Local swelling of the root zone, compactions of various sizes, throbbing pain, sensitivity to temperature when eating, enlarged lymph nodes may indicate an acute inflammatory process of infectious etiology. In dentistry, there are several types of diseases, among them periapical abscess. It can be caused by advanced caries, chipping of an element of the dental system, overheating of the pulp due to tooth preparation and various pathologies. This can also happen due to poor-quality root canal treatment.
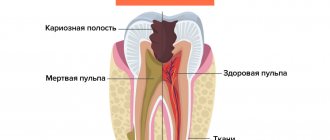
A periapical tooth abscess is an accumulation of pus between the molar and the gums. Purulent exudate can accumulate both in the inner and outer surfaces of the alveolar process of the lower or upper jaw. It most often begins in a tooth with a non-viable pulp, when the nerve dies, causing infection and progressive inflammation. The infection may gradually spread to surrounding tissue. Clinical symptoms are in many ways similar to acute periodontitis. The patient experiences increased sensitivity, acute pain, the mucous membrane may have swelling, there is active hyperemia, and overflow of blood in the vessels of the circulatory system.
Symptoms
- Intense dull throbbing pain.
- Discomfort when chewing food.
- Swelling in this area.
- Painful sensations when swallowing.
- Enlarged lymph nodes.
- Unpleasant sensations when opening the mouth.
- Change in molar color.
Other symptoms also include malaise, fever, weakness, and bleeding. It should be noted that in some cases the inflammatory process can be practically asymptomatic; activation can occur periodically, for example in the case of hypothermia. In this case, immediate assistance from a dentist is required so that he can quickly and accurately diagnose and establish a treatment regimen for effective recovery.
Causes of abscess
Complications associated with the inflammatory-destructive process can occur due to the following reasons:
- Poor quality endodontic treatment.
- Carious formations.
- Injuries to elements of the dentition.
- Unqualified prosthetics.
- Infectious diseases in the maxillofacial area, such as sinusitis.
Treatment of a periapical abscess without a fistula may be required in case of violation of the endodontic therapy protocol or incomplete obturation of the canal system. Provoking factors can be serious infectious diseases, hypothermia, and a reduced level of the body's immune defense. Leukocyte infiltration also often causes the formation of an abscess and microabscess.
Kinds
Based on the nature of the localized accumulation of pus in the elements of the dentition and nearby structures, two groups of abscess are distinguished.
- Periapical abscess without fistula. In this case, transcanal infection of periodontal tissue is observed. The adjacent gum may have swelling, hyperemia is observed, pain is felt when biting on a molar, and the appearance of purulent exudate is recorded. The disease has a pronounced clinical picture.
- Periapical abscess with fistula. With this phenomenon, the inflammatory destructive process spreads to the bone marrow and mucous membrane. The fistula most often opens in the projection of the apex of the root element of the dentition. There may be hyperemia on the mucous membrane, a scar from a fistula, and the gums may be quite sensitive to palpation.
In case of periapical abscess without a cavity and with a cavity, complaints of intense dull throbbing pain, deterioration of general condition, and constant pain are recorded.
Periapical radiographs
Author: Sanjay M. Mallya
Periapical radiographs are the most commonly used in dentistry and show the entire tooth and surrounding bone tissue.
|
Diagnostic purposes of periapical radiography.
For periapical radiography, two intraoral projection techniques are usually used: (1) long-focus parallel beam radiography and (2) contact radiography according to the isometric rule. Both methods can be applied to digital and film images. The long-focus radiography method is preferable because it allows you to obtain images with less distortion of the dentition. When anatomical configuration (eg, palate and floor of mouth) prevents strict adherence to the parallelism concept, minor modifications may be required. If anatomical restrictions are significant, contact radiography principles may be used to position the receiver and determine the vertical angle of the tube.
The term "image receiver" refers to any media used to capture an image, including film, charge-coupled devices, semiconductor metal oxide sensors, or plates containing a phosphor. The principles for creating projection radiographs are the same for each of these types of receivers; thus, this article uses the general term "receiver" to refer to any image receiving system.
Long focal radiography
The basic principle of this technique (also known as parallel beam imaging) is that the beam receiver is positioned parallel to the long axis of the teeth and the central beam of the beam is directed at right angles to the teeth and receiver (Figure 1).
Figure 1. Long-focus radiography is performed with parallelism between the long axis of the tooth and the receiver. The central ray runs perpendicular to both of them. This method minimizes image distortion but requires the use of a positioner.
This orientation of the receiver, teeth, and beam minimizes geometric distortion and represents the teeth and supporting bone in their true anatomical relationships.
Due to anatomical constraints, parallel orientation places the receiver closer to the center of the mouth and further from the teeth. This increases the distance between the object and the receiver and results in larger image magnification and poor geometric contrast. To compensate for the resulting distortion and lack of sharpness when using this method, a sufficiently large distance from the radiation source to the object under study is required (Figure 2).
Figure 2. Graph showing the change in image magnification as the distance between the test object and the receiver changes, using distances between the source and the study object of 20, 30 and 40 cm. Enlarge
Diagnostics
Diagnosis of an acute inflammatory process of infectious etiology with localization in the hilar region includes a visual examination and radiographic examination. In some cases, thermography may be performed. The dentist assesses the condition of the mucous membrane, hyperemia of the tissue, and changes in tooth color. X-ray examination helps to assess the location of the pus. At the diagnostic stage, the specialist determines the viability of the pulp.
A clinical study allows us to determine the degree of pathology and select the correct endodontic treatment or surgical intervention. If necessary, additional examination methods may be required to determine the condition of the periapical tissues. In each specific case, the treatment method is selected individually depending on the history and clinical examination. The patient’s age, local symptoms, and the presence of general diseases are also taken into account. Additionally, microbiological diagnostics can be performed to identify various types of microbial pathogens.
Gum abscess - symptoms and treatment
Gum abscess is caused by pathogens of the oral microflora, which is mainly represented by the following bacteria:
- Bacteroides forsythus (in 55.6% of cases);
- Porphyromonas gingivalis (50.0%);
- Fusobacterium nucleatum (44.4%),
- A. actinomycetemcomitans (38.9%);
- Prevotella intermedia (38.9%) and others.
In addition, in most cases, periodontal pathogens enter into symbiosis with fungi of the genus Candida (44.4%), bacteria Enterobacter (38.9%), Streptococcus intermedius (13.2%), Peptostreptococcus micros (13.2%) and Staphylococcus aureus (28.5%) [4].
The pathogenesis of the disease varies depending on the location of the inflammation.
1. An abscess that arises as a result of pathological processes in periodontal tissues. Inadequate treatment of tooth root canals leads to acute inflammation or exacerbation of its chronic form in the periodontal area. As a result, the number of microorganisms in the tooth root canal and in the periodontal area increases significantly. In response to this, granulation tissue (connective tissue formed during healing) grows in the area of the root apex, replacing bone tissue with it. At the moment of exacerbation of the process, foci of purulent melting of granulation tissue appear in this area. As a result of periodic exacerbation of the inflammatory process, the periodontal lesion gradually spreads to more and more new areas of the bone, mainly towards the vestibule of the oral cavity. This leads to the appearance of vertical slit-like defects of the cortical plate and the further development of first infiltration in the gum area, and then the appearance of an abscess [5].
2. An abscess that has arisen in the area of the periodontal pocket. Periodontal gum abscess occurs as a result of several interrelated pathological processes. A large amount of supra- and subgingival dental plaque promotes the development of periodontal pathogenic bacteria, which causes a strong immune reaction. The body responds by forming an infiltrate with a large number of immune system cells. These cells produce inflammatory mediators that stimulate the destruction of bone tissue by osteoclasts (cells that remove bone tissue by dissolving mineral content and breaking down collagen). The bone tissue begins to dissolve and a periodontal pocket is formed, which, depending on the severity of periodontitis, has different depths. At the time of exacerbation of periodontitis, suppuration from the periodontal pocket becomes continuous. If the outflow is disrupted, abscess formation occurs [6].
3. An abscess that has arisen in the area of peri-implant tissue. The cause of the development of peri-implantitis is microorganisms located in the biofilm on the surface of the structure. Colonies of microorganisms affect the soft tissue surrounding the implant, causing inflammation. Further, the process develops in the same way as with periodontitis, but does not remain localized, but spreads towards the apex of the implant. In peri-implantitis, the inflammatory infiltrate passes directly to the alveolar bone, while in periodontitis it is separated from the bone by a one-millimeter layer of connective tissue. At the early stage of peri-implantitis, an abscess occurs at the level of the upper third of the implant - in the area of the peri-implant pocket. At later stages, as the bone in the area of the implant body is destroyed, it can move closer to the transitional fold of the gums[7].
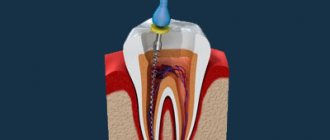
Treatment of periapical abscess
Depending on the stage and form of the pathology, the specialist selects a therapeutic or surgical method of treatment. At the initial stage, the canals are usually cleaned, in particular the elimination of pathogenic microflora between the teeth and gums, and the cavity is treated with antibacterial components. Endodontic therapy may include the installation of a temporary filling and the application of an antiseptic dressing with antimicrobial properties in the root canal. Antibiotics may be prescribed to stop the inflammatory process.
High-quality endodontic therapy allows you to eliminate the infectious focus. As inflammation increases, an element of the dental system can be removed. In some cases, the specialist performs appropriate tooth-preserving procedures, for example, hemisection, that is, removal of one of the molar roots.
The opening of an abscess is always performed using anesthesia; discomfort and pain are excluded during high-quality endodontic treatment. After the abscess removal procedure, drug therapy and surface treatment with special bactericidal compounds may be prescribed. The final step is to take an x-ray to ensure complete recovery.
The specialists of the AlphaDent clinic are always ready to help if you have complaints about a periapical abscess without a fistula or with a fistula. Dentists have the necessary knowledge and sufficient experience to provide high-quality endodontic treatment.
Qualified treatment will eliminate the recurrence of the infection that caused the abscess. Timely dental care will help keep your teeth and mouth in good condition. It is recommended to make visits to the dentist for preventive examinations in order to exclude complex endodontic treatment associated with the removal of an abscess.
Diagnosis and treatment
The doctor begins the diagnosis with a general examination. An abscess may appear as a small, red and inflamed lump. The fistula may ooze pus. To determine the size of the tumor, a picture is taken. It also eliminates damage to periodontal and bone tissue.
The first stage of treatment is always the removal of purulent contents. If the fistula is not open, the doctor makes an incision in the gum and installs a drain to ensure the drainage of pus. The next step is opening the tooth cavity. The doctor removes the dead pulp and performs root canals to reduce the risk of relapse. When the inflammation is stopped, the tooth is filled.
If treatment is not possible, the doctor will remove the affected tooth and then clean the capsule of purulent contents. Following treatment or removal, you must take prescribed antibiotics to reduce the risk of infection spreading.