly. It is also necessary to exclude sexual contact.
Can pregnant women get vaccinated?
Considering the fact that COVID during pregnancy is especially severe in patients at risk, timely vaccination is recommended for this category. Vaccination is allowed from 22 weeks; the recommended vaccine is Sputnik V.
Experimental clinical studies on animals did not reveal a negative effect of the vaccine on the body of the female and her offspring. Also in world medicine there is data on the impact of anti-Covid immune drugs on the body of pregnant women, who at the time of vaccination were not aware of their “interesting situation.” No negative consequences were registered.
Thus, vaccination during pregnancy is carried out when the expected benefits outweigh the possible risks.
39th week of pregnancy: what happens to the fetus?
At the 39th week, the child’s weight reaches 3,100-3,500 g, and his height is 50-52 cm. Height and weight indicators are very relative and can differ significantly. The baby is rapidly preparing for the most important test in his life - birth, which requires endurance and significant effort. During this period of pregnancy, the size and weight of the child’s adrenal glands, that is, the glands of the endocrine system, which are responsible for the human body’s response to stress factors, increase. It is the hormones adrenaline and norepinephrine produced by the adrenal glands that help the child adapt as quickly as possible to new temperature conditions, tactile, sound and light impulses.
All the baby's senses are developed at 39 weeks. Within a few moments after birth, the baby can focus his gaze, he reacts to bright light and moving objects, many scientists claim that newborns distinguish colors and see the faces of parents and doctors. In the last weeks of intrauterine life, the baby's hearing is also fully developed; after birth, he reacts to loud sounds and noise. A newborn baby can identify the basic shades of taste, recognize sour, bitter, sweet and salty.
In the womb, the baby is in an aquatic environment that minimizes contact. Immediately after birth, the baby experiences many tactile sensations; unlike intrauterine life, he feels the touch of his mother’s hands and diapers, towels, dressings and other materials. Babies especially like the touch of skin to skin, so in a modern maternity hospital, newborns are always placed on their mother’s stomach even before the umbilical cord is cut. The child adapts more easily to the new environment and feels protected. Placing the baby out has not only a psychological aspect, since it promotes the colonization of microorganisms from the mother’s skin onto the skin and mucous membranes of the baby, and increases his immunity.
What can cause diarrhea during pregnancy?
Diarrhea in late pregnancy can cause premature labor
Statistics give the following figures: each person experiences diarrhea on average 4-5 times a year. Common causes are viral infections and poor diet. In pregnant women, diarrhea can also be caused by hormonal changes. Moreover, “hormones play” in almost every expectant mother.
Diarrhea comes in different forms and varying severity:
- acute diarrhea lasts a maximum of several days and occurs as a result of viruses or pathogens entering the body (food poisoning);
- diarrhea that does not go away, lasts more than two weeks and does not respond to standard treatment;
- Chronic diarrhea is associated with some serious illness and can last more than a month.
There can be several causes of diarrhea during pregnancy: viruses or other microorganisms in foods, side effects of drugs, parasites and diseases of the digestive tract, consumption of foods that are poorly absorbed by the body.
During pregnancy, the body of the expectant mother is exposed to even minor influences from the external environment, because the immune system is weakened and lowered, and all the body’s forces are aimed at preserving and proper development of the fetus.
Therefore, even the simplest factors can cause diarrhea. For example, regular exercises for pregnant women can cause increased gastric motility, resulting in diarrhea.
Prescribed vitamins and vitamin complexes can also cause stomach irritation. Vitamins, by the way, can cause diarrhea in the later stages, even if they were absorbed completely without problems in the first trimesters. Even a proper and balanced diet can cause diarrhea in pregnant women, if before the “interesting situation” the woman ate completely differently. And hormonal levels can complement the overall picture and also become the cause of the disorder.
It would not be superfluous to remind you about the nervous tension of pregnant women: worries, constant stress caused by fear of future birth and the unknown can also cause diarrhea. This condition can also be caused by toxicosis, which is observed in almost every second expectant mother. This can be explained quite simply: toxicosis, in essence, is intoxication of the body. And, as you know, it is often accompanied by diarrhea.
It is worth remembering that diarrhea can have a different character and be observed at different stages of pregnancy. For example, sometimes before childbirth there is a natural cleansing of the body. In this case, you shouldn’t be nervous, you just need to prepare for the trip to the maternity hospital.
Pregnant woman
In the last weeks of pregnancy, the expectant mother strives to prepare her apartment or house as much as possible for the arrival of a new family member. Scientists call this sign of impending birth nesting syndrome. Many women observe signs of the syndrome from the thirtieth week of pregnancy, but at the 39-40th week nesting reaches its maximum point. Pregnant women strive to do general cleaning and repairs, re-stick wallpaper and purchase many new things that, in their opinion, are simply necessary in the house. After giving birth, many purchases cause confusion. The reason for this behavior is an increase in the level of adrenaline and norepinephrine in the body. These hormones are produced by the adrenal glands; they are necessary not only for the woman, but also for the baby to prepare for the upcoming birth.
Is coronavirus dangerous for pregnant women?
Pregnancy during the coronavirus period is especially dangerous if a woman is at risk. In this case, the likelihood of a more severe course of infection compared to the population is increased due to existing immune disorders and concomitant diseases.
Although the infection is new and much is still being studied, risk factors have been identified. These include:
- anamnestic indications of blood clots in arteries and veins before pregnancy;
- an established diagnosis of antiphospholipid syndrome - a condition in which antibodies to the cell membrane are formed in the body;
- inherited forms of thrombophilic disorders - increased blood clotting caused by genetic characteristics;
- confirmed autoimmune diseases, in which the immune system “works” against the cells of its body;
- diabetes mellitus of any type;
- obesity;
- metabolic syndrome is a pathological complex that includes impaired glucose tolerance, excess weight and a number of endocrine disorders;
- lung diseases characterized by a chronic course (bronchial asthma, chronic bronchitis, etc.);
- pregnancy resulting from the use of assisted reproduction methods;
- oncological processes in the body.
However, the presence of risk factors alone does not mean that in 100% of cases COVID during pregnancy will be severe. Coronavirus during pregnancy can go unnoticed (asymptomatic). Only positive results of an antibody test will help determine that a pregnant woman has had a new coronavirus infection.
40th week of pregnancy: how is the baby developing?
40 weeks – full-term pregnancy. The weight of a child born at this period ranges from 2,600 g to 4,400 g, and his body length is 48-53 cm. These indicators are very arbitrary, since at 40 weeks miniature babies weighing 2,600 g and real heroes are born, whose body weight approaches 5,000 g. The body length of newborns can also vary from 45 to 55 cm.
Most women give birth at 40 weeks. At this stage, the baby is completely ready for birth; it meets all the parameters of a full-term baby. Before birth, the baby presses its arms and legs closely to the body, bends its head as much as possible and presses against the exit of the uterus. This position makes it possible to pass the birth canal with the narrowest part of the skull. During labor, with each contraction, the child gradually moves downward; he does not move in a straight line, but makes helical-translational movements, as if screwing into the mother’s birth canal. As the newborn moves forward and his head descends completely, the cervix opens completely. This is followed by pushing, that is, contractions of the uterus that move the baby along the birth canal. The baby's head gradually appears, followed by his body. Childbirth is a complex mechanism that is aimed not only at the safe passage of the birth canal by the child, protecting him from accidental injuries due to increased pressure, but also at preventing ruptures of the woman’s soft tissues.
Pregnant woman
The long wait to meet your unborn child is coming to an end; the 40th week of pregnancy is the last for most women. Every day the expectant mother’s anxiety increases, and the long wait affects her mood and well-being. Women strive to give birth to a child as quickly as possible, so that pregnancy and painful contractions become a thing of the past. Every pregnant woman dreams of meeting her baby, wants to hold him to her breast and stroke his tender head.
Many women, especially first-time mothers, worry that labor will begin unnoticed, but such cases are extremely rare. A woman feels the onset of labor, feels regular contractions that repeat at certain intervals and gradually increase, the time interval between them shortens.
Contractions may be preceded by prenatal rupture of amniotic fluid, which is observed in a certain percentage of women in labor. After the water breaks, contractions may be quite weak or completely absent. Regardless of the intensity of contractions, the release of water is one of the signs of the onset of labor and requires immediate contact with specialists and the woman’s hospitalization in a maternity hospital or hospital, since when the water breaks, the integrity of the bladder is disrupted and the risk of microorganisms dangerous to the baby’s health entering the uterine cavity increases. It is important that after the water breaks, the baby is born within a maximum of 10-12 hours.
A pregnant woman must properly tune in to childbirth, concentrate on the desired result and believe in her own strength, and complete the task intended for her by nature. The right psychological attitude and theoretical knowledge will help a woman become a mother, successfully go through all stages of childbirth and hold the long-awaited child to her heart.
Viburkol during pregnancy - reviews on the use of the drug
Viburkol rectal suppositories are often prescribed to pregnant women, which is why there are a lot of reviews about this medicine. Most of them are positive, although some women did not notice the effect of therapy.
- “I used suppositories almost my entire last pregnancy. They helped very well. Now I'm in position again. My back and stomach started to hurt a lot. I bought Viburkol as prescribed by the doctor. Within 10 minutes after placing the candle I felt relief.”
- “In the second trimester, my health worsened, and the tests were not very good. My back and stomach hurt constantly. The doctor prescribed Viburkol. The candles worked, but not for long. I consider the effectiveness of the drug to be weak given its high price.”
- “The drug is good. The high cost of the drug is fully justified by its effectiveness. Prescribed in the first trimester due to strong tone. The treatment was complex. In addition to Viburkol, Papaverine, MagneB6, Iodofol and Pregnacare vitamins were also prescribed. I can’t say what exactly helped.”
- “I’m dissatisfied with the drug. Prescribed for tone. I didn’t feel the effect, and itching in the anus also appeared.”
- “Prescribed for 6 weeks for abdominal pain. After placing the candle, the discomfort went away.”
Viburkol suppositories quite often become the drug of choice for gynecologists for a wide variety of health problems. And although the drug has a fairly mild effect and is safe for the mother and her baby, it is still not worth abusing the drug.