What is mandibular anesthesia
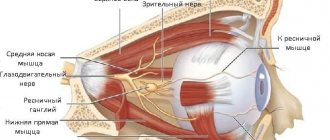
In pediatric dentistry, when treating primary teeth, they most often resort to mandibular anesthesia - anesthesia of the lower alveolar and lingual nerves. The inferior alveolar nerve arises from the mandibular nerve, passes through the mandibular foramen into the canal and branches to each tooth.
The action of the anesthetic solution is directed to the mandibular opening. Until the age of six, it is at the same level as the chewing surface of the primary molars, and then rises by 6 mm at the age of 9 and another 3 mm at the age of 12. Therefore, such exposure is not advisable until the age of six.
Since the inferior alveolar nerve is covered by a bony visor, it can only be reached in the groove of the mandibular nerve. The solution falls down under the influence of gravity. Before manipulation, it is recommended to palpate the edges of the mandibular ramus in order to determine the target point as accurately as possible. The needle is placed slightly above the mandibular foramen.
Anesthesia of the inferior alveolar nerve.
There are three levels of inferior alveolar nerve block. The lower block is standard mandibular anesthesia using the palpation method, the middle block is torsal anesthesia, and the upper block is Go-Gates anesthesia. These three methods of blocking the inferior alveolar nerve are used in different clinical cases. If mandibular anesthesia is ineffective, in order not to create an anesthetic depot in the same area, it is recommended to repeat higher methods of blocking the inferior alveolar nerve: torus anesthesia or Go-Gates anesthesia. If the patient has a history of unsatisfactory results of mandibular anesthesia, it is also recommended to use high blockade methods. On a toothless jaw, it is easier to perform torus anesthesia or Go-Gates anesthesia. When performing surgical interventions on lower molars, in the case of a local infectious process, it is better to use anesthesia that provides simultaneous blockade of the buccal nerve. In many cases, the choice of method for blocking the inferior alveolar nerve is a matter of the doctor’s habit or a feature of the school where his training was originally carried out.
a) Levels of mandibular nerve block; b) The place where the needle is inserted during local anesthesia.
Mandibular anesthesia by palpation.
Before administering anesthesia, the main bony landmarks of the mandibular ramus should be identified by palpation. These include the anterior edge of the jaw ramus and the temporal ridge, located somewhat inward.
Bone landmarks for mandibular anesthesia by palpation.
The needle is inserted medially from the temporal ridge, 1 cm above the occlusal surface of the lower molars. The syringe is located in the opposite corner of the mouth. The needle is advanced until it contacts the bone tissue, a depot of 0.3 ml of anesthetic is created, then the syringe is moved towards the opposite corner of the mouth and the needle is advanced backwards and outwards by 2 cm. An aspiration test is performed. An anesthetic depot of 1 ml is created. Among the positive aspects of this type of anesthesia, it should be noted that it is relatively easy to perform, because By palpation it is easy to determine the main bony landmarks. However, mandibular anesthesia is ineffective in 15 - 20% of cases. Mandibular anesthesia over the lower block does not provide anesthesia for the buccal nerve, so it is blocked separately by infiltrating a specific tooth. Due to the high density of large vessels in the distal part of the pterygomaxillary space, the frequency of positive aspiration tests is 12 - 15%. What are the reasons for the ineffectiveness of mandibular anesthesia? 1. Firstly, bony protrusions medially from the internal oblique line (temporal ridge) interfere with the reversal of the needle. 2. Secondly, anatomically, the mandibular foramen in some cases may be located slightly higher than 2 cm from the occlusal surface of the lower molars. In this case, mandibular anesthesia will be ineffective. Also, on a toothless jaw, due to the absence of lower molars as the main landmarks for the height of needle insertion, anesthesia will be difficult. H. In some cases, the innervation of the lower molars is carried out due to the additional branches of the maxillary-hyoid nerve (n. myelohyoideus). Mandibular anesthesia does not provide blockade of this nerve.
Torusal anesthesia.
The reference point for torsal anesthesia is the pterygomaxillary fold, which is formed by the anterior edge of the medial pterygoid muscle. The syringe is located in the opposite corner of the mouth. The needle is inserted 0.5 cm below the occlusal surface of the upper molars, outward from the pterygomaxillary fold. The needle is advanced anteriorly and outward until it contacts the bone tissue, and an aspiration test is performed. An anesthetic depot of 1.5 ml is created. This type of anesthesia provides anesthesia to the buccal, lingual and inferior alveolar nerves.
Anesthesia according to Go-Gates.
The purpose of anesthesia is to create an anesthetic depot in the area of the neck of the condylar process of the mandibular ramus. The main anatomical landmark during its implementation is the retromolar depression of the upper jaw, which is easily visible in normal and edentulous conditions. With the patient's mouth open as much as possible, the syringe is located in the opposite corner of the mouth, and the needle is inserted into the retromolar depression. The needle is advanced upward, posteriorly and outward, until it contacts the bone tissue of the neck of the condylar process. An anesthetic depot of 1.5 ml is created. An additional guideline for advancing the needle is a finger placed in the external auditory canal. That. the needle is advanced towards the finger. The patient is asked to make 10 open-close mouth movements. This type of pain relief is effective in 98% of cases. The rate of positive aspiration tests is less than 2%. Due to the fact that the soft tissues in the area of the neck of the condylar process are poorly vascularized, the rate of resorptive effect of the local anesthetic will be lower. It follows from this that the duration of anesthesia according to Go-Gates is much longer than with mandibular anesthesia. However, this method of anesthesia is difficult to perform due to the lack of clear guidelines.
Technique of mandibular anesthesia
In pediatric dentistry, this type of anesthesia is performed intraorally. There are various methods, but this one has proven to be the best.
- The dentist determines the point at the intersection of the two lines. The horizontal line is a line running along the chewing surface of the lower molars or 3-5 mm above. The vertical line follows the direction of the pterygomaxillary fold.
- The injection is made at the intersection of these lines.
- After the injection, the needle is gradually advanced, releasing the solution, along the bone by 1.1-1.2 cm. During this period, up to 1 ml of medication must be injected.
- The correct position is this: the bevel of the needle is directed towards the bone, the syringe is deflected in the opposite direction.
- After the injection, the soft tissue in the injection area is pressed against the bone for 1-2 minutes.
Tuberal anesthesia technique
The mouth is half-open, the instrument moves the soft tissues of the cheek outward. The needle is placed at an angle of 45° to the crest of the alveolar process, with a bevel towards the bone tissue. The injection point is in the transitional fold of the mucous membrane at the level of the second molar or between the second and third molar. The needle is advanced up, back and inward to a depth of 2.5 cm, moving the syringe outward so that the needle is always located as close to the bone as possible. Which to a certain extent prevents damage to the arteries, veins of the pterygoid venous plexus and the occurrence of hemorrhage into the surrounding tissues. Up to 2 ml of local anesthetic is injected. In the absence of molars in the upper jaw, the needle is inserted behind the zygomaticalveolar ridge, which corresponds to the middle of the crown of the missing second molar. Anesthesia zone Anesthesia of the upper molars; the periosteum of the alveolar process and the mucous membrane covering it in the area of these teeth on the vestibular side; mucous membrane and bone tissue of the posterior wall of the maxillary sinus. The posterior border of the anesthesia zone is constant. The anterior border can run along the middle of the crown of the first large molar or reach the middle of the first small molar and the corresponding section of the gingival mucosa from the vestibule of the oral cavity. Complications Damage to blood vessels in the area of the tubercle of the upper jaw with the formation of a hematoma; intravascular administration of a local anesthetic in combination with the vasoconstrictor adrenaline can lead to disturbances in the functioning of the cardiovascular and respiratory systems.
What happens after the introduction of conduction anesthesia?
2-3 minutes after the administration of the anesthetic, the patient may feel numbness, tingling and other unpleasant sensations in the lower lip and tongue. The closer the solution was injected to the inferior alveolar nerve, the faster the reaction will occur.
First, pain relief is noticeable at the end of the tongue, then spreads to the lower lip and the corner of the mouth. As soon as the patient’s entire tongue and lower lip are completely numb, this indicates that the anesthesia has taken effect and therapeutic manipulations can begin.
Palpation introduction
Before insertion, the injection site is palpated, which makes it possible to determine the location of the opening of the lower jaw. This is the area where the mandibular nerve exits.
The effect occurs after 10-15 minutes and lasts for 2-3 hours.
After administration, the patient feels numbness, coldness and tingling in the half into which the drug was injected.
Advantages and disadvantages
The advantages include:
- reducing the risk of complications by obtaining anatomical landmarks using the palpation method;
- elimination of sensitivity occurs even in complex clinical cases;
- long-lasting action of the anesthetic;
- complete blocking of half the jaw, which allows you to treat several areas during one appointment.
Disadvantages of the tactile method:
- increased morbidity if the technique is not followed;
- a feeling of discomfort for the patient due to complete numbness of the anesthetized half of the jaw;
- the likelihood of biting the mucous membranes until the effect of the substance stops.
Apodactyl insertion
To implement this method, it is necessary to accurately take into account anatomical features. The localization of the pterygoid fold of the movable jaw, passing behind the molars, serves as a guide to clearly determine the location of the needle entry.
The duration of anesthesia is exactly the same as with the tactile method.
Procedure:
- Injection is administered at the medial end of the fold at the point where the upper and middle thirds border.
- The direction of the needle is perpendicular to the bone.
- The cylinder of the injection mechanism is localized on the opposite side of the premolars.
- The distance the needle advances to the bone is one and a half to two centimeters. This is where the first dose of pain medication is administered.
- Next, the syringe is transferred to the incisors, and the needle is advanced another two centimeters.
- Carrying out an aspiration test. If the test result is negative, the remaining anesthetic is administered.
The area of sensitivity blocking and complications are the same as with the tactile method.
Advantages and disadvantages of the apodactyl method
The pros and cons of the considered method are practically no different from the previous one. The difference lies in the increased likelihood of complications, which is associated with a discrepancy between the exit site of the nerve ending and the anatomical structure of the pterygoid fold of the mandible.
There is another variation of performing apodoctylic mandibular anesthesia (using the Verlotsky technique). The procedure is carried out by analogy with the classical method, with the exception of the injection site. Introduction according to Verlotsky involves inserting the needle centrally between the molars of the upper and lower jaw.
Relevance
Most dental interventions are performed under local anesthesia, the effectiveness of which depends on the correct anesthesia technique [3, 4, 9]. Among the variety of different intraoral methods of anesthesia of the inferior alveolar nerve (mandibular anesthesia), there is no universal method that would be based on topographic-anatomical data. Doctors most often use the pterygomandibular fold as a reference point for mandibular anesthesia. However, when a needle is inserted medial to the pterygomandibular fold, anesthesia may spread to the tissues of the oropharynx and damage to the internal pterygoid muscle with subsequent development of contracture of the mandible [5-8]. The danger of this complication increases when the needle is inserted into a muscle tendon (usually the temporal muscle). When a needle is inserted into the pterygomandibular fold or into its lateral edge, vascular damage and hemorrhage may occur, sometimes the formation of a hematoma, the entry of anesthetic into the bloodstream, the appearance of ischemic zones on the skin of the lower lip, chin, and even a needle fracture. The prevalence of post-injection neurological disorders after mandibular anesthesia is 0.01%. Most often, paresthesia of the lingual nerve is observed [1, 2, 10, 11]. The search for new methods of effective and safe anesthesia remains a pressing problem in dentistry.
The purpose of the study is to increase the effectiveness of anesthesia in the lower jaw teeth and reduce the likelihood of complications using a universal method of local anesthesia based on topographic and anatomical studies.