Most often, a sore throat is associated with viral inflammation, which is accompanied by fever, cough, runny nose and minor difficulty swallowing. But, unfortunately, in some situations these diseases can be complicated by the development of purulent-inflammatory complications, for example, peritonsillar abscess, and the task of the ENT doctor at the present stage is the correct diagnosis of this complication and timely treatment, because this complication does not tolerate deposits and is fraught with more significant spread of infection into the deep tissues of the neck. At the GMS Hospital Otolaryngology Center, a comprehensive approach is used to treat peritonsillar abscesses, combining conservative and surgical techniques.
More about the disease
Peritonsillitis is an acute condition secondary to tonsillitis or tonsillopharyngitis, which results in the penetration of an infectious agent (bacteria) into the loose peritonsillar tissue (peritonsillar space). The process is always one-sided, as a result of which it has certain symptoms:
- pain or increased pain on one side;
- severe difficulty swallowing;
- swelling and bulging on the neck on one side;
- asymmetry and bulging of pharynx tissues.
A peritonsillar abscess occurs when a cavity filled with pus forms, located in the peritonsillar (peritonsillar) tissues.
It can form several days after the development of a sore throat or an exacerbation of tonsillitis. Less commonly, due to traumatic injury to the oropharynx or penetration of a foreign body into the tissue around the tonsils. In people with a weak immune system, an abscess can form within a day. It is more often unilateral, but cases with bilateral paratonsillar abscess have been reported in the literature. This pathology is one of the most severe purulent lesions of the oropharynx. With further spread, the infection moves into the deep tissues of the neck (parapharyngeal space), which can lead to a life-threatening condition. Depending on their location, there are several forms of peritonsillar abscess, but all of them require surgical treatment.
The Surgical Otolaryngology Center at GMS Hospital provides proper treatment and diagnosis of paratonsilitis and paratonsillar abscess of any form. Treatment tactics are selected by specialists individually, depending on the stage of the disease, the presence of complications and concomitant pathologies.
General information
Peritonsillar abscess (synonyms - paratonsillitis , phlegmonous tonsillitis ) is one of the nosological forms of purulent-inflammatory diseases of the pharynx, which differs from other forms (parapharyngeal and retropharyngeal abscess) in the prevalence of the pathological process and anatomical and topographic localization.
A peritonsillar abscess is an acute inflammatory and purulent manifestation in the area of the peritonsillar tissue. ICD-10 code for paratonsillar abscess: J 36. In most cases, tonsillar abscess is secondary, that is, a complication of chronic tonsillitis/acute catarrhal, lacunar or follicular tonsillitis . Much less often, it can be an independent disease (primary), developing as a result of an odontogenic process, trauma to the pharynx by a foreign body, or with chronic obstruction of the nasal cavities (adenoiditis).
Pathogenic microflora penetrates into the paratonsillar tissue mainly by contact from the enlarged, altered and branching lacunae of the tonsils through damaged (melted/necrotic) capsule tissue. That is, a purulent abscess in the throat (peritonsillar abscess/peritonsillitis) is a consequence of the transition of an acute infectious-inflammatory process from the palatine tonsils directly to the peritonsillar tissue and adjacent tissues, which is characterized by unilateral/bilateral inflammatory infiltration. The infectious-inflammatory process in loose connective tissue involves the buccal-pharyngeal fascia, as well as the upper pharyngeal constrictor with fascia. In most cases, there is a unilateral abscess; bilateral lesions occur only in 7-10% of cases.
Peritonsillar abscesses are the most common and severe disease among all purulent processes of the pharynx. It occurs in people of all ages, but people aged 15-40 years are more likely to get sick. No gender differences were found. The development of the disease is characterized by seasonality: it is more often observed in the off-season/cold season. Acute paratonsillitis occurs less frequently in the summer, mainly in cases of sudden local hypothermia - ice cream, cold drinks, swimming in cold water, etc.
Why is it necessary to open and drain a peritonsillar abscess?
Peritonsillar abscess is an urgent condition in otolaryngology. The proximity of vital structures (windpipe, large vessels of the head and neck) requires immediate diagnosis and treatment. In the initial stages, when an abscess has not yet formed, the pathology responds well to drug therapy. A course of antibiotic therapy, anti-inflammatory and painkillers is prescribed. If conservative treatment is ineffective, the abscess is opened surgically.
Peritonsillar abscess is dangerous due to its complications, fraught with the development of phlegmon, mediastinitis and even sepsis. The Otolaryngology Department at the GMS Clinic has everything you need to accurately diagnose and treat peritonsillar abscesses.
The opening of the abscess is carried out using modern surgical equipment. During the operation, the potential of laser and radio wave surgery is actively used, which allows the procedure to be performed in the most gentle manner, eliminating the development of surgical complications. Opening abscesses in children is performed under anesthesia, which significantly increases the comfort of the intervention.
Causes of PTA
The disease rarely occurs independently and is often a complication of purulent tonsillitis or chronic tonsillitis. It develops when pathogenic flora penetrates the tissues of the palatine tonsils. The inflammatory process is provoked by:
- bacterial lesions against the background of Staphylococcus aureus, streptococci, Escherichia coli, Haemophilus influenzae, Klebsiella. A throat abscess occurs when a sore throat worsens. In some cases, the disease can develop without a previous infection of the pharynx with blockage of the salivary glands. Often paratonsillitis or paratonsillar abscess is preceded by acute tonsillopharyngitis;
- dental diseases. These include periostitis of the alveolar processes, gingivitis, caries, etc. They often cause peritonsillar abscess in children;
- injuries. The disease occurs through contact. Violation of the mucous membrane provokes infection of the area.
Cost of treating peritonsillar abscess
The prices indicated in the price list may differ from the actual prices. Please check the current cost by calling +7 495 104 8605 (24 hours a day) or at the GMS Hospital clinic at the address: Moscow, st. Kalanchevskaya, 45.
| Name | Price |
| Opening of the epiglottis abscess | RUB 54,999 |
| Opening abscesses, phlegmon of the laryngopharynx | RUB 64,995 |
| Opening a paratonsillar or retropharyngeal abscess | RUB 46,998 |
| Drainage of peritonsillar abscess | RUB 24,997 |
| Tonsillectomy + removal of peritonsillar abscess (According to Quinzey) | RUB 189,994 |
Dear Clients! Each case is individual and the final cost of your treatment can only be found out after an in-person visit to a GMS Hospital doctor. Prices for the most popular services are indicated with a 30% discount, which is valid when paying in cash or by credit card. You can be served under a VHI policy, pay separately for each visit, sign an agreement for an annual medical program, or make a deposit and receive services at a discount. On weekends and holidays, the clinic reserves the right to charge additional payments according to the current price list. Services are provided on the basis of a concluded contract.
Plastic cards MasterCard, VISA, Maestro, MIR are accepted for payment. Contactless payment with Apple Pay, Google Pay and Android Pay cards is also available.
Western standards of treatment (evidence-based medicine)
Continuous staff development
Regular interaction with leading Russian and foreign medical institutions
Modern medical equipment and advanced diagnostic and treatment methods
Unified standard of service
We work around the clock 24/7/365
Make an appointment We will be happy to answer any questions Coordinator Oksana
Prevention
Prevention of paratonsillar abscess is based on timely and adequate treatment of acute tonsillitis and exacerbations of chronic tonsillitis with a full course of antibacterial therapy. In cases of a chronic course with frequent (3 or more times a year) exacerbations, an effective preventive measure (in the absence of contraindications) is timely tonsillectomy .
Individual prevention includes:
- Strengthening the body's overall resistance, increasing resistance to the effects of adverse external conditions (infectious factors, weather conditions) through local/general hardening (air/sunbathing, outdoor exercise, shower/rubbing/foot baths with a gradual decrease in water temperature).
- Correct work/rest schedule.
- Regular/timely sanitation of the oral cavity (for chronic gingivitis , carious teeth ) and nose.
- Balanced diet.
- Correction of immunodeficiency states.
- Quitting alcohol abuse/smoking.
Signs and symptoms of paratonsillitis
The disease has an abrupt onset. An abscess forms a few days after an exacerbation of tonsillitis or the onset of a sore throat and is accompanied by vivid symptoms:
- acute pain in the throat, radiating to the jaw or ear;
- sensation of a “lump” in the throat;
- fever (temperature 39-40°C);
- submandibular lymph nodes are greatly enlarged;
- difficulty swallowing (even drinks);
- the appearance of a repulsive odor from the mouth;
- neck pain that gets worse with exercise;
- general weakness;
- inability to fully open the mouth;
- headache;
- speech impairment (voice as if there is a hot potato in the mouth);
- difficulty breathing (with large ulcers).
Spontaneous breakthrough of suppuration into the throat cavity is accompanied by an improvement in well-being and the appearance of an admixture of pus in the saliva.
The spread of the abscess contents into the peripharyngeal space significantly worsens the condition, so there is no need to delay operations to open the abscess. If you have even one of the symptoms listed above, schedule a consultation with an otolaryngologist today. Doctors at the Center for Operative Otolaryngology at GMS Hospital use gentle microsurgical techniques, which contributes to a speedy recovery and the absence of relapses of the disease.
Clinical picture
There is pain in the throat, which increases with swallowing, turning the head and coughing.
The patient experiences difficulty opening his mouth, which is accompanied by severe pain. Trismus (inability to fully open the mouth) of the masticatory muscles is noted. The patient is forced to refuse to eat and drink, the pain interferes with his normal sleep. Body temperature is elevated, patients complain of weakness and malaise. When performing pharyngoscopy, hyperemia (pronounced redness) of the mucous membrane and infiltration of one half of the soft palate and palatine arches on the affected side are determined.
The palatine tonsil is slightly shifted to the healthy side and is tense. The lymph nodes located under the jaw and on the neck become somewhat swollen. Due to the fact that the soft palate is almost motionless, the voice becomes nasal. The most common are peri-almond abscesses with anterior and upper anterior localization.
Diagnostics
For the differential diagnosis of paratonsillitis, the following research methods are used:
- examination by an otolaryngologist;
- laryngoscopy;
- pharyngoscopy;
- laboratory tests (blood tests, culture for flora and sensitivity to antibiotics, etc.).
In some cases, to clarify the diagnosis, additional studies are performed - ultrasound, CT scan of the soft tissues of the head and neck.
A comprehensive examination allows you to assess the condition of the abscess and tonsil, determine treatment tactics and the scope of intervention. You can complete all the required tests at the GMS clinic in a day.
Tests and diagnostics
The diagnosis is made on the basis of typical clinical symptoms, the results of a physical examination and mesopharyngoscopy (asymmetry of the pharynx, swelling/hyperemia of the peritonsil tissue (arches, uvula, soft palate), protrusion of the palatine tonsil from the tonsillar niche and its displacement to the midline)). In detailed clinical tests - an increase in the level of ESR and leukocytes in the blood.
Differential diagnosis with other purulent-inflammatory nosological forms of the pharynx (parapharyngeal and retropharyngeal abscess) is important. Thus, a retropharyngeal abscess is characteristic mainly of young children, the cause of which is most often adenoiditis / acute tonsillitis . It is quite rare in adults. In addition to differences in the location of the abscess, there are no symptoms characteristic of peritonsillar abscess in adults - there is no severe pain in the throat and trismus. When pharyngoscopy - a purple protrusion to the right/left of the midline of the posterior wall of the pharynx, when palpated with a spatula - fluctuation, the tonsils and palatine arches are intact, white ulcers on the tonsils may be present.
Treatment methods
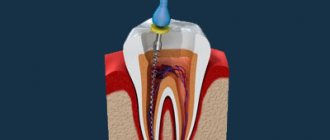
The treatment tactics for paratonsillitis depend on the extent of the spread of the purulent process and the presence of complications. Peritonsillitis in the initial stage is treated conservatively, with antibiotics, decongestants, painkillers and anti-inflammatory drugs. If drug treatment is ineffective or an abscess forms, the abscess is surgically opened and its cavity is drained. The opening of the paratonsillar abscess is carried out under local anesthesia. The otolaryngologist dissects the wall of the abscess, removes the purulent contents, and rinses the cavity with an antiseptic. An improvement in the condition is observed immediately after opening and draining the abscess.
You have questions? We will be happy to answer any questions Coordinator Tatyana
Treatment
For peritonsillar abscess, surgical intervention is indicated.
The opening of the abscess is performed through the anterior palatine arch, moving 1-1.5 cm outward from the free edge in the place where the greatest softening and protrusion is observed. If it is very difficult to determine the location of the softening, it is recommended to make an incision in the middle of the line that connects the last molar and the base of the tongue. The mucous membrane is treated with an anesthetic and an incision is made with a scalpel at the site of the greatest bulging of the infiltrate, no more than 1 cm long. Using a forceps, the soft tissues are moved apart to a depth of 1 to 2 cm. After the abscess is opened, treatment is prescribed, the same as for follicular and lacunar angina. If a person has suffered a peritonsillar abscess, then this is an indication for surgery to completely remove the tonsils (bilateral tonsillectomy).
Make an appointment right now!
Call us by phone or use the feedback form
Sign up
Surgical treatment of this disease is complemented by drug therapy, which includes all the components used in the treatment of paratonsillitis.
If paratonsillar abscesses often recur or paratonsilitis does not resolve for a long time (does not go away), then abscessonsillectomy is performed (complete removal of the tonsils).
Prevention of paratonsillitis
The following simple preventive measures will help prevent the development of peritonsillar abscess:
- strengthening the immune system;
- healthy lifestyle;
- timely treatment of acute and chronic diseases of the ENT organs (sinusitis, adenoids, pharyngitis, tonsillitis, etc.), caries;
- rejection of bad habits.
In the presence of recurrent abscesses, elective tonsillectomy is recommended.
Opening a peritonsillar abscess at the GMS clinic is a simple and safe surgical procedure that is performed in an outpatient or inpatient setting. Recovery takes 10-14 days, after which you will return to your normal life. You can make an appointment with an otolaryngologist at GMS Hospital by phone or using an online application.
Types and forms of PTA
Depending on the location of inflammation, there are:
- anterior paratonsillar abscess. In most clinical cases, pus accumulates near the upper pole of the tonsil, behind the anterior arch and soft palate;
- lateral paratonsillar abscess. Exudate forms between the pharyngeal fascia and the tonsil capsule. There are right-sided and left-sided PTA;
- posterior abscess. Pus accumulates in the posterior arch area. Pathology can provoke swelling of the larynx with subsequent stenosis;
- lower PTA. Rarely seen. In this case, the anterior palatal arch is displaced downwards from the front due to infiltration of the lower part.
Peritonsillar abscess has the following clinical and morphological forms:
- edematous. It occurs without significant inflammation without significant manifestations of symptoms. Because of this, the form of the disease is rarely diagnosed;
- infiltration Hyperemia occurs. Manifested by pain, fever;
- abscessing. Forms 4-7 days after the development of infiltration changes.
Pathophysiology
Purulent tonsillitis, as a rule, begins with the onset of acute follicular tonsillitis, progresses to paratonsillitis and leads to the formation of a paratonsillar abscess.
An alternative theory involves the Weber's glands, which are a group of salivary glands located directly above the tonsillar region in the soft palate. These glands are thought to play a minor role in clearing the tonsil area of any “garbage” that has accumulated there. Tissue necrosis and pus formation lead to the formation of an abscess between the tonsil capsule, the lateral wall of the pharynx and the peritonsillar space. As a result of scarring and obstruction of the excretory ducts, pus accumulates in the tissues and the formation of a purulent abscess progresses.
What is an abscess and how does it develop with sore throat?
An abscess with tonsillitis begins with inflammation that affects the tissue around the tonsils of the palate and lymph nodes, during which suppuration occurs. Its formation is due to the presence of several bacterial pathogens, consisting of streptococcal, staphylococcal, fungal or anaerobic and aerobic pathogens of phlegmous sore throat, which can lead to the development of pyogenic microorganisms. After the incubation period, the catarrhal process turns purulent and an extensive paranthosillar abscess begins. In addition, the disease often progresses due to the presence of chronic sinusitis, rhinitis or otitis in the body.
Abscesses can form not only around the tonsils, but also in the tongue, tubal tonsils or nasopharyngeal system.
They often arise as a result of dangerous hypothermia during an illness or frequent relapses, when the tissue of the tonsils is still fragile and inflamed. In rare cases, suppuration can begin after diseases such as influenza, scarlet fever, ARVI, measles, periostitis, neck injuries or purulent inflammation of the teeth and salivary glands.
The pathology occurs due to the structural features of the tissues of the tonsils, when an excess amount of blood enters the capillaries and swelling begins, and the crypts of the tonsils are filled with purulent discharge, most often in the upper part of the palate. There are several varieties, each of which has an individual development pattern.
- Lower - affects the fiber located between the tonsils of the tongue and palate, behind the lower third of the palatine arch. With an odontogenic cause, the development remains a rare type of abscess.
- Posterior - complicated by edema of the pharyngeal system and breathing problems, manifests itself mediocrely in patients of different ages in a ratio of 1:10.
- Supratonsillar - pus spreads to the tonsils and surrounding tissue, accumulating due to poor outflow, and is the most common type of suppuration.
- Lateral is the most severe form of the disease, due to the likelihood of microflora spreading to the pharyngeal area. Formed after mechanical damage or as a result of infection.
- Peri-almond is a complication due to tonsillitis with the participation of various bacterial microorganisms that greatly aggravate the pathology due to decreased immunity and scarring on the surface of the tonsils.
- External - pathology affects the surface of the tonsils and is very rare in medical practice.
People suffering from diseases such as immunodeficiency, anemia, diabetes mellitus or people with a predisposition to oncology are in the primary risk group for the development of severe pathological conditions of tonsillitis. There are no anatomical reasons for the development of an abscess, so the therapist, when treating, always focuses on the accompanying symptoms.
Causes of tonsillitis abscess
Among the causes of the disease will be the following.
- Untreated tonsillitis, the tonsils in this period have not yet become stronger, they have scars, the tissues around the tonsils are loose and inflamed. When anaerobic or aerobic bacteria enter, the process of suppuration begins.
- Too frequent follicular sore throats can also cause an abscess.
- Frequent, severe hypothermia, causing a decrease in immunity. They are especially dangerous during acute tonsillitis.
- The presence in the throat area of other chronic infections of the ear, nasopharynx, and teeth, which during a sore throat can cause suppuration.
- Poor sanitation of the inflamed oral cavity (infrequent rinsing, lack of treatment of inflamed tonsils).
Opening a hematoma (abscess) of the nasal septum
Traumatic injuries to the nose are often accompanied by external bleeding of varying degrees of intensity, which stops on its own or with the help of nasal tamponade. With normal blood clotting and the absence of severe concomitant pathology, bleeding is not dangerous and the body very quickly compensates for this blood loss.
It is very important to monitor a patient with a nasal injury in the first days after the injury, since complications in the form of a hematoma of the nasal septum and its subsequent abscessation are possible. According to statistics, in 1 out of 100 cases of nasal injuries we encounter such complications. Considering the abundant blood network in the nasal cavity and the direct connection with the vessels of the brain, the high importance and timeliness of the primary diagnosis of these nasal diseases for the prevention of serious intracranial complications becomes obvious.
Causes of hematoma of the nasal septum
The immediate cause of a hematoma of the nasal septum is a trauma to the nose, which results in damage to the vessels of the perichondrium in the cartilaginous part of the nasal septum and hemorrhage into the cavity between the mucous membrane of the nasal cavity and the cartilage. Predisposing factors are disorders of the blood coagulation system, acute respiratory diseases, in which a hematoma of the nasal septum can appear even with the slightest trauma to the nose.
Symptoms of nasal septum hematoma
The main and first symptom of the development of a hematoma of the nasal septum is difficulty in nasal breathing, which develops several days after the injury to the nose, on one or both sides, increasing in intensity every day. The addition of a headache, increased body temperature, and malaise indicate the addition of pathogenic microflora and the formation of an abscess of the nasal septum.
Diagnosis of nasal septum hematoma
Due to the high risk of developing intracranial complications, diagnosis of nasal septum hematoma and its possible abscess formation should be timely and based on characteristic complaints, medical history and rhinoscopy data.
Treatment of nasal septum hematoma
Treatment of hematoma of the nasal septum consists of emptying the hematoma cavity, leaving drainage and tamponade of the nasal cavity on both sides for 1-2 days. General treatment consists of prescribing antibiotics and hemostatic agents for changes in hemostasis. In case of an abscess of the nasal septum, the abscess is opened and emptied, drainage is introduced into the abscess cavity and systemic antibiotic therapy is performed.
As a rule, with timely diagnosis and adequate treatment, recovery occurs within 5-7 days.
The ENT Clinic in Chertanovo provides comprehensive care to patients after nasal injuries complicated by the development of a hematoma of the nasal septum and its abscess formation.
Opening an abscess (furuncle) of the ear
Ear boil is a purulent-inflammatory disease of the hair follicle of the skin of the auricle and external auditory canal.
The cause of an ear boil is microtrauma when scratching or cleaning the ear with a cotton swab or foreign objects (matches, pins, etc.). Pathogenic microflora settles on the injured surface of the skin of the external auditory canal and an inflammatory process develops. This is facilitated by water getting into the ear, metabolic disorders that change the barrier function of the skin (diabetes, obesity), decreased immunity, unfavorable ecology and environmental factors (air pollution, working in a dusty room, etc.).
The development of the disease goes through several stages:
- infiltrative,
- abscess formation and necrosis,
- recovery
The disease is characterized by diffuse pain in the affected ear, aggravated by chewing, talking, and opening the mouth. Due to swelling of the skin of the external auditory canal, its lumen narrows until there is no lumen at all. This leads to a feeling of ear fullness and decreased hearing on the affected side, since sound waves cannot be carried to the eardrum and transmitted along the chain of auditory ossicles to the inner ear. Upon examination, the skin of the external auditory canal is hyperemic and swollen; at the stage of abscess formation, an area of necrosis with a purulent core can be seen. As a rule, regional lymph nodes are involved in the process, enlarging and causing pain upon palpation. Depending on the stage of the disease and the extent of damage to the skin of the external auditory canal, the clinical picture may be limited only to local manifestations, or accompanied by symptoms of general intoxication - high fever, weakness, malaise, headache.
Diagnosis of an ear boil
Diagnosis of an ear boil is not difficult; it is enough to collect an anamnesis, the patient’s characteristic complaints and examine the external auditory canal using an otoscope or endoscope.
Treatment of ear boil
Treatment for ear boils depends on the stage of the disease. At the infiltration stage, local alcohol applications (calendula solution, chamomile, iodine tincture), oral antibiotics, antiplatelet agents (aspirin) to prevent thrombosis, and antihistamines are prescribed. If it was possible to start treatment in the first hours or day of the disease, then the process is localized and quickly resolves without a stage of suppuration. It should be remembered that self-medication and independent attempts to open an abscess threaten the development of serious complications, including death.
Opening a boil in the ear
In the stage of suppuration and necrosis, it is recommended to open the boil and drain its cavity, rinse with antiseptic solutions, continuing active general therapy.
In the resolution stage, a good therapeutic effect is achieved by the use of physiotherapeutic procedures, such as ultraviolet irradiation of the affected area, laser therapy or photochromotherapy.
Doctors at the ENT Clinic in Chertanovo carry out the full range of necessary treatment measures for patients with ear boils, selecting an individual treatment regimen and choosing certain techniques based on the stage of the disease, the patient’s age, duration of the disease and concomitant pathology. After opening the boil, it is possible to conduct detoxification therapy and monitor the patient in a day hospital. During the recovery stage, patients undergo laser treatment or photochromotherapy of the external auditory canal in order to improve the regeneration process of the skin of the external auditory canal and prevent relapses in the future.
After recovery, it is necessary to conduct an examination for concomitant conjugate, hidden pathology to prevent the occurrence of boils in the future, since in the absence of treatment of the underlying disease, frequent relapses of the disease are possible.